
Abstract
Purpose:
The aim of this study was to evaluate the effect of the infliximab on autogenous-mediated bone regeneration and resorption of autogenous graft in the ovariectomised rat model.
Materials and methods:
Forty rats underwent ovariectomy and 6 weeks later the animals were randomly assigned to four groups. Critical size defects were created in each rat calvarium. In the control group (C), the flap was closed without any further action. In the only infliximab group (In), the flap was closed without any further action. After the operation, intravenous infliximab was injected. In the autogenous graft group (Ag), autogenous bone was applied in to the defect. In autogenous graft + infliximab group (Ag+In), autogenous graft was placed on the defect. After the operation, intravenous infliximab was injected. The animals were sacrificed at 4 weeks. Bone formation was assessed by micro-computed tomography (micro-CT) scans and stereological analysis.
Results:
The mean new bone volume was the greatest in Ag+In group (1.76 ± 0.20), followed by the Ag group (1.51 ± 0.05) (statistically significant difference at P <0.05). The lowest new bone was found in the control group (1.05 ± 0.09), however no difference was observed from the In group (1.14 ± 0.08) (P >0.05). Besides there was a statistically significant difference between the Ag+In group (1.00 ± 0.05) and Ag group (0.74 ± 0.04) in terms of the graft volume (P <0.05).
Conclusion:
This study, despite its limitations, showed that infliximab has a beneficial effect for prevent graft resorption and bone regeneration in osteoporotic rats.
Introduction
Maxillofacial bone defects caused from tumours, infection or traumas require surgery. Various bone substitutes are used to restore bone defects; however, bone healing depends on the properties of the substitutes and the host bone.1–5 Osteoporosis is a skeletal disorder that delays bone healing and reduces the quality of new bone formation.1,3 Many studies have focused on fracture prevention and therapeutic management to enhance bone density during osteoporosis;6,7 however, few studies have focused on osteoporotic bone regeneration in the presence of grafted biomaterials. 5
TNF-α is an important mediator in local erosive processes and systemic osteoporosis. It is an osteoclast-stimulating molecule that induces the receptor activator of nuclear factor kappa B ligand (RANK-L) production.8,9 Agents that block TNF-α have been proposed to protect bone and cartilage by imparting a beneficial systemic effect on bone metabolism.8,10 Infliximab, a human IgG1 TNF-α monoclonal antibody, is used for rheumatoid arthritis therapy, where it reduces TNF-α levels in the crevicular fluid in rheumatoid arthritis patients. 11 Infliximab also prevents bone resorption during periodontitis.9,12 Here, we implemented an ovariectomised rat model to evaluate the effect of infliximab on bone regeneration and resorption after application of an autogenous graft.
Materials and methods
Surgical procedures
Eight-month-old female rats (n = 40) with an average weight of 250 g were ovariectomised and randomly assigned to four groups. Six weeks after the ovariectomies, the rats were anaesthetised with an intraperitoneal injection of 10 mg/kg ketamine HCl (Ketalar; Pfizer, Istanbul, Turkey) and a semi-lunar incision was made in the calvarium, allowing reflection of a full-thickness flap in the anterior direction. A 5-mm-diameter calvarial defect was created using a trephine bur on low speed under continuous saline irrigation (Figure 1). Later, the operation flaps were closed with 3/0 silk suture material. This study was approved by the Bulent Ecevit University Animal Care and Use Committee.

Critical size defect in rat cranium.
Experimental groups
Animals were assigned to four groups:
Control group (C): the flap was closed without any further action.
Infliximab group (In): the flap was closed without any further action. After the operation, 5 mg/kg of intravenous infliximab was administered.
Autogenous graft group (Ag): the autogenous graft was ground using a bone grinder and applied to the defect. The flap was sutured using silk sutures.
Autogenous graft + infliximab group (Ag+In): the autogenous graft was applied using the same method as with the Ag group, and after the operation, 5 mg/kg of intravenous infliximab was injected.
