
Abstract
Background:
Despite the shift towards direct-acting anticoagulants, warfarin remains widely used in Canada and is traditionally managed by family physicians through laboratory-based international normalized ratio (INR) testing. The Community Pharmacy Anticoagulation Management Service (CPAMS) in Nova Scotia represents an innovative approach, enabling community pharmacists to conduct point-of-care (POC) INR testing and manage warfarin therapy. A potential benefit of this approach is the opportunity to identify non-warfarin medication therapy problems (nwMTPs) during routine visits.
Method:
We conducted a prospective, multicentre, observational study across 40 community pharmacies in Nova Scotia, part of CPAMS’s second phase. Pharmacists documented nwMTPs identified in patients with atrial fibrillation during routine POC INR visits using the Qualtrics Insight Platform, categorizing them by indication, effectiveness, safety, or adherence, alongside corresponding interventions.
Results:
Over 6 months, 43 nwMTPs were submitted from 13 unique pharmacies. There were 3404 POC INR tests in patients with atrial fibrillation, yielding an estimated nwMTP detection rate of 1.26 (95% CI, 0.69 to 2.32) per 100 INR tests. The most common nwMTP category was “Indication,” primarily requiring additional therapy. Pharmacists frequently intervened by recommending medication adjustments or providing patient education.
Discussion:
The findings highlight a modest, yet potentially significant role of pharmacists in detecting and managing diverse MTPs during focused warfarin management assessments. The predominance of indication-related problems underscores unmet therapeutic needs in patients on warfarin.
Conclusion:
This study illustrates the potential of pharmacist-led POC INR testing in community settings to identify and address nwMTPs, contributing to comprehensive patient care.
Knowledge into Practice
Community pharmacists managing warfarin therapy with point-of-care international normalized ratio (POC INR) testing identified 1.26 non-warfarin-related medication therapy problems (nwMTPs) per 100 visits, with the most common being issues of indication.
The primary pharmacist intervention was to recommend starting or stopping a medication.
This ability to address nwMTPs during POC INR visits highlights a potentially significant, previously unrecognized benefit, contributing to improved health outcomes and reducing strain on the health care system.
Background
Although warfarin is no longer the first-line oral anticoagulation recommended for stroke risk reduction for atrial fibrillation, it is still used by a significant number of Canadians. 1 Traditionally, patients taking warfarin are managed by their family physician, who is responsible for reviewing the results of venipuncture international normalized ratio (INR) tests performed at community laboratories and contacting the patient with any recommended warfarin dosage changes. More recently, community pharmacists in Canada have been providing warfarin management services using point-of-care (POC) INR testing. 2 A review published by the Canadian Agency for Drug and Health Technology (CADTH) reported that the use of POC coagulometers was associated with increased time spent in therapeutic range (TTR) by an average of 6.14% compared to laboratory-based INR monitoring. 3 Two evaluations of the effectiveness of pharmacist-led warfarin management that used POC coagulometers reported significantly better TTRs than those studies that did not.2,4 -8
Besides the possible improved quality of warfarin management, POC INR testing offers other benefits that may improve the overall quality of care provided to patients taking warfarin. Seeing the patient face-to-face for the test provides the clinician with an enhanced opportunity for assessment of the patient’s health condition, their use of medications, and their understanding of instructions and education provided. In contrast, when patients have their INR tested at a laboratory, the clinician assessment is constrained because it usually takes place a day or 2 after the test, and it often occurs over the telephone. Anecdotally, clinicians who offer POC INR testing clinics report addressing various non-warfarin-related health issues at patient visits (e.g., managing heart failure exacerbations, addressing uncontrolled hypertension, and discussing alternatives for pain control).
Identifying and resolving these non-warfarin medication therapy problems (nwMTPs) may represent a significant additional benefit of POC INR testing. A search of PubMed and Google Scholar completed in October 2023 failed to find any studies describing this type of ancillary benefit from POC management of warfarin therapy. Before it is possible to determine whether these potential benefits lead to improved health outcomes, research is required to investigate the frequency and types of MTPs identified by community pharmacists at point-of-care INR visits by patients taking warfarin for atrial fibrillation.
