
Abstract
The aim of the present study was to assess atypical changes in urothelial cells among petroleum station workers. This is a case control study, investigating 300 participants by cytological methods. Of the 300 participants, 150 were cases (exposed to petroleum products) and 150 were controls (non-exposed). Full voided urine was obtained and was cytologically assessed. Cytological atypia was identified in nine (6%) out of the 150 cases and could not be identified in 141/150 (94%) of the cases, whereas, in the control group, cytological atypia was recognized in four (2.7%) of the 150 controls and could not be identified in 146/150 (97.3%). The risk associated with petroleum product exposure, the odds ratio (OR), and 95% confidence interval (CI) was 2.33 (0.7015–7.7378), P = 0.1673. Exposure of petroleum station workers to petroleum products increases the risk of urothelial atypical changes, which may progress to precancerous and cancerous changes.
Introduction
The most common petroleum product in petroleum stations are benzene and gasoline. Recently an International Agency for Research on Cancer (IARC) Working Group determined that there was adequate evidence in humans for the carcinogenicity of diesel exhaust (Group 1). In addition, the Working Group found that diesel exhaust has “a positive association (limited evidence) with an increased risk of bladder cancer.” Like most other carbonaceous fuel emissions, diesel and gasoline exhausts contain toxic levels of respirable particles (PM <2.5 μm) and polycyclic aromatic hydrocarbons. 1 Aromatic hydrocarbons such as benzene, toluene, ethylbenzene, and xylene (collectively labeled BTEX) are natural constituents of the petroleum stream and exposure to these agents gives rise to many cancers.2–4
However, several epidemiological studies have been performed to investigate the association between occupation and bladder cancer incidence. These studies delivered reliable support for a small but significant increased risk of bladder cancer among petroleum workers. Although the relative risk of bladder cancer associated with these occupations is small, the public health impact may be significant, in view of the substantial number of people who were and are employed in petroleum-related occupations. 5
Bladder cancer is one of the most frequently diagnosed malignancies worldwide, derived from the urothelial cells of the urinary bladder. There are several risk factors contribute to etiology of bladder cancer which can be categorized into three groups: genetic and molecular abnormalities; chemical or environmental exposure; and previous genitourinary disorders and family history of different malignancies. Various genetic polymorphisms and microRNA might represent useful diagnostic or prognostic biomarkers. 6 Many methods have been introduced for the early detection and diagnosis of bladder cancer. The typical methods for the detection and screening of bladder cancer involves cytology and cystoscopy, but both examinations suffer from many limitations, including issues related to accuracy, invasiveness, and cost. Several non-invasive methods for detection and surveillance of bladder cancer are now available and urine-based biomarkers appear to be the most promising. 7
However, the advanced methods for diagnosis of bladder cancer might not be suitable for the screening of apparently healthy individuals. Cytology seems to be the most practical methods for screening and early detection since it is a non-invasive and cheap method. Therefore, in this study we used cytology to assess urothelial cells atypical changes among petroleum station workers.
Materials and methods
In this prospective case-control study, 300 volunteers living in the city of Hail, Kingdom of Saudi Arabia (KSA) were randomly (blinded) selected for this study and asked to take a urine self-sample. Of the 300 participants, 150 were petroleum station workers (ascertained as the case group) and 150 were non-petroleum exposed individuals (ascertained as the control group). All of the study population were men and apparently healthy. Tobacco smokers were excluded from both cases and controls. Since we were interested in cell morphology, the exclusion criterion was no history of bladder and/or kidney disease.
Fresh voided urine specimens were collected from each participant and immediately prepared. Each urine sample was placed in a sterile container and immediately centrifuged (at 1500 rpm for 10 min) and the deposit was smeared onto a cleaned glass slide. Each smear was immediately fixed while it was wet in 95% ethyl alcohol for 15 min and eventually stained adopting Papanicolaou procedure (Pap. stain). Ethyl alcohol fixed smears were hydrated in descending concentrations of 95% ethyl alcohol, through 70% alcohol to distilled water, for 2 min in each stage. The smears were then treated with Harris’ hematoxylin for 5 min to stain the nuclei, rinsed in distilled water, and differentiated in 0.5% aqueous hydrochloric acid for a few seconds, to remove the excess stain. Then the smears were blued in running tap water for 5 min and dehydrated in ascending alcoholic concentrations from 70%, through two changes of 95% alcohol for 2 min for each change. The smears were then treated with Eosin Azure 50 for 4 min. For cytoplasmic staining, they were treated with Papanicolaou Orange G6 for 2 min, rinsed in 95% alcohol and then dehydrated in absolute alcohol. The smears were then cleared in Xylene and mounted in DPX (Distrene Polystyrene Xylene). All the reagents used were from Thermo Electron Corporation, UK. All quality control measures were implemented all over the study procedures. Smears were first examined by light microscope at ×10 followed by ×40. For assessment of morphological changes and the degree of the quality of the staining, each smear was assessed for quality sufficiency and cellular adequacy. Only stained smears that showed fair staining quality were assessed. For cytological assessment, each slide was assessed for its level of preservation and degeneration by two cytology screeners in a blinded fashion. To reduce the bias, the smears were re-indexed in such a way so that the examiner did not know the cases and controls; three independent examiners then screened the smears.
Assessment of cytological atypia
Cytological atypia was assessed adopting criteria described by Ahmed et al., 8 the presence of two or more of the following features indicated the presence of epithelial atypia: nuclear enlargement associated with increased nuclear cytoplasmic ratio, hyperchromatism, chromatin clumping with moderately prominent nucleolation and irregular nuclear borders, bi- or multinucleation, increased keratinization and scantiness of the cytoplasm, and variations in size and/or shape of the cells and nuclei. Moreover, the degree of epithelial atypia was assigned by adopting criteria described elsewhere. 9 Smears previously prepared from patients with bladder cancer were included as internal control (Photomicrograph 1).

