
Abstract
Purpose:
As the scope of practice continues to evolve for pharmacists, professional abstinence is being observed by students in workplaces and practicums. Professional abstinence is defined as “consciously choosing not to provide the full scope of patient care activities”. Exposure of students to professional abstinence may cause cognitive dissonance, as they are challenged by practices that do not match what they are taught in school. This study explores pharmacy student perspectives on professional abstinence in community practice settings and their thoughts on how it could be addressed.
Methods:
Pharmacy students enrolled at an accredited Canadian pharmacy school with previous experience at a community practice site were invited to participate via email and social media. Data were collected between March and November 2021 through virtual individual interviews using a semistructured guide and the Zoom platform. Recordings were transcribed verbatim, and data were analyzed using cognitive dissonance theory to guide the inductive coding and interpretation of results.
Results:
Twenty students representing 6 pharmacy schools were recruited. Themes identified regarding students’ experiences with professional abstinence were “introspection and reflection” and “the system”, with the subthemes of emotion, excuses, professional identity and infrastructure, and inertia/disengagement, respectively. Regarding how to address professional abstinence, the themes “self as professional” and “empowering professionals” emerged. Self as professional included the subthemes of continuous learning, role modelling/mentorship, and internal drive/initiative, while empowering professionals included improved logistics, self-care, and advocacy.
Conclusion:
Students’ experiences with professional abstinence led to mixed feelings and influences on their professional identity. Pharmacy schools should be made aware of the phenomenon of professional abstinence and its effect on students, as they can potentially help manage learners’ cognitive dissonance and best prepare them for their future full-scope practices.
Knowledge into Practice
Professional abstinence has been defined as “consciously choosing not to provide the full scope of patient care activities” and continues to be found across pharmacy practices.
Given the important role mentorship plays in developing pharmacy students’ professional identity and skills, we sought to understand the impact that observing professional abstinence had on them.
We found that pharmacy students across Canada held 2 competing feelings: hopeful in their own ability to practice to full scope and burdened by the responsibility to be changemakers. They discussed an ongoing cognitive dissonance between what they are being taught in pharmacy school and what they are observing in practice.
Students voiced several solutions for professional abstinence, which reflect their responsibilities as professionals to continuously learn and advocate for the profession, as well as to surround themselves with like-minded practitioners rising to meet the challenges in practice.
Introduction
Few professions have seen as much change in the past several years as the practice of pharmacy in Canada. The continuous expansion of pharmacists’ roles is multifactorial and has been accelerated in some jurisdictions by the shortage of primary care physicians in the community.1,2 A full scope of practice for pharmacists is supported by a robust body of literature demonstrating the beneficial impact of their care on chronic disease outcomes.3-7
Ongoing practice change is essential to position pharmacists to best meet the needs of the communities they serve. However, nationally, there is heterogeneity in the legislation and regulating policies that govern the provincial scope of practice, creating diversity in the pharmacist’s practice at large. In addition, individual pharmacists have the autonomy to exercise their clinical judgment in providing professional services, including patient assessment and prescribing. Professional abstinence, coined by Biggs et al., 8 is defined as “consciously choosing not to provide the full scope of patient care activities” where competent and enabled to do so otherwise. In a call to action, the National Association of Pharmacy Regulatory Authorities (NAPRA) released a white paper attributing this phenomenon to a “weakening of the culture of professionalism in pharmacy practice” that is “impacting the ability of the profession to best meet the needs of patients and the health care system”. 9
Mise En Pratique Des Connaissances
L’abstinence professionnelle se définit comme « le choix délibéré de ne pas offrir l’ensemble de la gamme d’activités de soins aux patients » et perdure dans l’ensemble de la pratique pharmaceutique.
Compte tenu du rôle important que joue le mentorat dans le développement de l’identité professionnelle et des compétences des étudiants en pharmacie, nous avons cherché à comprendre l’incidence de l’abstinence professionnelle sur ces derniers.
Nous avons constaté que les étudiants en pharmacie de l’ensemble du Canada éprouvent deux sentiments contradictoires : l’espoir dans leur capacité à appliquer toutes leurs compétences à leur exercice de la pharmacie et l’accablement face à la responsabilité d’être des acteurs du changement. Les étudiants en pharmacie ont mentionné une dissonance cognitive permanente entre ce qu’on leur enseigne dans les facultés de pharmacie et ce qu’ils observent dans la pratique.
Les étudiants ont proposé plusieurs solutions à l’abstinence professionnelle, reflétant leurs responsabilités en tant que professionnels de se développer continuellement et de défendre leur profession, ainsi que de s’entourer de praticiens aux vues similaires s’efforçant de relever les défis dans la pratique.
The resulting faction of “abstainers” who demonstrate diminished engagement with professional activities likely also provides suboptimal patient care.9,10 They may also impact pharmacy students who, when exposed to professional abstinence, have a shift in their developing professional identity, potentially disengaging them from the full scope of practice even before they graduate.10,11 Pharmacy students across Canada are being trained to practice to full scope and look to their preceptors and work colleagues to equip them with the opportunity to practice the skills they need to deliver optimal patient-centred care and witness what they learn in school in real-life practice settings. However, exposure to professional abstinence can lead to tensions, wherein the students experience cognitive dissonance due to the discordance between what they are taught in school and what they observe in practice.10,11 Cognitive dissonance theory purports that there is a discrepancy between what you are learning and pre-existing knowledge that causes discomfort for a person. 12 This disconnect in learning and knowledge can provide a “provocative moment” in pharmacy student education that can help to develop their identities. 13 Additionally, professional abstinence has the potential to breed new generations of “abstainers” who are not providing a full scope of practice and services to patients. 10 An example of the cognitive dissonance that exists for pharmacy students is when what they learn in pharmacy school is met with resistance from preceptors responsible for fostering and complementing their learning, with comments like “that’s not what we do in the real world”. Students are the future changemakers of the pharmacy profession and are uniquely positioned to provide their perspectives on professional abstinence. 10 But their professional identity can be undermined or changed by their experiences in community pharmacy placements and rotations.