Mise En Pratique Des Connaissances
Les pharmaciens communautaires qui gèrent le traitement par la warfarine à l’aide de la mesure du apport international normalisé au point de service (RIN au PDS) ont identifié 1,26 problème de traitement médicamenteux non lié à la warfarine par tranche de 100 visites, le plus courant étant un problème d’indication.
La principale intervention du pharmacien consistait à recommander de commencer ou d’arrêter un médicament.
Cette possibilité de traiter les problèmes de traitement médicamenteux non liés à la warfarine lors des visites pour la mesure du RIN au PDS souligne un avantage potentiellement important, et non reconnu jusqu’ici, qui contribue à améliorer les résultats en matière de santé et à réduire la pression sur le système de soins de santé.
Methods
The study population was derived from the Community Pharmacy Anticoagulation Management Services (CPAMS) project in Nova Scotia. Pharmacists participating in this program provide warfarin management services using POC INR testing and computerized decision support software (INR Online Canada). All pharmacists completed a course in warfarin management offered through the University of Waterloo, Ontario. We performed a prospective, multicentre, observational, descriptive study involving 40 community pharmacies in Nova Scotia who were part of the second phase of the CPAMS project. Pharmacists from these pharmacies were introduced to the study at a program launch webinar held on November 23, 2022. The webinar was recorded for pharmacists who were unable to attend.
Pharmacists at any of the 40 participating pharmacies were eligible to include patients with atrial fibrillation during their scheduled POC INR testing visits between November 28, 2022 and May 28, 2023. The indication for warfarin therapy, including atrial fibrillation diagnoses, was confirmed through each patient’s profile listed in the INR Online software. We focused on patients with atrial fibrillation because this indication represents the largest proportion of individuals enrolled in community-based warfarin clinics, and patients with atrial fibrillation tend to be older than individuals using warfarin for other indications, which may increase the risk for MTPs. 9 If the pharmacist, in their routine assessment of the patient, identified an nwMTP, they were asked to fill out a data collection survey using the Qualtrics Insight Platform (Qualtrics, Provo, UT, USA) to document the patient’s age and sex, the category of nwMTP (indication, effectiveness, safety, or adherence), 10 the most responsible medication involved, the most responsible medical condition or symptom involved, and the action taken to address the nwMTP. The pharmacists were incentivized to participate through a monthly draw for a $100 prepaid VISA card. Pharmacist names were not linked to the nwMTP entry. With each submission, pharmacists had the option to complete a separate survey to provide their name for the monthly prize draw.
Study definitions
Medication therapy problem (MTP): “An undesirable patient experience that involves drug therapy and that actually or potentially interferes with a desired patient outcome.” 11
Non-warfarin MTP (nwMTP): Any MTP that does not involve simply increasing or decreasing the dose of warfarin in response to an out-of-range INR value.
Statistical procedures
Descriptive statistics were used to summarize the sample characteristics, such as mean age and the percentage of female patients. The primary endpoint was the presence of an nwMTP identified by the pharmacist at a routine POC INR testing visit for patients with atrial fibrillation, expressed as the number of MTPs identified per 100 POC INR visits. To estimate the rate of nwMTPs detected per 100 INR tests, we employed a generalized estimating equations (GEE) model. This method provides population-averaged estimates and accounts for the clustering of data by pharmacy.
We included an offset term, defined as the natural logarithm of the number of INR tests conducted by each pharmacy, to model the rate of nwMTPs per 100 INR tests accurately. The GEE model was specified with a Poisson distribution, an independent correlation structure, and robust standard errors. The model was fitted using the “statsmodels” package in Python. The rate of nwMTP detection per 100 INR tests was derived by exponentiating the intercept term from the model.
Roche Canada provided each study site with a Coaguchek XS Pro device to assist with the study, but pharmacist participation in the research project was voluntary. INR Online Canada provided data regarding the number of tests performed on patients with atrial fibrillation during the study period.
Ethics approval
Ethics approval for this study was provided by the Office of Research Ethics at the University of Waterloo, Ontario on September 27, 2022 (ORE # 44492).
