
Abstract
Background:
Pharmacists are essential to team-based care, contributing knowledge and expertise that positively impact patient care. However, it is less clear how interprofessional collaboration is enacted by pharmacists in single-disciplinary outpatient practice environments.
Methods:
We recruited pharmacists from 3 university-affiliated, pharmacist-led primary care clinics in Canada. Employing a social network analysis approach, the data collection encounter explored the nature and composition of collaboration in patient care. We conducted semistructured interviews, including participant drawings (sociograms), to illustrate their network experiences caring for specific patients. Transcripts from the data collection encounters were systematically coded and analyzed in an iterative process. Initial codes were generated inductively and broader categories refined through constant comparison and finalized by author discussion.
Results:
Eleven (78%) pharmacists were interviewed and drew 28 sociograms. Pharmacist networks encompassed a wide array of health professionals and patient family members. Despite the physical distribution of interprofessional members, pharmacists formed and maintained relationships to support patient care through conscientious communication and medication management decision-making. Network relationships and system factors influenced collaboration and patient care, often resulting in practice paralysis and/or the need to re-emphasize patient self-advocacy.
Interpretation and conclusion:
Our findings underscore the dynamic nature of pharmacist networks and how they are navigated to support pharmacist-led medication management. Primary care pharmacists attempt to overcome encountered barriers to implementing patient care plans through various strategies, including leveraging new and existing network relationships. System obstacles impeding effective and efficient patient care could in part be overcome through pharmacist scope of practice expansion.
Introduction
Interprofessional care is endorsed by professionals and policymakers alike as the model for health service delivery in Canada.1,2 Primary care pharmacists embedded in general medical practices with physicians and other health professionals positively impact direct patient care. Studies of such team-based primary care demonstrate how drug therapy and other health outcomes, including patient quality of life, are optimized through pharmacist integration.3-5 These findings offer encouraging perspectives on the pharmacist’s impact and influence on patient care when team members are co-located in hospitals, specialized clinics, or ambulatory care settings. However, in many primary care settings, pharmacists are situated in independent practices without other health professionals physically present on predesignated teams.
Knowledge into Practice
Pharmacists are essential to interprofessional patient care, but it is less clear how pharmacists in single-disciplinary practice environments collaborate with others.
Pharmacists leading medication management in university-affiliated primary care clinics form, maintain, and enact collaborative relationships with other professionals in diverse patient care networks. Pharmacists in these single-discipline practice environments have developed specific strategies to share care with those who are not physically present in their practice.
Our findings underscore the dynamic nature of pharmacist networks and how they are navigated to support pharmacist-led medication management. However, system and policy barriers to pharmacist practice undermine safe and efficient primary patient care.
Practice configurations for primary care pharmacy in Canada are evolving. Pharmacist-led primary care represents an appointment-based ambulatory care model whereby patients see the pharmacist for health and drug therapy assessment and management in a clinic setting. 6 Patient consultation for pharmacist-led primary care in Canada is a model of care already associated with reduced opioid use for non-cancer pain, non-drug-based resolution of chronic insomnia, modification of cardiovascular risk factors, and enhanced medication adherence.7-9 Typically, pharmacists in these practices are not physically co-located with other health professionals. Given the potential dynamic and complex nature of patients’ medical and social conditions in general practice, it is important to understand how primary care pharmacists in pharmacist-run clinics collaborate with other team members to achieve these positive outcomes.
The large body of literature outlining the barriers and facilitators to interprofessional care consistently points to relationship quality between members. Positive relationships built on trust and respect between health professionals are cited as essential for collaboration. 10 Effective relationships may be marked by a shared vision for patient care. 11 Interpersonal relations among health care team members also affect communication, team performance, and patient safety. 12 While the research underscoring the value of interprofessional relationships is clear, very little is reported about how positive relationships between collaborating members initially form and continue to function.
Mise En Pratique Des Connaissances
Les pharmaciens sont essentiels à la prestation de soins interprofessionnels aux patients, mais la manière selon laquelle les pharmaciens des milieux de pratique monodisciplinaires collaborent avec les autres est moins clairement établie.