The purpose of this study is to explore pharmacy students’ experiences with and perspectives on professional abstinence in community pharmacies and what they see as their role in addressing it.
Methods
Study design
Using the lens of cognitive dissonance theory in student learning, a qualitative, semistructured interview study design was chosen to investigate pharmacy students’ experiences with and perspectives on observations of professional abstinence in community practice settings. This study follows the Consolidated Criteria for Reporting Qualitative Research (COREQ). 14
Data collection
All pharmacy students enrolled at an accredited Canadian pharmacy school who had previous experience at a community practice site either during their clinical rotations or placement and/or their pharmacy student jobs were eligible to take part in the study. Interviews were conducted between March and November 2021. The Canadian Association of Pharmacy Students and Interns (CAPSI) helped distribute recruitment postcards and provided information about the study to their members through email. Recruitment also proceeded through posting on social media and word of mouth. Information on who was conducting the interviews and the purpose of the research was provided to potential participants through an information letter. Students were selected serially until thematic saturation was reached and no new themes were being discussed. This was determined by the research student who conducted all the interviews as she was familiar with their content.
Participants who provided consent to participate in the study underwent a 30- to 60-minute semistructured, virtual 1:1 interview on Zoom conducted by a trained pharmacy research student. The interview guide included closed-ended questions regarding general demographic information and open-ended pharmacy experience questions (Appendix, available online in Supplementary Materials). The guide was designed to be inclusive of the entire spectrum of the student’s potential experiences, with questions written using an iterative process grounded in the concept of professional abstinence as defined by Biggs et al. 8 and the research student’s own experiences in a community setting. Field notes, including free written reflections, were made following interviews. Transcripts were not returned to participants for comment and/or correction unless requested.
Demographic information collected included the province of study and the participant’s expected year of graduation. The open-ended questions explored the student’s understanding of and experience with a pharmacist’s full scope of practice in their province, an explanation of the definition of professional abstinence, student experiences with it, its impact upon their professional identity, and any suggestions they had for addressing it.
Data analysis
Analysis of each transcribed interview was initially conducted by the trained undergraduate pharmacy student (Q.W.) using inductive coding to determine the codes, categories, and themes regarding student experiences and perceptions of professional abstinence. Manual coding followed a 3-stage process consisting of open coding, pattern coding, and abstraction, following the methodology outlined in The Coding Manual for Qualitative Researchers by Saldaña using Google Workspace. 15 The first stage, open coding, consisted of parsing through the transcripts using specifically the descriptive and “in vivo” approach. 15 In the second stage, pattern coding was applied, where the textual data obtained from the first stage were analyzed and collapsed into categories based on similarities. The last stage, abstraction, drew on the information established in the previous stages to form themes. A second undergraduate research student independently conducted the data analysis, with coding confirmed and refined by senior members of the research team. The researchers met after the first few transcripts to create a coding manual for the subsequent transcripts. The final themes and subthemes were applied to the full data set, and representative quotes were extracted. Participants did not have the opportunity to provide feedback on the findings. Trustworthiness of data was maintained through audit trails, peer briefing, investigator triangulation, and reflexivity. 16
In terms of reflexivity and researcher bias, the entire research team comprised pharmacists and pharmacy students who had practice experience in a variety of settings and experience in pharmacy practice research. As researchers, we all bring a bias of wanting to elevate pharmacy practice by investigating ways to support pharmacists and pharmacy students to practice to the top of their scope.
This project received approval from the University of Alberta Research Ethics Board (Pro00103909).