All animals survived during surgeries and the postsurgical period. There was no evidence of wound dehiscence, wound infection or abscess formation. All animals were sacrificed 4 weeks after the operation. Calvarias were removed and kept in formaldehyde prior to stereological examination and micro-computed tomography (micro-CT) analysis.
Micro-CT analysis
Samples were scanned using micro-CT (Skyscan 1174; Micro Photonics Inc., Allentown, PA, USA) with a spatial resolution of 15 µm, using 50 kV and 800 µA at a 0.7° rotation step for a total of 180°. Three-dimensional images were taken using NRECON software, and the data were evaluated using CTAn software. Only the volume of mineralised new bone, without graft materials, was calculated (Figure 2).

Micro-CT views of the defects. (a) Autogenous graft group (Ag) in the 4th week. (b) Autogenous graft + infliximab group (Ag+In) in the 4th week. (c) Infliximab group (In) in the 4th week. (d) The control group (C) in the 4th week.
Stereological analysis
Prior to stereological analyses, samples were decalcified in formic acid (5%) for 21 days. Samples were then fixed in 10% formaldehyde, dehydrated in a graded alcohol series, and clarified in xylol for light microscopic examination. After dehydration, samples were embedded in fresh paraffin and cut using a microtome (Leica RM 2135; Leica Instruments, Nussloch, Germany). Paraffin blocks were cut serially to a thickness of 7 μm, and every 20th section was selected for analysis. The first section was chosen at random and all sections were sampled in a random manner. Sections were stained with haematoxylin–eosin (H&E) and photographed using the stereology analysis system (Stereoinvestigator 9.0, Microbrightfield, Williston, VT, USA) with a light microscope (Leica M 4000 B, Germany) containing a digital colour camera (Microbrightfield, Williston, VT, USA).
To estimate the volume of new bone area (Vn; Figure 3), the unbiased Cavalieri method was applied using point-counting test grids. The point density of the point-counting test grids was designed to obtain an appropriate coefficient of error (CE). CEs and coefficients of variation (CVs) were estimated according to the formula of Gundersen and Jensen. The volume of each area was estimated with following formula:
where ‘t’ is section thickness, ‘a/p’ is the area of each point on the point counting grid, and ‘∑p’ is the total number of points hitting the area of interest.

Histological view of defect region. Autogenous Bone Graft (ABG), Defect Margin (DM), New Bone (NB) (H&E, original magnification ×250).
Statistical analysis
The Shapiro–Wilk test was used to determine whether the data were normally distributed. Comparisons of the new bone, connective tissue and residual graft values were analysed using the Kruskal–Wallis non-parametric test, followed by post-hoc group comparisons with the Bonferroni-adjusted Mann–Whitney U test after normality of data had been failed. For the Bonferroni correction, α = 0.05/6 = 0.008 was considered to be statistically significant. All tests were performed using statistical software (SPSS Inc., version 19.0, Chicago, IL, USA ).
Results
Animals
All animals tolerated surgery well and survived the postsurgical period. Neither wound dehiscence nor wound infection nor abscess formation was observed at any surgical site.
Micro-CT and histomorphometric findings
New bone volume (mm3) is shown in Figure 4. The mean new bone volume was the greatest in the Ag+In group (1.76 ± 0.20), followed by the Ag group (1.51 ± 0.05) (statistically significant difference at P <0.05). The lowest new bone was found in the control group (1.05 ± 0.09), however no difference was observed from the In group (1.14 ± 0.08) (P >0.05).

New bone volume (mm3) in study groups.
Micro-CT (%) is shown in Figure 5. The greatest new bone was found in the Ag+In group (15.12 ± 2.57), and a significant difference was observed from the Ag group (8.05 ± 2.25) (P <0.05). The lowest new bone was found in the control group (1.15 ± 0.31), however no difference was observed from the In group (1.30 ± 0.35) (P >0.05). There was a significant difference between the Ag groups and non-Ag groups (P <0.05).

The percentage of new bone in micro-CT (%) in study groups.