Les pharmaciens qui dirigent la gestion des médicaments dans des cliniques de soins primaires affiliées à des universités forment, maintiennent et mettent en œuvre des relations de collaboration avec d’autres professionnels de divers réseaux de soins aux patients. Les pharmaciens de ces milieux de pratique monosciplinaires ont élaboré des stratégies précises pour partager des soins avec des personnes qui ne sont pas physiquement présentes dans leur pratique.
Nos résultats soulignent la nature dynamique des réseaux de pharmaciens et la façon dont ils sont utilisés pour soutenir la gestion de la pharmacothérapie dirigée par des pharmaciens. Cependant, les obstacles à la pratique de la pharmacie liés aux système et aux politiques nuisent à l’offre de soins primaires sécuritaires et efficaces aux patients.
The social network analysis (SNA) research paradigm investigates relationship ties between individuals or groups in a given context.13,14 The resultant networks may be dynamic entities as individual member(s) and system conditions impact how these relationship ties form, function, strengthen, and even dissolve. By mapping these relationships and connections, SNA can uncover unique patterns, structures, and compositions of networks and how they influence behaviour. Using SNA, research project objectives were to visualize and characterize network member relationships in pharmacist-led primary care and how these impact patient care.
Methods
Methodology
We employed a qualitative social network theoretical and analytical framework using an egocentric perspective. Egocentric SNA is an approach to both model and analyze an individual’s relationships as described from their perspective. 15 Network-based data can characterize and advance understanding of these relationships and how they influence attitudes, experiences, and behaviours, and ultimately patient care.
Setting and participants
Our study recruited participants at the 3 university-affiliated, pharmacist-led primary care clinics established in Canada (Memorial University in Newfoundland, the University of Saskatchewan, and the University of British Columbia). Clinics were located on campuses of the respective provincial academic settings for pharmacist training. Pharmacists conducted patient appointments in-person, onsite in consultation rooms, or remotely using videoconference/telephone.16-18 In addition to certain specialty care at some sites, general medication management services were provided at all 3. All clinic pharmacists at the time of our study in 2023 (N = 14) were invited by email to participate.
Data collection
Consistent with the SNA approach, the data collection encounter was designed to explore the composition and nature of collaborative relationships in pharmacist-led primary care practice: a 30-minute semistructured interview followed by the participant drawing to illustrate their specific network experience caring for 2 to 3 selected patients (sociograms). Participants were instructed to position themselves in the centre (as the ego). Collaborating network members drawn in large circles (nodes) represented more influential relationships than those in smaller circles. Thicker lines between the ego and network member represented closer relationships than dotted ties. Interview recordings were transcribed verbatim by a third party (TranscriptHeroes: https://transcriptheroes.ca).
Data analysis
Transcripts from the interviews and narratives from the drawing component were coded by the first author and analyzed in an iterative process throughout the data collection period using NVivo as supporting software. 19 Initial codes were generated through an inductive process and broader categories identified through pattern recognition and constant comparison. Repeated dialogue among the 3 authors (K.W., D.J., D.K.) guided code consolidation and interpretation of participant network relationships. Participant-drawn sociograms were referenced concurrently throughout the analytic process to enhance understanding of participants’ narrative descriptions.
The research team consisted of pharmacists and educators experienced in primary care and interprofessional practice and research. Two authors (D.J., D.K.) were involved in the development and leadership of the pharmacist-led clinics at their universities but did not have access to unblinded participant data. Researcher reflexivity was employed whereby researchers acknowledged the influence their backgrounds had on the collection and interpretation of the data.
This study was approved by the University of British Columbia Behavioural Research Ethics Board (BREB # H21-0162).
Results
Eleven (78%) pharmacists completed the data collection encounter (Table 1), including 28 total sociogram drawings (Figure 1). Pharmacist network collaborators consisted of health professionals from many disciplinary backgrounds as well as other pharmacists (Table 2).
Participant demographics (N = 11)
To avoid unblinding participants in this small sample and population size, we have withheld other identifying features such as participant self-identified race, age, and clinic location. We can report that at least 2 of 3 eligible pharmacists at each clinic participated.