Results
Demographics
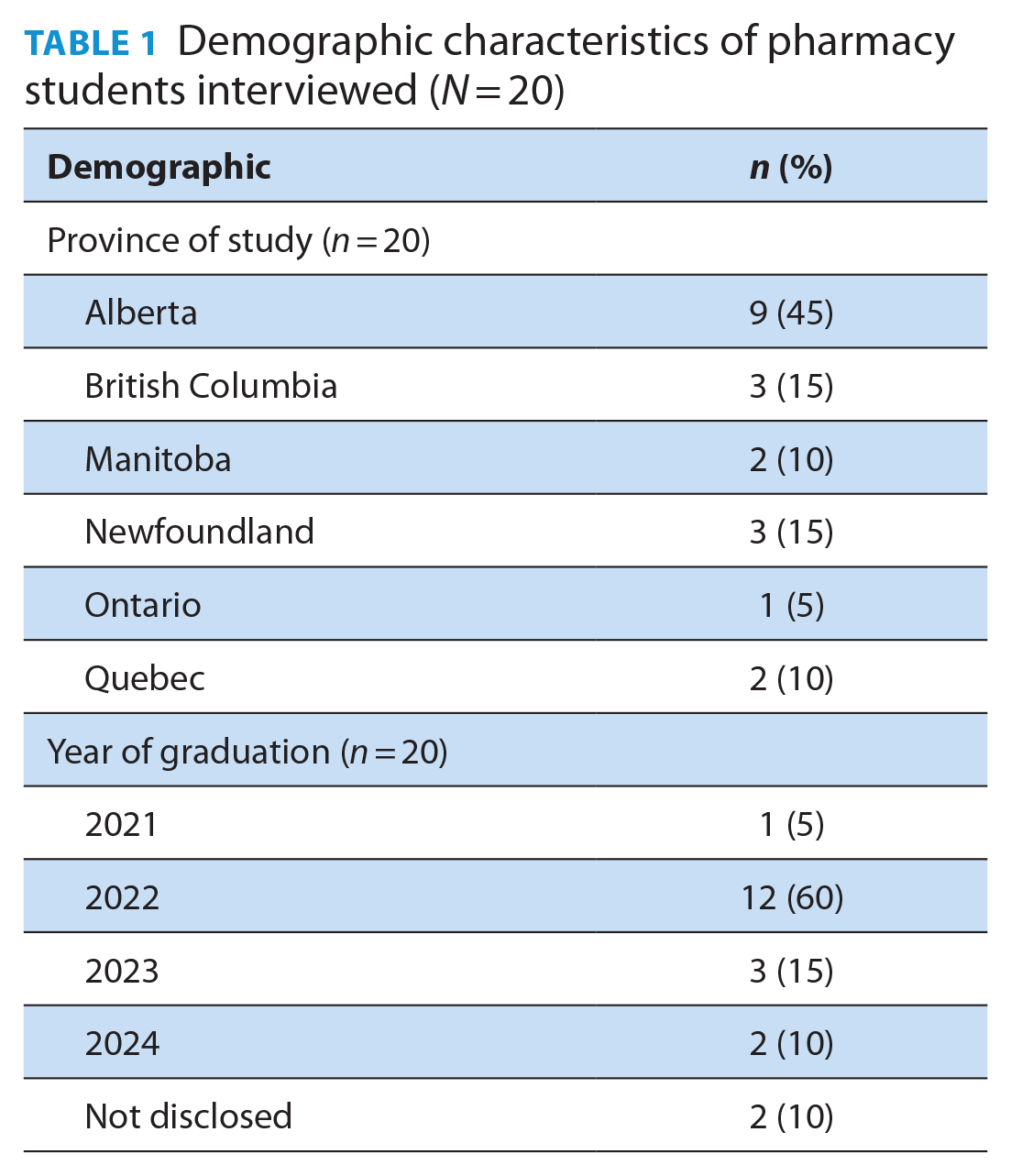
Twenty respondents who met the inclusion criteria and consented to participate in the study were included. Participant demographics are summarized in Table 1. Most students were from the University of Alberta (n = 9) and in their third year of study at the time of the interviews (n = 12). After 20 interviews, thematic saturation was reached; therefore, no other interviews were scheduled. No participants withdrew consent from the study.
Demographic characteristics of pharmacy students interviewed (N = 20)
Thematic analysis
The themes generated from the data were divided into 2 categories. The first category was students’ experiences with professional abstinence, and the second category described potential solutions to professional abstinence, each with 2 themes and 2 or 3 further subthemes, represented in Figure 1. It demonstrated the balance between students’ experiences with professional abstinence and the solutions they proposed to address it moving forward. Each of these themes and subthemes are further described below.
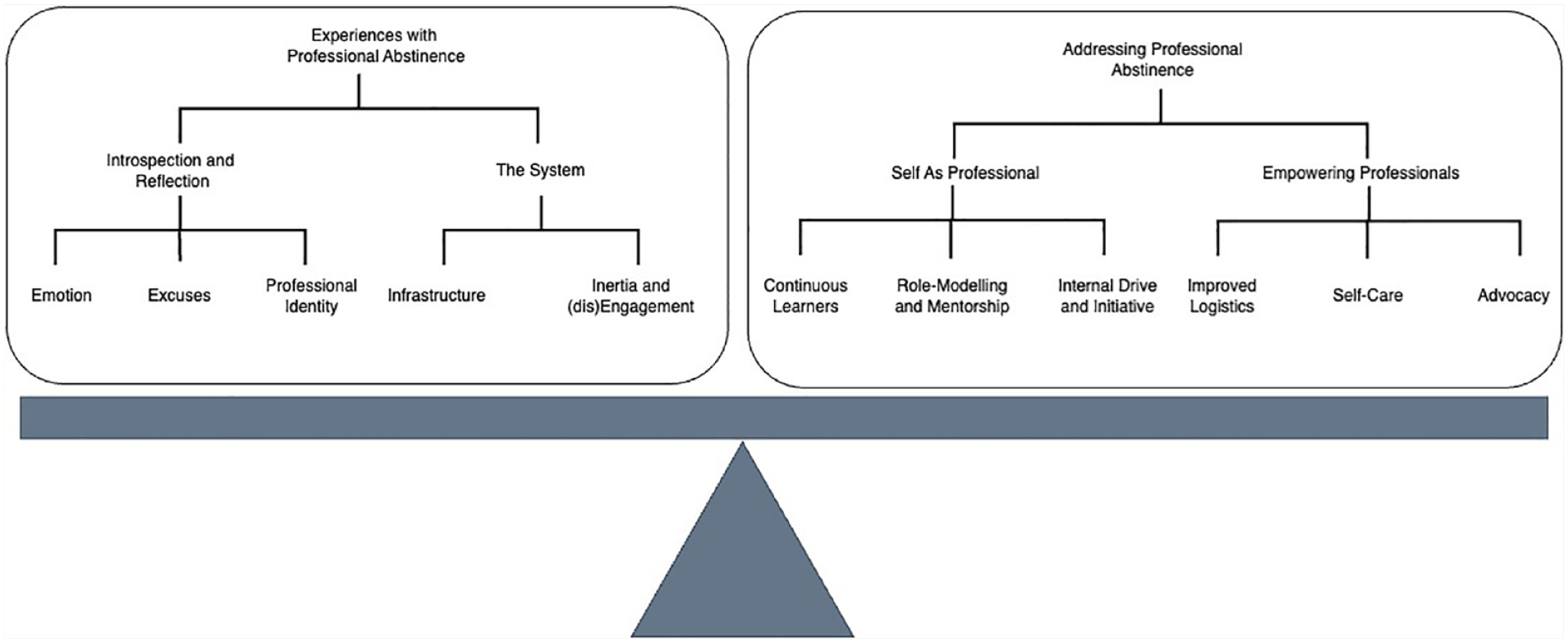
Relationship between themes and subthemes of pharmacy students’ experiences with professional abstinence
Two major themes were identified with the student experiences: 1) introspection and reflection and 2) the system (Table 2, Figure 1). For these participants, experiencing professional abstinence forced them to turn inward to reflect on how they see themselves as emerging pharmacists. Additionally, some of the rationale for the observed professional abstinence was attributed to environmental factors within the health care system and outside of a pharmacist’s control.