Pap. stained urine smear showing atypical urothelial cells, 400×. The smear was obtained from a known patient with bladder cancer (internal control).
Data analysis
SPSS version 16 statistical software was used for Statistical analysis. The 95% confidence level was used. The Chi-square test was used to compare the differences in categorical variables between the groups. Relationships between variables were analyzed using Friedman’s non-parametric test. A P value <0.05 was considered statistically significant.
Ethical consent
Each participant was asked to sign a written ethical consent form during the interview, before the obtaining of the sample. The informed ethical consent form was designed and approved by the College of Applied Medicine, University of Hail, KSA.
Results
This study investigated 300 men (150 cases, 150 controls; age range, 20–50 years; mean age, 31 years). Cytological atypia was identified in nine (6%) of the 150 cases and could not be identified in 141/150 (94%) of the cases, whereas in the control group, cytological atypia was recognized in four (2.7%) of the 150 controls and could not be identified in 146/150 (97.3%). The risk associated with petroleum product exposure, the odds ratio (OR) and 95% confidence interval (CI) was 2.33 (0.7015–7.7378), P = 0.1673 (Photomicro-graphs 2–5).

Pap. stained urine smear showing a group of normal urothelial cells, 400×. Smear was obtained from non-petroleum station worker.
Pap. stained urine smear showing normal urothelial cells with scant inflammatory cells infiltrate, 400×. Smear was obtained from non-petroleum station worker.