The volume of connective tissue (mm3) is shown in Figure 6. The mean connective tissue volume was observed to be the lowest in the control group (0.94 ± 0.09) and the highest in the Ag+In group (1.66 ± 0.07) (P <0.05). There was a statistically significant difference between the control group and the In group (1.22 ± 0.09) in terms of the volume of connective tissue (P <0.05), whereas no difference was observed between the Ag+In and Ag groups (1.54 ± 0.14) (P >0.05).
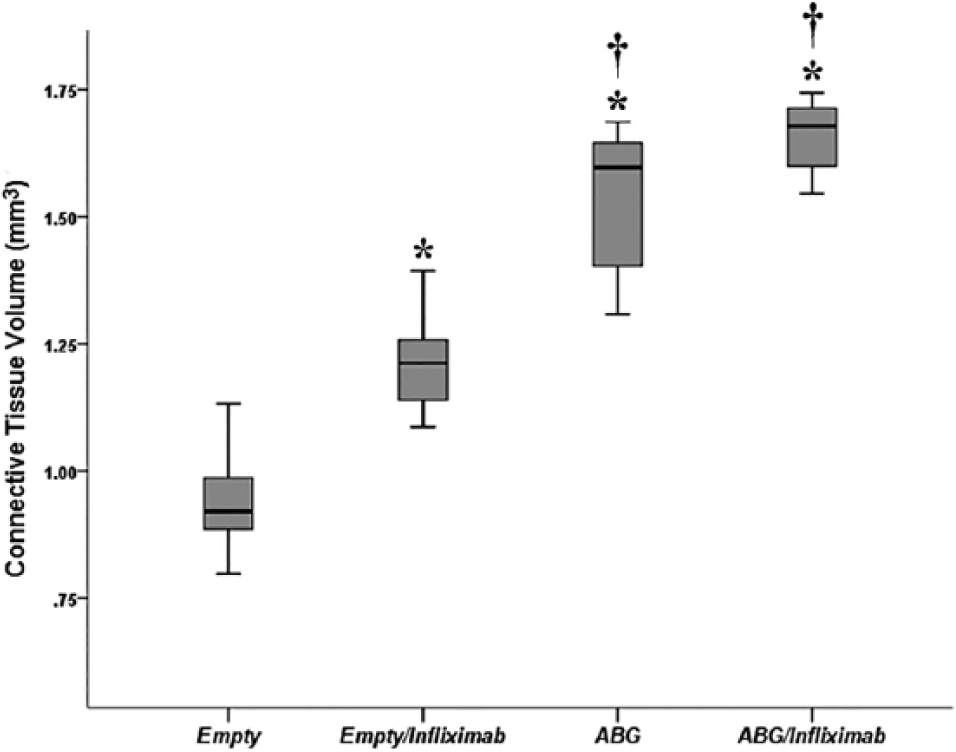
Connective tissue volume (mm3) in study groups.
Residual graft volume is shown in Figure 7. There was a statistically significant difference between the Ag+In group (1.00 ± 0.05) and Ag group (0.74 ± 0.04) in terms of the graft volume (P <0.05).

Residual graft volume (mm3) in study groups.
Histological evaluation
Histological analysis showed new bone formation in all groups. Neither inflammatory reaction nor secondary infection findings were observed at any surgical specimen. Fibrous connective tissue was mainly observed in the C and In groups. Centripetal (from the periphery toward the centre of defect new bone formation) was seen in all groups. No new bone formation was detected at the centre of the defect area in the C and In groups. Although there was new bone formation there was no significant difference between the C and In groups; more cellular collagenated connective tissue stroma was seen in the In group. The lowest new bone formation was found in the control group.
In the Ag and Ag+In groups, autogenous grafts were trapped by new bone and in some areas it reached to defect margins. In both groups using Ag, connective tissue was superior and irregular between new bone areas.