Themes and subthemes when pharmacy students were asked to share their experiences with and perspectives on professional abstinence
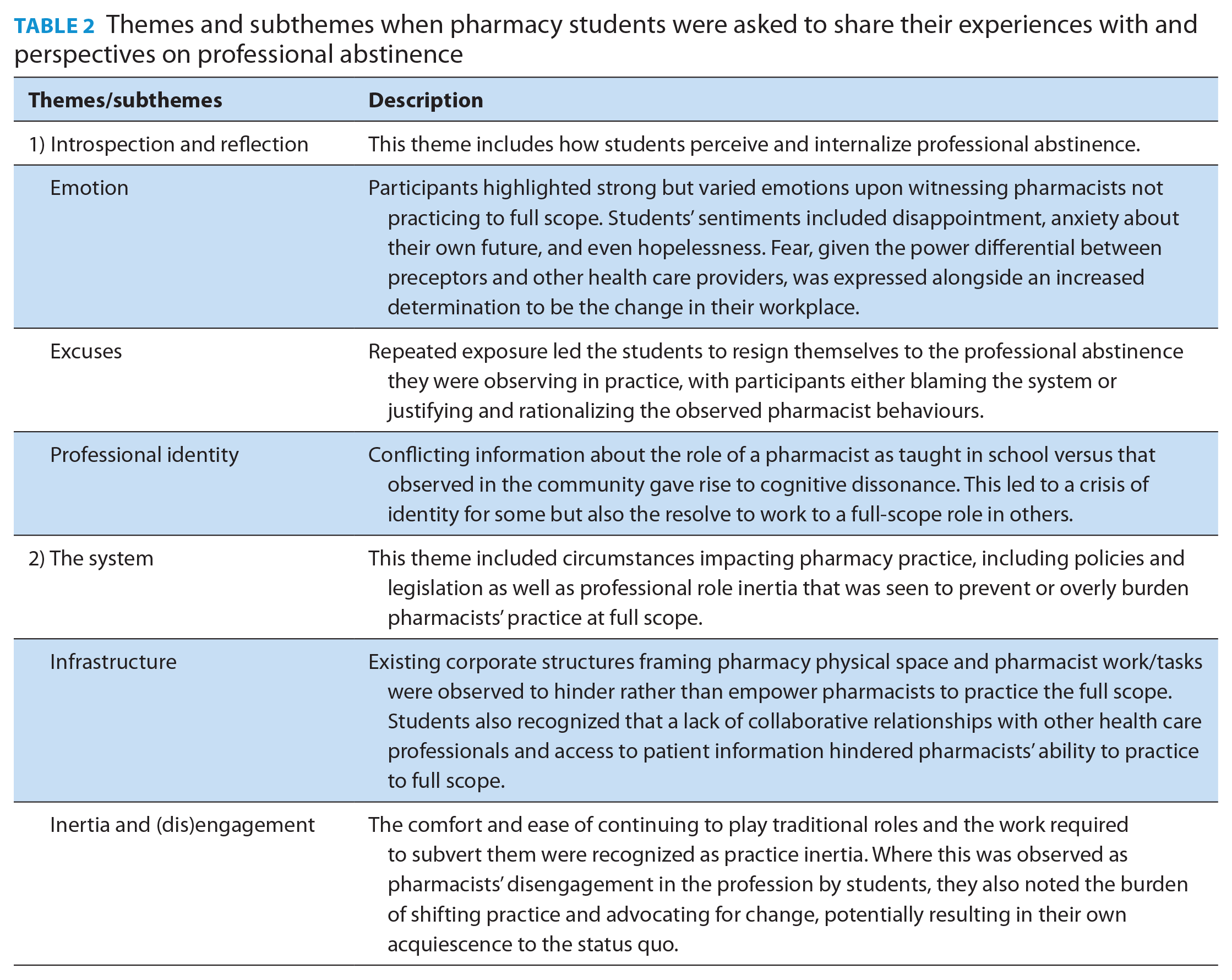
Introspection and reflection
Students described the significance of observing professional abstinence on their psyche in the theme of introspection and reflection. The subthemes included emotions, excuses, and professional identity.
