
Abstract

Significant updates to the patient care process
Language has been updated to be more inclusive and person-centred.
More emphasis has been placed on patient assessment in order to focus users on exploring the identified problem(s).
More emphasis has been placed on monitoring, to ensure that specific targets/goals are set with next steps for patient reassessment in the follow-up plan.
A glossary of terms has been added to clarify language, including those with multiple iterations (like “care plan”), and to improve consistency for structure and meaning (such as for “drug therapy problems”).
The process of providing patient care for pharmacists working in any care setting is illustrated in Figure 1. Although the process is inherently cyclical, the initial step, collect data, involves the creation of a database of relevant patient information. This is the first section where the purposeful inclusion of person-centred language is evident, with sex at birth and pronouns added for consideration, along with members of the patient’s circle of care. In addition to gathering the appropriate demographic information, pharmacists must determine or clarify the reason the patient is seeking care, being referred, or requiring an assessment. Understanding the patient’s health goals, values, and medication experience is essential for delivering person-centred care and supporting shared decision-making. Information may be gathered through a patient interview as well as from other sources such as electronic health records and/or prescription records. It is emphasized that data collection should be comprehensive but limited to what is required to provide care.
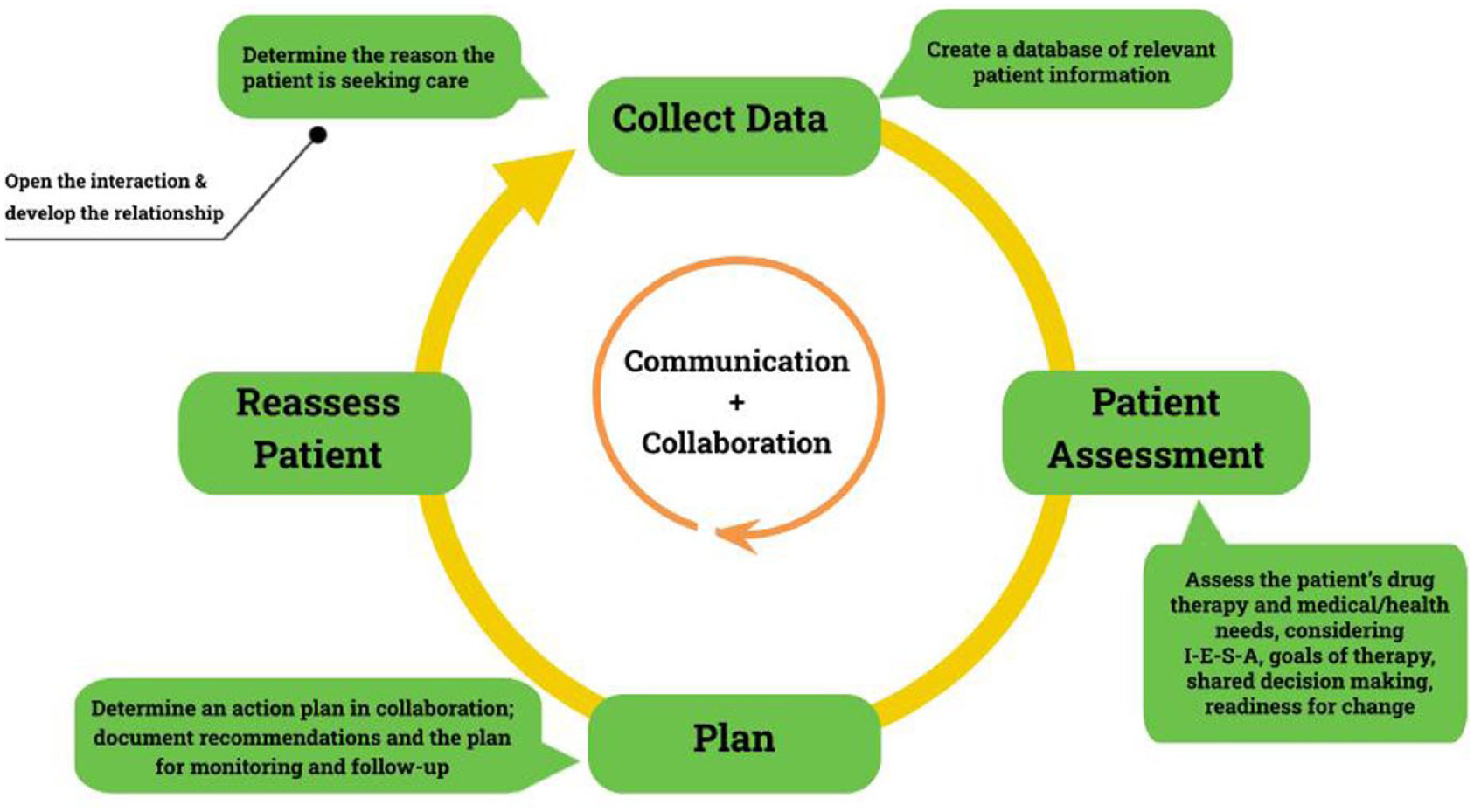
Patient care process diagram
The history of present illness (HPI) allows for an exploration of what the patient has experienced with their primary concern or most urgent issue. For acute conditions, the use of the symptoms, characteristics, history, onset, location, aggravating factors, remitting factors, and explanation (SCHOLAR-E) approach is encouraged, with other mnemonics also provided to allow for provider flexibility. A best possible medication history (BPMH) is clarified as a comprehensive approach to gathering current and previous prescribed and non-prescribed medications, along with the patient’s medication experience and ability to adhere. Relevant historical information may include medical conditions, allergies, family history, and/or consideration in the expanded functional and social history sections. A review of systems may be appropriate to support the assessment of the patient’s reason for seeking care or to help identify other medical conditions or medication adverse effects. A head-to-toe approach is outlined to assess relevant systems, and data from investigations, such as vital signs, physical examination findings, or results from laboratory, imaging, and/or other diagnostic tests, which are becoming more available to pharmacists in community practice settings across Canada, may also be necessary for a thorough assessment.