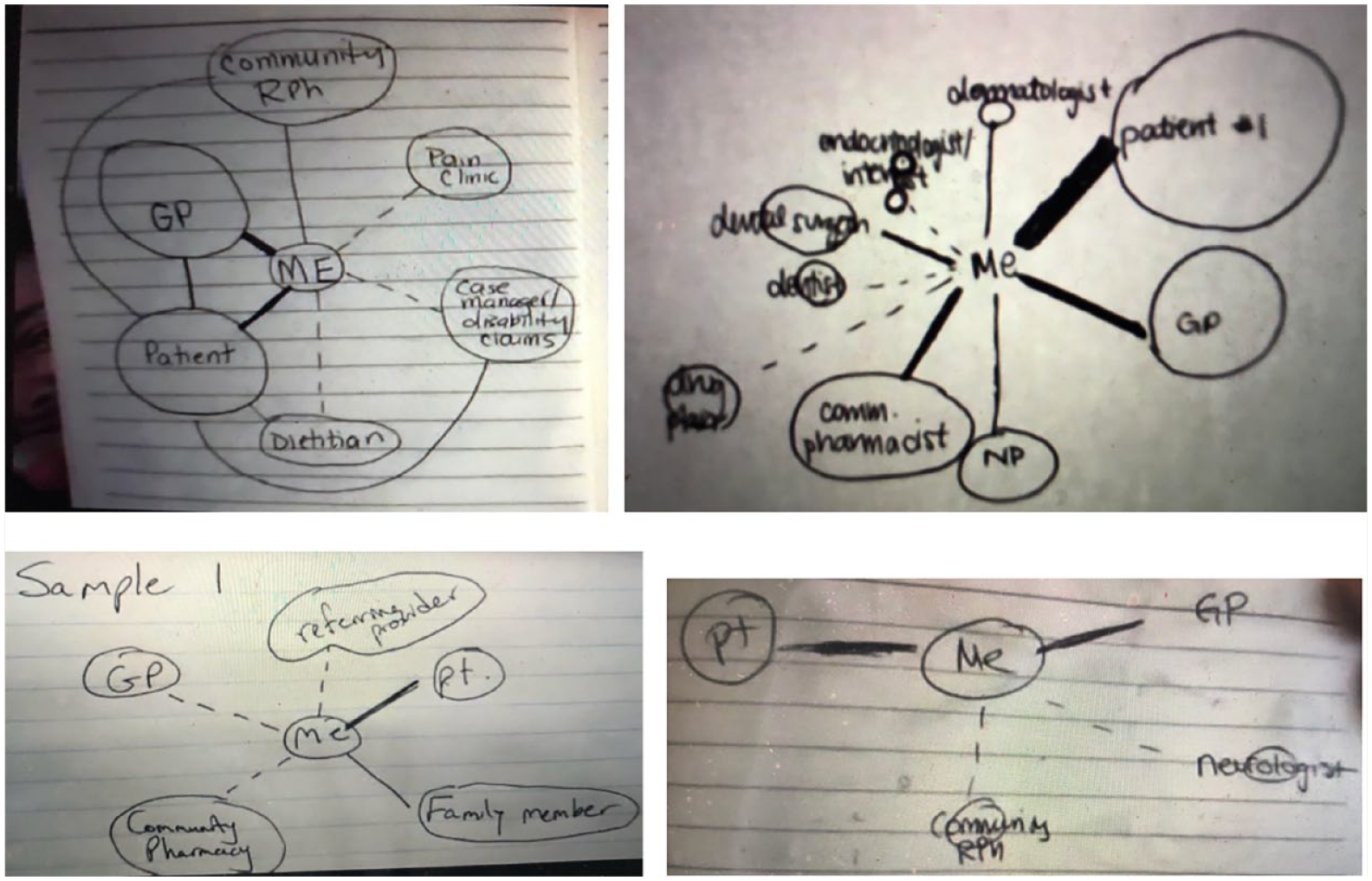
Participant sociogram samples
Participant network members*
Participant network members were identified from both participant interview or sociogram drawing narratives.
Primary care pharmacist network relationships formed through formal clinic referral and informal circumstances. Pharmacists maintained relationships with network members by purposeful communication and favourable patient-oriented outcomes. We identified how these network relationships and other system factors subsequently influenced collaboration and patient care, resulting in practice agility or paralysis and emphasis on patient self-advocacy.