In the subtheme of emotions, students recalled circumstances where they observed professional abstinence and how that made them feel. Some felt that professional abstinence was “borderline . . . unethical”, and others were disappointed that pharmacists were not maximizing their benefit for patients when full scope was not practiced. One participant stated that they felt useless when working in a pharmacy where full scope is not used, and it’s “harder for me to feel like I’m doing something good”. Students also expressed some anxiety about their future, noting in various ways that practicing at the full scope is the ideal, but given what they have observed in practice, they see full scope as a romantic notion, an unattainable goal, and certainly not a current reality. One student felt hopeless after they had attempted to intervene through the provincial regulator when professional abstinence was witnessed at their workplace and no observable action was taken. Another expressed confusion with discordant decisions, where the same pharmacist would provide a specific service for 1 patient but not another, stating, “I’m never quite sure what exactly the thought process is there”. Fear was another identified emotion. Some students expressed a fear of backlash when they challenged abstainers, given the power imbalance between preceptors/supervisors and students. Other students shared concerns that they heard about negative repercussions from both physicians and patients concerning pharmacists’ use of a full scope of practice. One student stated their motivation to use full scope was out of fear that these expanded roles might get taken away if there is not enough uptake among pharmacists, while another emphasized pharmacists’ fear of liability when taking on responsibility for patient care decisions.
Students both observed and expressed a variety of excuses for professional abstinence. They identified a range of barriers present in the community pharmacy, including time pressures, competing demands, limited compensation, and a lack of infrastructure as reasons why professional abstinence was observed and rationalized. However, students also noted that 2 pharmacists working in the same environment may exhibit completely different practice behaviours, emphasizing that professional abstinence is related to the autonomous choice by a pharmacist of how to approach practice. Other excuses focused on the pharmacists themselves, including their comfort and confidence level, skill set and training, or that established practitioners cannot change, with 1 student expressing: “Yeah, so it really comes down to the pharmacist as well. First of all, a lot of them have varying levels of comfortability with the situation and with prescribing and all that”. However, despite observing abstinent behaviours, students also expressed optimism for what the next generation of pharmacists will achieve in practice, given their education and role modelling in school.
Students were cognizant of the important role professional identity plays in abstinence from full-scope activities. They made note of the roles they saw pharmacists in community settings playing and the value they placed on them, for example, as dispensers performing technical tasks, and how that differed from their own developing identity. Participants shared how their own sense of professional identity was influenced by the values, responsibilities, and ethical standards of their pharmacy school as “education really pushes [you] to try and learn what [the] scope is . . . and by that merit it also makes [you] want to do it in practice”. Students expressed eagerness to perform the full scope but felt disappointed when pharmacists were “[not] given the opportunity to really excel as the drug experts” in the pharmacy practice they were immersed in and even “felt a little bit like being a cashier”. When students observe professional abstinence modelled by people they trust and respect, they may begin to internalize it. One participant noted, “[This is what] my preceptor did, so it becomes easy to rationalize it in your head and become complacent . . . and maybe even a little bit lazy”. Nevertheless, some participants pushed back against these sentiments, stating that as pharmacists are the most accessible health care professionals in the community, they planned to “form [their] own identity” as collaborative health care practitioners and “be more independent and develop confidence in [their] decisions”. One student expressed frustration with not having appropriate mentorship for the development of their professional identity, noting that the burden is on them to navigate full-scope roles and responsibilities.
The system
This theme outlines issues inherent to the health care system and human behaviour in times of change. The subthemes include infrastructure along with inertia and (dis)engagement.
Infrastructure: It was observed by participants that the environment in which pharmacists practice has a large impact on the degree to which they are able to work at full scope. Some observations included that there is “a lot of pressure from corporate office . . . to do a certain amount of clinical services”, that there is limited time for but also that specific “stores [have] a policy to not do [a] particular subset of their scope”. Participants noted that many of the barriers they identified were those over which an individual pharmacist had no control. Concerns were raised about physical space (e.g., spaces not being private enough for patients who need more comprehensive work-ups). Pharmacy policies outlining the type and number of staff may also impact pharmacist behaviour, with 1 student stating that if pharmacists “are not eating lunch, not taking breaks, not having time to use the bathroom” due to lack of shift overlap, they would not be in the best mindset to make clinical judgments that impact their patient’s health.
Pharmacists’ inability to access a patient’s laboratory and other diagnostic test results in some jurisdictions was recognized as a barrier, with 1 student expressing that: “The lack of access to the entire, I guess, medical record of a patient, or an important aspect of the patient, kind of places pharmacists in a position where they maybe don’t feel like they’re equipped to take on these big decisions for [patient] care”. Students noted that pharmacists may have deferred decision-making if they felt they did not have all the patient information they required or to avoid conflict with other health care professionals.
Inertia and (dis)engagement: In this subtheme, participants observed the tendency for themselves and pharmacists to keep on practicing in the way that they had always practiced, in order to not cause any issues in their workplace. For example, even where students could see that pharmacy workflow could be optimized to embrace more clinical services, students “didn’t want to disrupt what the current pharmacists were doing just because [they] were young and new [and other pharmacists] have seniority in working, experience-wise”, resulting in practice inertia. Students also mentioned that “strained relationships with . . . other health care professionals” who may believe that pharmacists are straying out of their purview held their preceptor back from completing clinical activities traditionally performed by another health care professional. One student stated: “Despite understanding the scope, I think my perceptions kind of come from the fact that I know how strained relationships can be with other health care professionals . . . where doctors aren’t always happy with us making changes, making, I guess, decisions on behalf of patients that they deem to be ‘their own’, per se”—again, suppressing change.