Patient assessment involves evaluating collated data, current drug therapy, and the patient’s health needs to identify drug therapy problems (DTPs) and to consider therapeutic alternatives using the indication, effectiveness, safety, and adherence (I-E-S-A) framework. In the updated version, a purposeful decision was made to shift from “drug-related” to “drug therapy” to emphasize that some problems identified will involve missing medication. A substantially revised comprehensive pathway to identify and resolve DTPs (Figure 2) provides step-by-step direction through the I-E-S-A framework with guiding questions to support both the assessment and next steps towards a plan. Importantly, drug interactions are clarified as potential causes of an effectiveness or safety issue, and adherence explores barriers to medication taking and the patient’s medication experience.
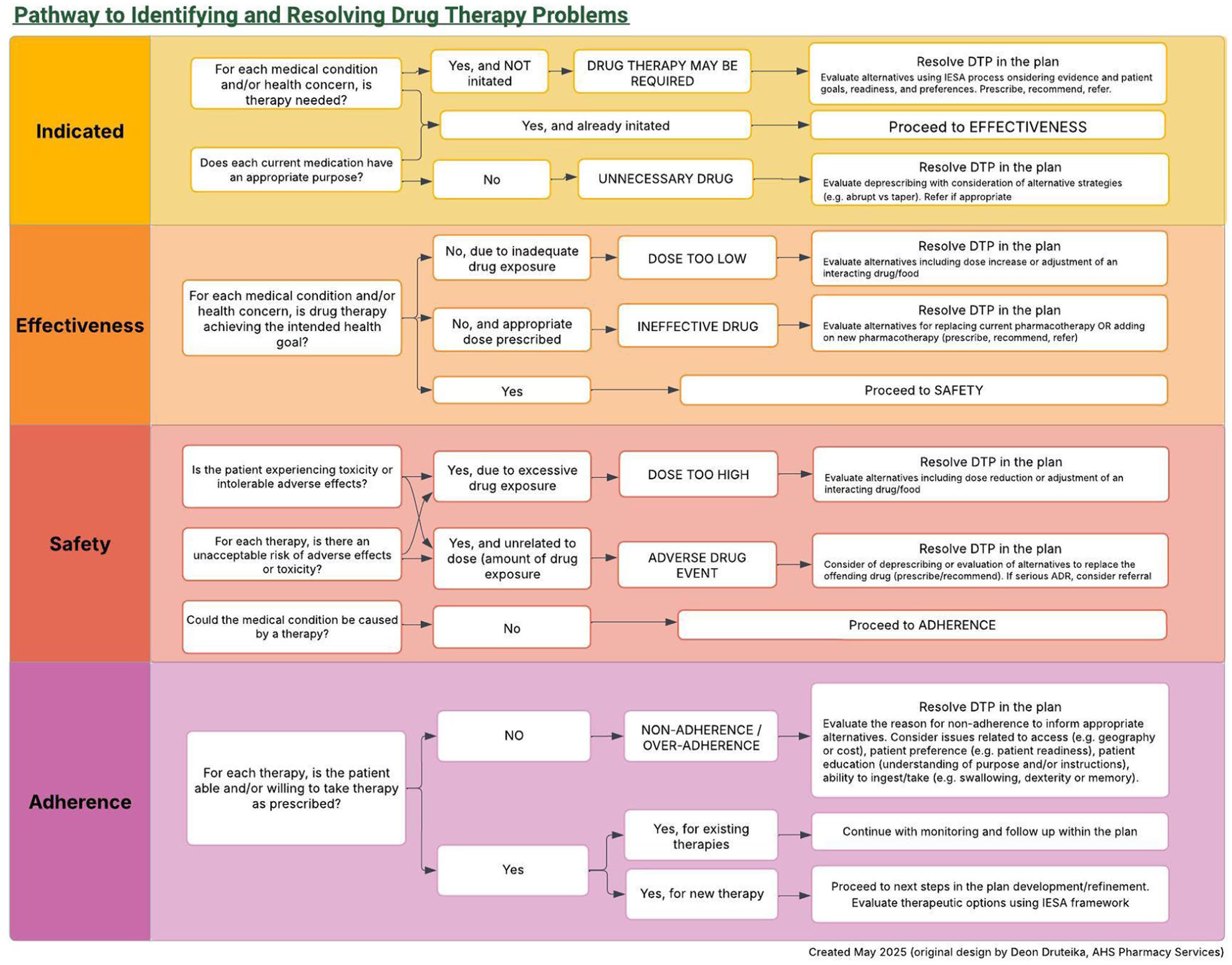
Pathway to identifying and resolving drug therapy problems
For each DTP, pharmacy professionals should consider both non-pharmacologic and pharmacologic options that are indicated and expected to be effective and safe. Therapeutic options should be evaluated based on evidence, patient values, and feasibility for access and ability to adhere. In some cases, deprescribing, or the planned process of reducing or stopping drugs, may be the most appropriate course of action.
Person-centred care is further emphasized in the Plan. Engaging the patient (and/or patient’s agent) to determine the best recommendation is essential for collaborative goal setting, shared decision-making when considering reasonable alternatives, and honouring patient autonomy. The chosen course of action may be adding, changing, or removing a pharmacotherapy (prescribe/deprescribe, recommend, or refer) and/or implementing non-pharmacologic strategies.
The critical component of the Plan involving the establishment of an effective monitoring and follow-up plan is expanded to clearly outline the components of what, who, and when. First, the specific parameters that should be monitored (what) need to be identified with specific targets, goals, or thresholds. For example, systolic blood pressure could be a parameter with an efficacy target of achieving <130 mmHg consistently and a threshold of concern for safety of