Results
At the start of the study, 62 pharmacists were providing warfarin management services at 40 community pharmacies. By the midpoint, 422 patients were enrolled in the CPAMS service at participating sites. The specific indication for therapy for each of these 422 patients was not available, but prior research involving the overall CPAMS program reported that approximately 70% of enrolled patients had atrial fibrillation. 2 Over the 6-month study window, a total of 43 nwMTPs were detected at routine INR testing visits for patients with atrial fibrillation. Thirty-five of the 40 pharmacies performed at least 1 INR test for a patient with atrial fibrillation during the study window, and 13 unique pharmacies submitted at least 1 MTP during the study period (Figure 1). There were 3404 POC INR tests performed for patients with atrial fibrillation at the 35 pharmacies reporting at least 1 test during the study. Using a GEE model to account for clustering by pharmacy, we estimated the rate of nwMTPs detected per 100 INR tests to be 1.26 (95% CI, 0.69 to 2.32).
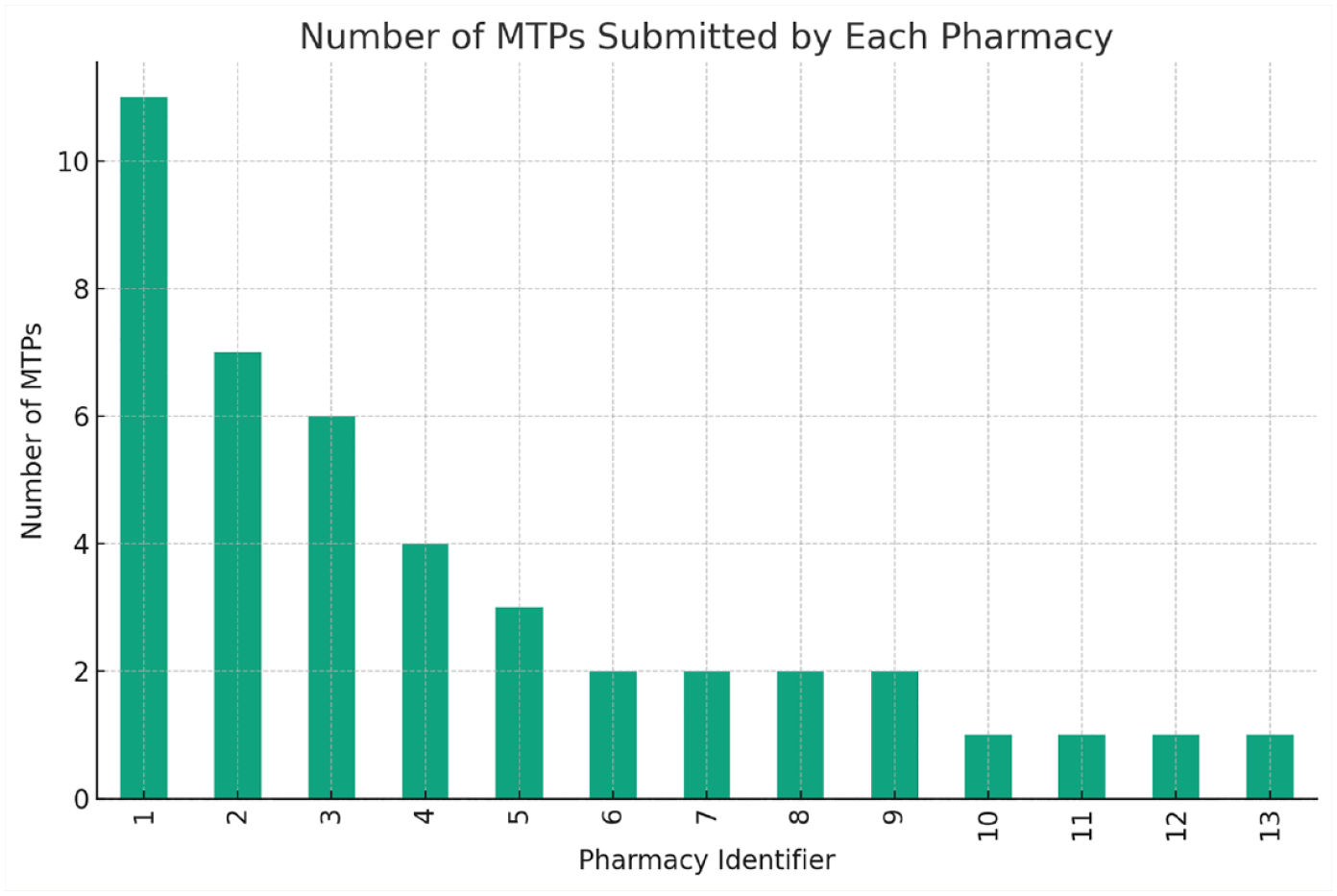
Frequency plot for the number of MTPs submitted by individual pharmacies
The average age of the patients who had a reported nwMTP was 74.1 (standard deviation [SD], 11.6 years), and 44% (19/43) of the nwMTPs were identified in female patients with atrial fibrillation.