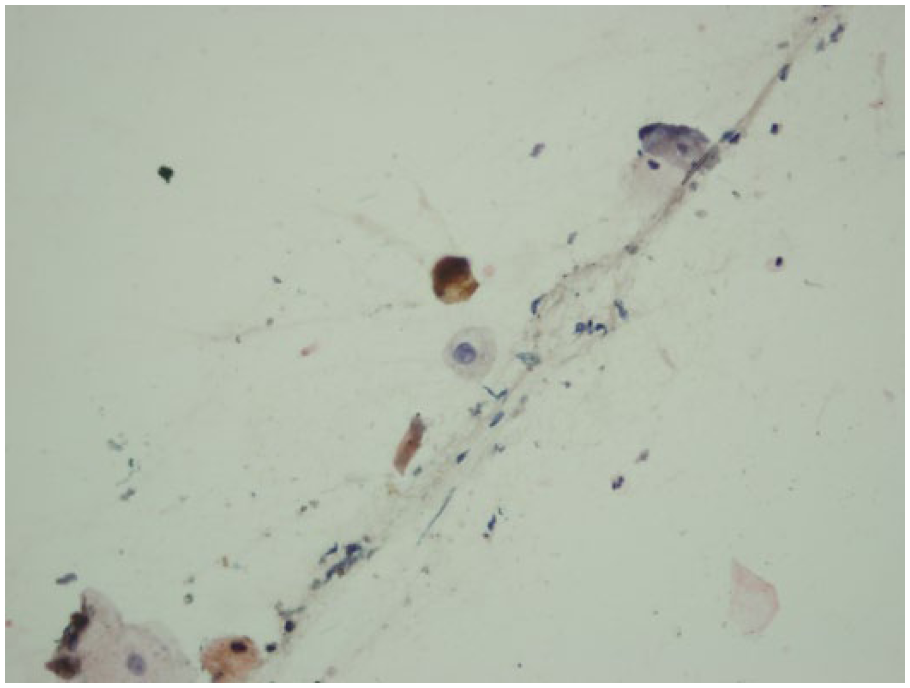
Pap. stained urine smear showing atypical urothelial cells with acute inflammatory cells infiltrate, 400×. The smear was obtained from a petroleum station worker of 10 years.

Pap. stained urine smear showing atypical urothelial cells with dense inflammatory cells infiltrate, 400×. The smear was obtained from a petroleum station worker of 11 years.
Acute inflammatory cell infiltrates (including polymorph nuclear and monocytes) were found among 6/150 (4%) and could not be found among 144/150 (96%). For controls, acute inflammatory cells were found among 10/150 (6.7%) and could not be found among 140/150 (93.3%). The risk of acute inflammatory infiltrate was inversely associated with exposure in petroleum stations, the OR and 95% CI were 0.58 (0.2065–1.6480), P = 0.3090 (Photomicrographs 4 and 5).
Chronic inflammatory cells (including lymphocytes, plasma cells, and macrophage) were found among 12/150 (8%) of the cases and could not be found among 138/150 (92%). For controls, chronic inflammatory cells were found among 3/150 (2%) and could not be found among 147/150 (98%). The risk of chronic inflammatory infiltrate was significantly associated with exposure in petroleum stations, the OR and 95% CI were 4.26 (1.1772–15.4221), P = 0.0272, as indicated in Table 1 and Figure 1.
Distribution of the study participants by cytological findings.


Description of the study participants by cytological findings.
The distribution of cytological findings in the cases by age and duration of exposure in petroleum stations was summarized in Table 2. Most of the cases with cytological atypia were identified among the age group 36–45 years followed by 26–36 years, representing five and four cases, respectively. With regard to chronic inflammatory cells infiltrates, the condition was predominantly revealed among the age group 26–35 years, constituting seven cases followed by the age ranges 36–45 years and <25 years representing four and one cases, respectively.
Distribution of the cases by cytological findings and age and duration of exposure.

For duration of exposure to petroleum products, the great majority of the cases with atypia were identified in <5 years’ duration representing five cases, followed by 6–10 years’ duration constituting four cases. With regard to chronic inflammatory cells infiltrates, the condition was similarly found in durations of <5 years and 6–10 years constituting six cases each, as shown in Figure 2.