Confidence was also seen as connected to professional abstinence in terms of being related to engagement with practice change. Practicing to full scope means taking on more accountability and liability, putting in “more effort” and, ultimately, standing behind the clinical decisions one makes. One student spoke about how fear of responsibility and the pharmacist’s own professional (or role?) identity can dictate actions taken, stating: “If a patient was consistently getting [an inhaler] renewed by a pharmacist, [this specific] pharmacist would usually say they need to be reassessed by the doctor even though I guess technically as pharmacists we could also assess how their COPD or asthma is”, suggesting the pharmacist may not see themselves as responsible primary care providers. Likewise, students noted that when they observed professional abstinence in practice, it “[takes] a little stab at [your own] professional confidence”, which may disengage them from performing the full scope in the future.
The work of pushing pharmacists to expand the roles they have traditionally held and that are well-entrenched in professional culture, such as that of the medication dispenser, was noted to be overwhelming. Some students expressed concern with the burden that comes with being expected to be the agents of change and advocating for practice change. One student stated: “You’re the [student] trying to describe it to people and make it comprehensible and educate patients, educate policy makers, educate different pharmacists. It becomes almost like a whole other job on the side.” One student stated, “When we’re so used to seeing what we see in practice with some of the pharmacists that we have worked with or some of the preceptors we’ve had on rotations . . . I feel like there is not proper mentorship for students and . . . sometimes I feel like we don’t know where to go when we haven’t been seeing this in real life.”
Students’ suggestions for addressing professional abstinence
Students proposed various strategies in response to their observations of professional abstinence, which were aligned either with the theme of 1) self as a professional or 2) empowering the professional (Table 3, Figure 1). Through their experiences with professional abstinence, participants contrived plans for how they would stay engaged and work toward full-scope practice while recognizing the personal and system supports they would need to do so.
Themes and subthemes when pharmacy students were asked how to address professional abstinence
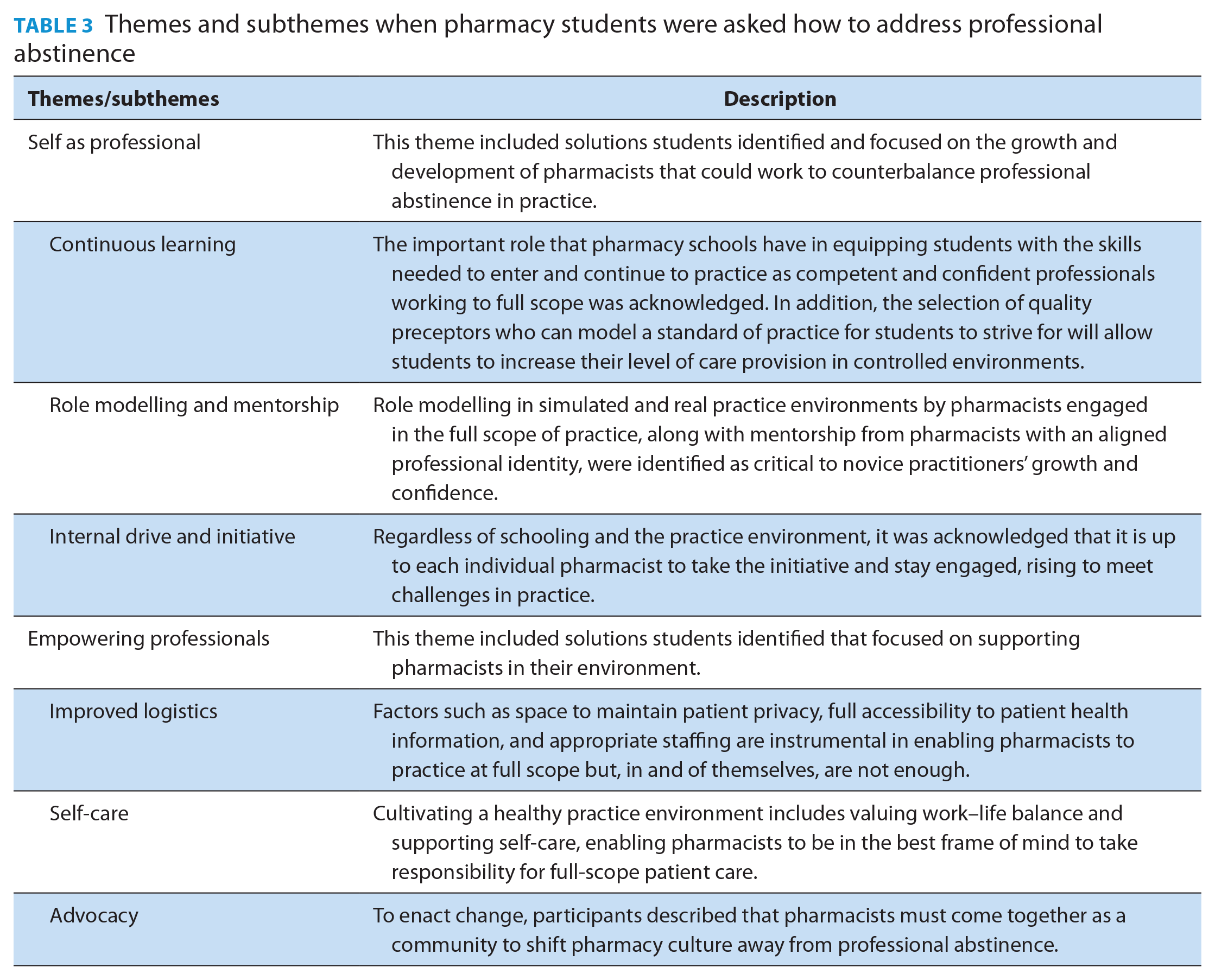
Self as professional: Students recognized that pharmacists have a responsibility to be continuous learners as part of their ethical obligation to their patients and their profession. While it is not possible to be prepared for every scenario one might encounter in patient care, 1 student noted that rather than deferring responsibility, “Those are good opportunities to learn from a situation and to realize your own weaknesses and self-evaluate your skills [which] . . . probe you to perhaps learn more about that topic or learn how you could have better handled that”. Participants recognized that while students have a role in their own learning, they suggested that pharmacy schools should be providing opportunities for them to take increasing degrees of responsibility for care in patient care skills labs and on experiential placements, with the aim of increasing both competence and confidence with the full scope of practice at graduation.