Forming collaborative relationships
Driven by referral: The 3 clinic sites received patients through the same referral process, namely by a health professional or by the patient (or family member) directly. The network relationship between the pharmacist and other health professional typically stemmed from this first point of contact and, in particular, following the patient’s first clinic appointment.
All pharmacists indicated past or ongoing clinic outreach in their communities to raise awareness of medication management services. Such intentional engagement directed additional referrals and network membership from government agencies, patient advocacy, and community groups.
Derived by circumstance: Accordingly, local health care landscapes heavily influenced pharmacist networks as members were drawn from distinct referring communities in the clinic’s region. Pharmacists had established consultation channels with specialty practices situated on or near their campus. Certain clinics also had service agreements with different health authorities.
Pharmacists described identifying and accessing network members through personal relationships. When entertaining patient referral for care beyond the clinic’s medication management scope, they sought advice from colleagues. Clinic pharmacists shared network member information gathered through resources, prior experiences, and even friendships with potential collaborators, including dietitians, physiotherapists, and occupational therapists.
Network relationships were also formed through patient nomination. Pharmacists often collaborated with other professionals providing care to their specific shared patient but also identified potential collaborators for others when endorsed by specific patients.
“There was actually a physiotherapist I worked very closely with and she was referred to me through a patient who said, ‘I have this awesome physiotherapist who helps me with all these things. You should connect with them’.” (Participant 1)
Maintaining collaborative relationships
Navigating communication: Considerable time and purposeful effort were invested in communication with network members. All pharmacists transmitted comprehensive clinic encounter documentation to the patient’s referring professional and primary care prescriber (if these were not the same). These appointment records and recommendations were intentionally crafted using language to promote clarity and trust, especially when the recipient was not the referring professional.
“If I don’t know that the GP has bought in, I might be a little more conservative in how I phrase things.” (Participant 8) “I’ve personally changed to using, ‘This is your patient’s goal and this is how I recommend to achieve the goal’.” (Participant 10) “Writing these notes was cumbersome, it probably took up more time than I spent face-to-face with my patients, . . . but necessary for establishing those relationships and gaining trust to actually be able to open up those lines of communication.” (Participant 7)
In some instances, documentation evolved as relationships with the recipient professionals strengthened through repeated referrals over time or expressed preferences for communicated recommendation(s). However, there was often no feedback whatsoever. Pharmacists were resigned to never receiving acknowledgment of the documented referral or direct information about prescribing actions arising from their recommendation(s). While 1-way communication with prescribers seemed widely accepted, it was decidedly discouraging for many.
“I would say 85% of the times, primary care providers don’t respond to our consult notes.” (Participant 3) “Sometimes, it’s emotionally defeating.” (Participant 9)
Unsurprisingly, pharmacists were invigorated when interacting with network members in real time. Pharmacists expressed a sense of satisfaction when opportunities to speak to others invariably expedited information exchange and patient care. Pharmacists tended to initiate phone conversations with other health care professionals more liberally than for physicians and described varied circumstances whereby calls to these network members were prioritized, including urgent (safety) issues or discussion of multiple recommendations.
“You can get a lot more clarified and you can also connect more and build rapport and gain mutual understanding of where each discipline is coming from with some form of verbal communication.” (Participant 6)
Ensuring positive outcomes: Pharmacists bring clarity to the medication management of the many complex patients referred to pharmacist-led clinic care. The consultation outcomes reinforced certain collaborative relationships in the pharmacist’s network, as evidenced by repeat referrals and sometimes more ready access to the network member for decision-making dialogue.
“In terms of developing a relationship with somebody who is referring a lot, I want to make sure I do my job and complete that task and build that relationship.” (Participant 2) “The care that we put into that patient, the thoughtful recommendations—it does end up with referrals for other patients and strong relationships, because, wow this is a great service.” (Participant 11)
Pharmacists consistently outlined situations where it was apparent that they were regular members of another professional’s collaborator network as a resource for patient care. Many pharmacists also identified strong network relationships with members who they had never met or spoken with but with whom they routinely exchanged patient information. Positive shared care experiences sometimes percolated into the consultation practices of adjacent health professionals.