Description of the cases by cytological findings and age and duration of exposure.
Discussion
Saudi Arabia has traditionally been considered as the world’s most important swing producer of oil. 11 This high product of petrol is reflected in the low price of petroleum products within the country and high density of petroleum stations in all parts of KSA. These countless petroleum stations involve the employment of thousands of workers. It was observed that the great majority of these workers are exposed to air pollution with petroleum products, particularly benzene, without any protective tools. Benzene, formaldehyde, and acetaldehyde are carcinogenic elements to which gasoline station workers are most likely exposed to via inhalation. 12
However, in the present study we aimed at evaluating the burden of such exposure through assessment of urothelial atypical cytological change. Although, the presence of atypia among cases was statistically insignificant, the risk associated with exposure was relatively high. Such findings were previously reported.13,14 Petroleum products contain a variety of aromatic amines that are considered potential causes of bladder cancer. It was suggested that when individuals are exposed to both aromatic amines and tobacco smoke interaction occurs (statistically insignificant); risk considerably increases when both exposures occur versus either exposure alone. 15 Comparable interactions were also seen with exposure to smoking and polycyclic aromatic hydrocarbons (PAHs) and smoking and diesel exhaust. 16 Another study also investigated the interaction of the previously mentioned three occupational exposures when specific metabolic genes were expressed and found evidence of gene-environment interaction with glutathione S transferase (GST), N-acetyltransferase (NAT), and sulfotransferase (SULT). Although these findings illustrate the importance of studying combinations of exposures, results are based on a very small sample size; therefore, further exploration is needed. 15 Benzene is a recognized carcinogen which must be activated to benzene oxide (BO) to utilize its carcinogenic potential. BO can be detoxified in vivo by a reaction with glutathione and excretion in the urine as S-phenylmercapturic acid. 17
The IARC has classified diesel exhaust as a carcinogen based on lung cancer evidence. 18 Exposure to diesel engine emissions are constant with the hypothesis of a threshold effect, however, the excess risk of bladder cancer occurs only at high concentrations of exposure. The mechanism underlying this correlation remains theoretical; particles deposited in the lungs, and their metabolites, can frequently be found in measurable quantities in other organs. 19 It is assumed that the gases and particulate substance, which include elemental carbon and PAHs, are emitted by diesel engines. 20 Diesel-related metabolites may accumulate in the urine where they may interact with the urothelial cells of the bladder to initiate carcinogenesis. 21 Greater levels of diesel metabolites have been detected in the urine of exposed individuals compared to unexposed individuals.22,23 It was suggested that such metabolites may lead to genotoxic effects including DNA damage and DNA-adduct formation24,25 in urothelial cells, which can lead to cancer if the damage is not repaired.
With regard to the duration of exposure, most cases of cytological atypia appeared after five years of exposure.
It was also observed that during collection of samples, all of the petrol station workers were non-Saudi and little or non-educated. They ignore all precaution measures, such as wearing masks and washing hands, which are useful tools to reduce their exposure. Such individuals require awareness programs towards these hazards and how they can reduce them.
In the present study, the acute inflammatory cells infiltrate was not significant, but the chronic inflammatory cells infiltrate was statistically significant among cases. The presence of chronic inflammatory cells in the urine of such exposed workers may predict continuous inflammatory processes due to continuous exposure. However, further study is needed in this area with a link with what is known as the neutrophil-to-lymphocyte ratio (NLR). The NLR is an inflammatory index that has been considered as a potential prognostic factor in human cancer. 26 In the present study, the predominance of abnormal variables among cases compared to controls, may verify the harmful effects of petroleum occupational exposure on the wall of the urinary bladder, which might eventually lead to the development of precancerous and cancerous lesions.
The limitation in this study is that we did not use the urinary biomarker (such as the urinary’s t,t-MA, formaldehyde, and acetaldehyde ) to determine whether there is a cancer risk from exposure to benzene, formaldehyde, and acetaldehyde.
However, this study raised some controversies for policy makers to plan strategies to petroleum product workers and at the same time to stimulate further research into this issue.
In conclusion, the exposure of petroleum station workers to petroleum products increases the risk of urothelial atypical changes which may progress to precancerous changes. Awareness programs for petroleum station workers are needed, particularly for wearing masks and washing hands. Continuous screening for those who have worked for more than five years is important. Urine cytology can be a suitable non-invasive and cost-effective procedure for large population screening.
Footnotes
Acknowledgements
The authors thank the University of Hail for supporting this work. The authors also thank the petroleum station workers for their kind collaboration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.