Table 1 outlines the categorization of the highest-priority nwMTPs. The most common category was indication (44%), followed by safety (33%), effectiveness (16%), and adherence (7%), and the most common subcategory was the need for additional therapy (42%). The categories of most responsible medication classes and medical conditions or symptoms are found in Table 2. There was significant diversity in both the medication classes and medical conditions involved in the highest-priority nwMTP, with more than 9 classes of drugs and 11 classes of conditions or symptoms reported. The most common classes of medications included drugs that affect the blood and blood-forming organs (21%), anti-infectives for systemic use (14%), and drugs that affect the cardiovascular system (12%). Cardiovascular (40%), gastrointestinal (9%), respiratory (9%), and musculoskeletal (7%) were the most reported classes of conditions and symptoms.
The categories of the highest-priority nwMTPs detected at routine point-of-care INR test visits

INR, international normalized ratio; nwMTP, non-warfarin medication therapy problem.
The most responsible drugs and conditions or symptoms involved in the highest-priority MTPs

Classified using the Anatomical Therapeutic Chemical system.
MTP, medication therapy problem.
In general, pharmacists were able to address the nwMTPs without referring the patient to another health care provider. The presence of peripheral edema was the reason for referral to the patient’s family physician in all 4 cases requiring this intervention. The most common methods used to address the nwMTP included recommending the patient start or stop a non-prescription (30%) or prescription medication (16%) and providing education (14%) (Table 3).
Method used by the pharmacist to address the highest-priority nwMTP

nwMTP, non-warfarin medication therapy problem.
Discussion
In our review of anticoagulation visits, we estimated the rate of nwMTPs detected per 100 INR tests to be 1.26, with a 95% confidence interval of 0.69 to 2.32. We consider this a conservative estimate because only 13 of 35 pharmacies documented at least 1 nwMTP, and only 2 pharmacies contributed 42% of all nwMTPs reported. The rate of nwMTP detection is modest, but it is important to emphasize that these appointments are meant to be focused assessments of warfarin therapy. The average length of a POC INR testing visit in a previous CPAMS study was approximately 11 minutes. 12 Any nwMTPs detected at these appointments are an unintended benefit of POC testing and pharmacist-managed warfarin therapy. Because of the novelty of this research, we were unable to find any appropriate studies to compare the rate of nwMTP detection. It is not helpful to compare our results to other studies documenting rates of MTP detection by pharmacists because the primary purpose of the visit in all other studies we located was for medication management services or medication reviews—in other words, to specifically find MTPs. A more appropriate comparison would be against the rate of nwMTP detection when following the traditional method of warfarin management, in which patients attend a community laboratory for a venipuncture INR test and receive a phone call a day or 2 later with warfarin dosing instructions. Unfortunately, no such studies have been performed to our knowledge.