“It was actually more through her colleagues who have referred to me, sharing their experience, that made her a little bit curious and led her to send that first referral.” (Participant 1)
Relationship impacts on patient care
Practice agility and paralysis: Strong network relationships resulted in responsive information exchange for patient care. Pharmacists described collaborative dialogue around decision-making and joint problem-solving with other professionals, patient families, and care providers.
However, it was apparent that despite strong relationships with network members, effective medication management often hinged on a collaborating primary care prescriber. Pharmacists described countless instances where, without one, plans to decrease medication safety risks to patients or improve therapeutic efficacy were “stuck in limbo.”
“If I’m making a recommendation because somebody’s really dizzy with really low blood pressure but they see a cardiologist maybe every 1 to 2 years, the family doctor could say they’ll defer any changes to the specialist. The patient feels really defeated often times, as do I . . . that [appointment’s] not for another year.” (Participant 9) “Even simple things, like somebody’s started thyroid therapy. The dose is too high and you can see from all the blood work and they’ve got all the symptoms and the dose really needs to be reduced . . . but we can’t act on our own.” (Participant 1)
Despite collaboration between them, positive relationships could not overcome practice rights differences between community pharmacists and these pharmacists in single-disciplinary clinic environments.
“There have been times that we sent [recommendations] directly to the specialist and we’ve gotten great responses. They’ll say, ‘yeah, go ahead’ but then they don’t know what we can and can’t do. So when they say, ‘yeah, go ahead’, I’m saying, ‘well, I can’t physically change this’. Here we don’t dispense, so it would have to go back to the [community] pharmacist who would then say, ‘well, that wasn’t to me, I need to hear that prescriber say that directly to me’.” (Participant 9) “Pharmacists not being able to prescribe, having to rely on someone else to write that prescription or action that item, creates inefficiencies and can make things more difficult for patients that are just trying to access care.” (Participant 1)
Patients as the Trojan horse: Information and recommendations were sometimes channeled to prescribers through the patients. Pharmacists formed trusting relationships with their patients and could also learn the outcome of their medication recommendations in follow-up appointments. Through these relationships, pharmacists also encouraged patient self-advocacy.
“We’re very clear about what our limitations are. So, part of my role is giving some pep talks in how to be an advocate in their own care, to empower patients to have conversations with their primary prescribers and other team members.” (Participant 5)
When unresolved medication issues were an ongoing patient concern, recommendation copies were provided to show the prescriber at their next appointment. Increasingly, such records were becoming an unfortunate but necessary option for clinic patients who had no prescribing primary care provider.
“So often what I’ve tried to do is just send my report with the patient to show to a clinician they wind up seeing. Because even they don’t know who they’re going to see.” (Participant 11) “We might arm them with information and say, ‘OK, if you’re going to go to the walk-in clinic, here’s some guidance as to what changes you could make’. Unfortunately, we don’t have a direct link to be able to link people up with prescribers. I wish we had that.” (Participant 5)
Discussion
The collaborative networks of pharmacists leading medication management in a single-disciplinary primary care environment encompass a wide array of health professionals, patients, and family members. Despite the absence of interprofessional team members physically embedded in the same practice spaces, primary care pharmacists formed and maintained relationships to support patient care through conscientious communication and medication management decision-making.