Role modelling and mentorship were also identified as critical to improving students’ confidence in patient care, as well as learning to determine when to refer to another care provider. Recognizing that role modelling and guidance are provided to students in the classroom and on placements, 1 proposed solution was a more careful selection of preceptors who practice to full scope. This may further enable reciprocal learning, where students can learn from quality preceptors who are keen to learn more about “the latest research, where practice is headed”, and who are open to alternative approaches students may come up with. Being in an environment where mentors are practicing to full scope has great potential to impact a student’s future practice. For example, 1 student stated: “Seeing a lot of initial access prescribing did create some discomfort for me as well, because it is an important role and there is a lot more room for error when you’re prescribing versus not prescribing as often, so it did kind of feel a little uncomfortable but I think it was a good uncomfortable because it was an area for growth.”
Participants also noted internal drive and initiative as essential in changing practice and culture. Rather than defaulting to the professional abstinence that they may observe, 1 participant noted, “I might not be able to change how other pharmacists are practicing but I really make sure that I am doing what I can personally do to help patients.”
Empowering professionals: Students recognized in their interviews that pharmacists need to be empowered to practice to full scope in supportive environments. Recognizing several systemic barriers, students pressed for improved logistics, including access to patient care records, such as lab tests, and structural changes to the design of the dispensary, to provide for private spaces for patient assessment and counselling. They also recommended a streamlined workflow by having the right professional performing the right work, including pharmacy technicians taking responsibility for appropriate prescription filling as per their scope of practice. One student proposed “that the pharmacist delegating some of their other responsibilities [would enable them to] then spend [the time needed] with the patient in the counselling room”. Related to this was the suggestion to improve staffing, with 1 student stating that “having more than 1 pharmacist working at a time can be really helpful. I know that is not always feasible but, even having some overlap, for example, between shifts” could allow for pharmacists to engage in the clinical aspects of the dispensing role and in other services such as medication reviews and chronic disease management.
Improved staffing could also impact the not-so-hidden lack of self-care that pervades community pharmacy settings. One participant advocated for pharmacy programs to include education on work–life balance and self-care given professional abstinence may be an unintended consequence of poor work culture: “reminding pharmacists that we are humans and we need to have breaks and take care of ourselves so we can practice to our full scope to keep our patients safe and put them first”.
Students identified further advocacy pathways that they felt could impact professional abstinence. They noted that, as a profession, pharmacists must advocate for a shift in pharmacy culture to exclude professional abstinence. This includes increasing the broader community’s awareness of the term professional abstinence and its definition and building a support network. One suggestion was that it is “important to [find] those [like-minded] people . . . to keep yourself motivated” to achieve shared goals and to “keep advocating for policy changes [because] we have all the knowledge we need, we just kind of need policy to be on our side” to give patients the best possible care.
Discussion
The primary objective of this study was to explore the experiences students had in observing professional abstinence in community pharmacy practice, along with any suggestions for potential solutions. Our findings indicate that when students experienced professional abstinence on a practicum placement or at work in community settings, it caused them to turn introspective and reflect on their experiences of observing professional abstinence and how that fits with their own developing professional identity of what and who a pharmacist is, as well as to consider contributors within the existing system and infrastructure.