The most frequent category of nwMTP was indication, with the need for additional therapy being the most common subcategory. This may seem surprising, given the purpose of the appointment was for INR determination. Prior studies reporting on MTP detection by pharmacists suggest significant variability in the most common category and subcategories of MTPs. A systematic review suggested the most common subcategories of MTPs are the need for additional therapy (43 studies ranked it in their top 3), non-adherence (42 studies), and unnecessary therapy (28 studies). 10 Perhaps the closest study to ours involved a retrospective review of medical records to study pharmacists’ interventions in a specialized direct-oral anticoagulant (DOAC) follow-up clinic. 13 Patients requiring long-term therapy with a DOAC were referred to this clinic for pharmacist assessment within 6 months. The most common problems identified after pharmacist review were adverse drug reactions (30% of all problems), non-adherence (25%), and dose too high (20%). 13 Of note, pharmacists in this study used a standardized tool developed by their thrombosis team to assess patients. This likely explains the difference between the types of MTPs detected in their trial (i.e., focused on anticoagulant therapy) versus our study (i.e., focused only on non-warfarin-related MTPs). The fact that our study identified the need for additional therapy as the most common MTP may have significance with respect to the potential clinical and economic impact of this novel service by community pharmacists. Not only does CPAMS deliver high-quality warfarin-related care, 2 but pharmacists may also be contributing to improved health care efficiencies by identifying unmet medication needs in their patients. Nearly all nwMTPs were addressed by the pharmacist, which may prevent visits to overburdened family physicians and emergency departments and/or improve the management of comorbid conditions. For example, on 2 occasions, pharmacists in this study documented the administration of the influenza vaccine.
The most common action to address the highest-priority nwMTP was to recommend the patient start or stop a prescription or non-prescription medication. In a retrospective analysis of patients readmitted to hospital within 30 days of discharge, 50% of readmissions involved a medication-related problem, and the most common category was indication for therapy. 14 This study estimated nearly 30% of the possibly preventable readmissions were related to an untreated condition, lending support to the notion that actions taken by pharmacists in our study may provide important benefits. 14
The types of medications, medical conditions, and symptoms involved in the highest-priority nwMTPs are diverse. This is perhaps a previously unrecognized advantage of having community pharmacists managing warfarin therapy using POC INR testing. Not only did pharmacists in this study have the specialty training required to manage warfarin, but they also possessed significant breadth in their ability to recognize and manage a variety of common conditions seen in primary care. If the POC INR testing and warfarin management were supervised by thrombosis specialists, some of these opportunities like administering influenza vaccines, recommending treatment for urinary tract infections, or managing seasonal allergies may be missed.
Limitations
Our study has several limitations. The participation rate was lower than expected, with fewer than half of the pharmacies reporting at least 1 nwMTP. This could be due to several factors, including the novelty of the service for pharmacists, the busy season with vaccine clinics, and the time pressures of managing a POC INR clinic alongside dispensary duties. We limited the data collected to minimize the survey completion time but recognize that even a short survey can be challenging amid competing priorities. Future studies should consider providing additional staffing support to enhance data collection. 15 Our study did not have a control group, so we are unable to determine whether there are more nwMTPs detected in pharmacist-led POC INR clinics than are found in the traditional model of warfarin management. This should be considered in the design of subsequent research. Also, there was no attempt made to follow-up on whether the pharmacists’ recommendations were followed through or whether patient outcomes were improved. This precludes any assessment of the benefits associated with nwMTP detection at POC INR visits. In addition, the clinical importance of nwMTPs detected was not reviewed. Finally, we focused our study on patients with atrial fibrillation, and our results may not apply to patients seen at pharmacist-led POC INR clinics with other indications for warfarin therapy.
Conclusion
In conclusion, this preliminary study suggests that pharmacist-led POC INR testing may have the potential to detect nwMTPs in patients with atrial fibrillation. While the observed rate of nwMTP detection is modest, it indicates an additional benefit to routine warfarin management that could contribute to improved patient care. The findings also highlight the diverse role that community pharmacists can play in primary care settings. Further research is needed to validate these results and to explore the full impact of pharmacist-led POC INR testing on patient outcomes. ■
Footnotes
Author Contributions:
Jeff Nagge, Michelle Moussa, Lisa Woodill, and Joey Champigny contributed to the study conception and design, performed material preparation, and completed data collection. Data analysis and interpretation were performed by Jeff Nagge, Michelle Moussa, Lisa Woodill, Joey Champigny, and Amleset Zerai. The first draft of the manuscript was written by Jeff Nagge, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement:
Ethics approval for this study was provided by the Office of Research Ethics at the University of Waterloo, Ontario on September 27, 2022 (ORE # 44492).
Funding:
This study was supported by an equipment grant provided by Roche Diagnostics, Canada. The six $100 prepaid VISA cards used to incentivize participation were provided by the Pharmacy Association of Nova Scotia.