Lack of physical proximity and practice co-location are known threats to effective interprofessional care. In their review of strategies improving interprofessional collaboration in primary care, Sirimsi et al. 20 identified how useful formal and informal meetings were to communication and shared decision-making. Individuals on the team learned more about each other and built relationships over time. However, in pharmacist-led primary care clinics, there is no fixed interprofessional team, and it is evident from our findings that reaching members working elsewhere, when possible, takes effort. Communication through shared electronic health record platforms can facilitate work and collaborative relationship-building, but these systems’ existence, compatibility, and reliable use among our pharmacists’ network members were incomplete. 21 We know family physicians report inconsistencies coordinating care outside their practices. 22 Consequently, pharmacists in our study encountered challenges exchanging patient information in the network, which contributed to “action opacity,” the unknown fate of their medication management recommendations. 23
Our findings demonstrate that difficulties facing health professionals forming and maintaining collaborative relationships across distributed settings can be overcome. Pharmacists described thriving long-distance relationships with many different network members. In some instances, pharmacists may have previously met the other professional (e.g., at continuing education activities), but in many of these cases, they have never met in-person or even spoken on the phone. Perhaps unsurprisingly, clinic pharmacists could identify as members of multiple teams for different patients, transcending physical spaces. While communication was an essential factor for establishing and maintaining these relationships, pharmacists put confidence in the medication management work itself. A study of statewide diabetic foot care providers also found how positive patient outcomes promoted trusting relationships among distributed interprofessional collaborators, with little real-time communication. 21 Meanwhile, Canadian family physicians have also reported how trusting relationships with pharmacists was grounded in “first-hand observation” of success. 24 For the clinic pharmacists, trusting network relationships with collaborators were in part realized by a shared history of patient care over time, either for an individual or for multiple patients from an individual practice. It is likely that these network members were also somehow constructively predisposed to interprofessional care, which can be an accelerant to effective collaboration.11,25,26 We found pharmacists leading medication management in primary care were optimizing the interpersonal factors associated with successful interprofessional collaboration within their individual control.11,27
However, it was apparent how positive network relationships could not overcome health system and policy barriers to interprofessional primary care. Mulvale et al. 27 describe a conceptual framework of interprofessional collaboration reliant on interrelated policy (macro), organizational (meso), team (micro), and individual factors. Pharmacists in this study encountered “macro” and “meso” factors impeding medication management in primary care, including regulatory limits to making dosage adjustments, deprescribing, or ordering laboratory values, to name just a few. Such limits also had negative implications for intraprofessional collaboration between pharmacists in the clinics and community practice. Pharmacists in these non-dispensing clinic practices could not directly act on verbal order prescriptions or be indirectly transmitted to and processed by community pharmacists. These system and policy barriers undermine safe and timely medication management, which is further exacerbated for patients without a prescribing primary care provider. Given the current perilous state of primary health care in Canada, pharmacists’ right to exercise full scope of practice is imperative to contribute to the health system, as is already evident in some jurisdictions.28-32 Current variability in provincial regulations must also continue to shift towards national harmonization to avoid further widening of access disparities for patients.33,34 Our research clearly demonstrates professionals in pharmacist-led primary care clinics are poised to capitalize on these rights to augment collaborative patient care.
By design, an egocentric approach limited our findings to the individual pharmacist’s perspective. Other whole-network SNA approaches can map and quantify relationships across networks yet require input from all members. 35 Although our target population was finite (14 possible eligible participants nationwide at the time of our recruitment), we are confident we reached a point of information power whereby we acquired sufficient data to answer our research questions. 36 We did not set out to compare network relationships between the clinics but recognize that legislation and scope of practice in different provinces can dictate pharmacist abilities in their local networks of patient care. We began studying a small and relatively specific primary care practice; however, appointment-based, pharmacist-led primary care is now proliferating in Canada, particularly in community pharmacies. Our study offers important insights into forming and maintaining collaborative relationships that function to support timely and effective patient care when pharmacists are not physically co-located with other health professionals.
Conclusion
Pharmacists in single-discipline primary care clinics successfully collaborate with a wide variety of other health professionals in distributed settings and consider themselves members of multiple teams. Our findings underscore the dynamic nature of these relationships in pharmacist networks and how they are navigated to support pharmacist-led medication management. Primary care pharmacists attempt to overcome encountered barriers to implementing patient care plans through various strategies, which include leveraging new and existing network relationships. Persistent system and policy obstacles thwarting effective and efficient patient care could in part be overcome through pharmacist scope of practice expansion. ■
Footnotes
Author Contributions:
K.W. conceived and designed the project and led the data collection and analysis. All authors (D.K., D.J., K.W.) contributed to data collection design, data synthesis, and interpretation. All authors contributed to manuscript writing and approved the final paper.
Declaration of Conflicting Interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: We wish to acknowledge the Canadian Society of Hospital Pharmacists Research and Education Foundation, which awarded a grant to support this work.
Ethical Considerations:
This study was approved by the University of British Columbia Behavioural Research Ethics Board (BREB # H21-0162) in April 2022. Participants gave written consent for review and signature before starting data collection encounters.
Data Availability:
Researchers should contact the corresponding author with any data access inquiries.