It was clear from the data that students held 2 competing feelings: hopeful in their own ability to practice to full scope and burdened by the responsibility to be changemakers. Participants recognized that they themselves need to take responsibility within their own practices, exercising self-determination for what their practices look like. But with that, participants recognized that as the next generation of practitioners, they were also viewed as somewhat responsible for changing the whole of pharmacy practice. They saw the ease with which abstinent pharmacists deferred responsibility and struggled with the “why”. The suspected uneasiness of taking on the accountability and responsibility as the primary health care decision-maker has been identified as a hindrance or resistance to practice change. For some, it may be the weight of taking responsibility for decisions.17-19 For others, it may be the burdens associated with the existing community practice setting: high-volume dispensaries, imposed quotas for clinical services that the pharmacy is not well set up structurally or personnel-wise, and a “customer” rather than “health care”-oriented attitude from patients. These factors have been shown to contribute to burnout and may be a big part of why efforts with practice change are not getting better.20-22 Interrelated to these concepts is the phenomenon of pharmacists recognizing themselves as primary care providers; even pharmacists who work in integrated primary care teams more often identify as being supportive in their roles than providing direct patient care. 23 Pharmacists are often the first point of contact for patients seeking care, yet pharmacists do not routinely consider themselves their primary care provider or clinician. 24
The tension between competing feelings about participants’ future practice was also identified in the development of their professional identity. Students discussed an ongoing cognitive dissonance between what they were being taught in their undergraduate education and what they were observing and experiencing in practice. This is not a new finding, with Noble et al. 25 describing this phenomenon as early as 2015. However, almost 10 years forward, educators are still struggling with how to help students navigate this dissonance. Reflection has been identified as critical in professional identity development and cognitive dissonance; faculty and preceptors need to provide students with the opportunity to debrief these disconnects, offering support and knowledge from our own experiences as educators. 25 As described previously, professional identity formation can be facilitated by an experience of a “crisis” that prompts the student to progress along their growth trajectory. 26 These experiences of professional abstinence can serve as that critical event, whereafter faculty can help students make sense of the experience through reflection, dialogue, and other pedagogical approaches. 27
Although students described feelings of frustration and fear in taking on expanded scope opportunities in environments that may not support them, none of the participants expressed anger about the lack of change. Instead, they more often came up with excuses for why it is, why change has not been wide-sweeping, and why pharmacists engage in professional abstinence. This is a particularly interesting finding that we postulate might be related to the fact that as students, they are looking for ways in which to be a part of the “community”—an important step in professional identity formation.28,29 As students are trying on different identities present in the professional community, they may experience feelings of comradery around how difficult it is to work in the current practice environment. 26 In thinking and feeling like the pharmacists they work with, students may see an easier path in joining that community, adopting practice inertia, and losing the motivation to be a force of change. Moreover, participants’ actions in response to observations of professional abstinence highlight the clear power differential between students and pharmacists, leading to acquiescence rather than change. To help close that power gap, students may want to create shared experiences with the pharmacists, and therefore excuse-finding becomes a way to achieve that.
So, what does this all mean for the future of pharmacy practice and education? There is no one quick-fix solution to professional abstinence. Pharmacy educators have long held the view that by teaching students to practice to the fullest possible scope upon graduation, that practice will change. Our results refute this belief, as on its own, it is not enough. Students feel the pressure of being these agents of change while at the same time trying to fit into the community of practitioners, with some holding fast to the status quo. Even with the changes in the scope of practice across Canada, it is clear that these structural and policy changes do not in and of themselves bring about a monumental shift in practice. 30 Pharmacists being granted access to further information, such as lab values, does not in and of itself change practice; so many other factors at play interrupt that shift.
As pharmacy educators, we should be preparing students to practice to full scope while also acknowledging and sharing with them that they will experience different practices that both propel and inhibit practice change. We need to do our best to support the development of their professional identities and empower them with the knowledge, skills, and attitudes to feel confident to be autonomous practitioners who can effect change 1 patient at a time. In addition to the education of students, the pharmacy community needs to adopt a growth mindset and develop strategies to take responsibility for decision-making. Developing a growth mindset has been explored from a student’s perspective; 31 however, we likely need to also investigate how to help practitioners in this regard.
Self-care was indicated as an important solution by students, and part of this includes developing a culture of well-being for pharmacists and pharmacy staff. 20 However, self-care must be accompanied by organization-level interventions to promote autonomy, purpose, and recognition. Together, they contribute to the engagement of pharmacy professionals, which is considered a key tenet of professionalism itself. 32 Adequate staffing is a structural barrier to managing burnout in pharmacists but could also be a solution to reducing the frequency of professional abstinence in practice settings where it is observed. Further research in this area could explore other strategies for the structure and function of pharmacies.
A key limitation of this study is that most respondents come from 1 institution and may reflect the practice of that particular province. Interestingly, the province most commonly represented was Alberta, which has the broadest scope of practice in Canada, and the assumption would be that students practicing there would be more likely to see expanded scope. 33 Another limitation is recall bias, with participants recalling observations that were more formative in their practice experiences, such as instances that challenged their expectations of practice as framed in their undergraduate course, creating dissonance. We also must acknowledge that the data were collected more than 3 years ago; while practice has continued to change throughout Canada, student feedback gathered following community setting placements at our school remains aligned. Finally, the current study provides no insight into the prevalence of professional abstinence in community practice or its impact on practicing pharmacists.
In conclusion, pharmacy students are feeling the pressure to change practice and to fit into the current practice structure. As we move forward with advanced practice, we need to consider the role of pharmacy students in these endeavours and how we can help them manage the cognitive dissonance that comes with these competing roles. ■
Supplemental Material
sj-pdf-1-cph-10.1177_17151635241306458 – Supplemental material for Navigating the influence of professional abstinence on pharmacy students: Observations and solutions from their perspective
Supplemental material, sj-pdf-1-cph-10.1177_17151635241306458 for Navigating the influence of professional abstinence on pharmacy students: Observations and solutions from their perspective by Jill J. Hall, Haley Tong, Kaitlyn E. Watson, Ross T. Tsuyuki, Catherine Biggs and Theresa L. Charrois in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Acknowledgements
We thank Queeny Wu, who initiated this project and led data collection and interpretation, and thank Hoda Borno for her contributions to data analysis.
Note: Since completing the research, Theresa L. Charrois has moved to the Faculty of Pharmaceutical Sciences at the University of British Columbia, and Kaitlyn Watson has moved to the Faculty of Pharmacy and Pharmaceutical Sciences at the University of Alberta.
Declaration of Conflicts of Interest:
Ross T. Tsuyuki is the Editor-in-Chief of the Canadian Pharmacists Journal.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements:
This project received approval from the University of Alberta Research Ethics Board (Pro00103909). Participants were provided with a digital copy of an information sheet and provided verbal consent.
Data Availability Statement:
The data supporting this study’s findings are available from the corresponding author, J.J.H., upon reasonable request.
Supplemental Material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.