dizziness/light-headedness upon standing on multiple occasions. Action would need to be taken if the target is not reached or the threshold of concern occurs. The responsibility for who is monitoring should be clear, in addition to when the parameter will be assessed. Will the patient monitor at home daily or will the pharmacist check weekly, or both? For follow-up, a realistic timeline for the target to be achieved and/or threshold of concern to be identified should be set, along with how the pharmacist and patient will communicate with each other to assess or discuss.
The last step of the PCP, reassess patient, is essentially initiating the process anew—supporting ongoing management of chronic conditions or assessing improvement of the acute ailment. New data are collected, focusing on changes since the previous interaction. The assessment will explore whether DTPs remain and will modify the care plan as needed. Again, this may involve adding, changing, or removing pharmacotherapy (prescribing/deprescribing, recommending, or referring). It should be emphasized that monitoring and follow-up cannot be neglected and are not one-time tasks; rather, they are a critical component of the ongoing process that enables the care plan to be adjusted based on evolving health goals and necessary changes in targets and thresholds.
There are other notable additions and revisions to the 2025 PCP document. A glossary of terms has been introduced to enhance clarity for learners; support consistency among instructors, preceptors, and clinicians; and align terms with the Alberta standards of practice. An updated Pharmacy Care Plan Worksheet has been included to reflect the revised process (see pages 20-21 of the PCP document: https://doi.org/10.7939/82181), and a detailed graphic has been included to support the development of robust monitoring and follow-up plans. Additionally, a companion document to the PCP that guides the documentation of patient care has been developed. 3
The Faculty of Pharmacy and Pharmaceutical Sciences PCP is being implemented across the pharmacy curriculum for fall 2025. We invite all pharmacists to use the document and process for their clinical practice and teaching activities. This open-access item can be referenced as noted below in reference 1.■
Footnotes
Author Contributions:
T. Leslie and J. Hall drafted the manuscript. T. Leslie, R. Breault, and J. Hall edited the manuscript and approved the final version.
Funding:
The author(s) received no financial support for the authorship and/or publication of this article.
Declaration of Competing Interests:
None to declare.
Ethical Approval and Informed Consent Statements:
N/A
Data Availability Statement:
N/A