Discussion
Osteoporosis is a systemic illness characterised by inadequate bone formation and excessive bone resorption. Osteoporosis reduces bone volume and density in the maxilla and mandibula, and increases bone destruction around the teeth. However, the changes in osteoporotic bone, including the regenerative processes mediated by biomaterial implantation, have been only minimally evaluated.1,4,5
In this study, we evaluated the effect of infliximab on bone regeneration and resorption after application of an autogenous graft in an ovariectomised rat model. To our knowledge, this is the first study investigating such an effect. Stereological methods and micro-CT analyses were used to evaluate new bone and resorption of the autogenous graft.
Histological and pathological tissues are often examined in two dimensions using conventional methods; 13 however, Sterio 14 reported several modifications for estimating the quantity of structures in three-dimensional space. The estimation of microscopic parameters in three-dimensions increases the accuracy of morphological measurements. 13
Biomaterial-mediated bone regeneration processes were impaired under osteoporotic conditions,5,15–18 which indicated the negative impact of osteoporosis on bone graft healing. Oberg et al. 17 performed 5-mm-diameter defects in ovariectomised and healthy rabbit tibias, and grafted half of the cavities using allogeneic bone. After 8 weeks, histologic evaluations revealed no differences between the empty and grafted cavities. However, significantly less new bone was formed in the ovariectomised rabbits compared with the healthy animals. Kim et al. 18 created surgical defects in the calvarium of ovariectomised and non-ovariectomised rats and grafted defects with a mixture of tooth ash and plaster of Paris. The ovariectomised group had less bone formation compared with non-ovariectomised animals. In a similar ovariectomised rat model, Durao et al. 6 showed a decrease in biomaterial-mediated bone formation using microtomographic and histological analyses. They also observed impaired osteoblastic function in the regenerated bone of ovariectomised rats using gene expression analyses. The authors suggested these findings were consistent with impaired osteogenic processes in biomaterial-mediated bone healing in osteoporotic patients. Ribeiro et al. 16 created surgical defects in ovariectomised rat femurs and grafted defects with hydroxyapatite. In the ovariectomised group, without hormone replacement therapy, less newly formed bone was observed during histological analyses.
Surgical ovariectomies are commonly performed in osteoporotic rat models, and thus, were used in the present study. Rats were our preferred model as they closely resemble major clinical symptoms in humans when oestrogen is deficient. Another reason for our preference of ovariectomised rats is because osteoporotic bone modifications are rapid.
TNF-α plays a dominant role in local bone resorption and systemic osteoporosis. It is an osteoclast-stimulating molecule that induces the receptor activator of nuclear factor kappa B ligand (RANK-L) production;8,9 thus, agents that block TNF-α may protect bone and cartilage. Infliximab is an IgG monoclonal antibody that binds TNF-α, inhibiting its activity.19–21 In this study, we used infliximab to prevent graft resorption and evaluated its effect on bone healing using an osteoporotic rat model. The mean new bone volume was greatest in the Ag+In group, and a statistical difference in graft volume was observed between the Ag+In and Ag groups.
Consistent with our results, TNF-α inhibition was also beneficial in other studies. 8 Kastelan et al. 22 showed that inhibition of TNF-α prevented bone resorption in ovariectomised mice. Moreover, postmenopausal women with osteoporosis have increased TNF-α levels. Goncalves et al. 10 reported that infliximab prevented bone resorption in a periodontitis model, while Timmen et al. 23 showed that infliximab inhibited TNF-α, which was otherwise harmful during chronic inflammation and fracture healing.
Consistent with previous studies, 5 mg/kg infliximab was used in this study. This dose of infliximab is effective at preventing inflammatory changes and bone loss. Gonçalves et al. 10 reported that lower doses of infliximab failed to prevent bone resorption.
In this study, we evaluated the effects of infliximab treatment using an osteoporotic rat model. Our results showed that infliximab prevented graft resorption and increased bone regeneration in osteoporotic rats. Additional studies are required for understanding the benefits and side effects of infliximab on bone regeneration in osteoporotic models.
Footnotes
Acknowledgements
Special thanks to our research assistants, Gamze Yayla and Burcu Delibaş, for performing stereological examinations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.