
Abstract
Background:
Lyme disease is a bacterial infection transmitted to humans through bites from infected Ixodes species of ticks. Prophylaxis with a single dose of oral doxycycline following a bite from an infected tick reduces the risk of developing Lyme disease. Pharmacists in Nova Scotia (NS) were among the first in Canada to prescribe for this indication. The primary objective of this study is to describe experiences with pharmacist prescribing of prophylaxis after tick bites in NS.
Methods:
A retrospective cohort study was performed using health administrative data 16 months before and after pharmacists were authorized to prescribe Lyme disease chemoprophylaxis (August 1, 2021). All dispensations of a single dose of oral doxycycline from a community pharmacy in NS were included. Data collected included prescriber type, date, and county of dispensation. Comparisons of dispensations were completed before and after pharmacists gained prescriptive authority and relative to other prescribers. Dispensations were described descriptively.
Results:
Over the study period, 12,549 single-dose doxycycline prescriptions were dispensed in NS: 3900 prescriptions were dispensed before pharmacist prescribing authorization for this indication occurred and 8649 were dispensed after. Pharmacists prescribed 61.3% of all single-dose doxycycline prescriptions following implementation of prescribing authority.
Discussion:
An increase in single-dose doxycycline prescriptions was observed in NS. Pharmacists have become the primary prescribers for Lyme disease chemoprophylaxis in the province.
Conclusion:
Patients were willing to be assessed for chemoprophylaxis after tick exposure by pharmacists, and pharmacist prescribing for this indication suggests increased access to post-tick exposure care.
Knowledge into Practice
This study is the first in Canada to describe experiences of pharmacist prescribing for Lyme disease chemoprophylaxis.
Following implementation of prescribing authority, pharmacists prescribed more than half (61.3%) of all prescriptions for prevention of Lyme disease after a tick bite in Nova Scotia.
Further research is needed on the impact on Lyme disease rates following pharmacist prescribing for Lyme disease chemoprophylaxis, the appropriateness of pharmacist prescribing, and its impact on the health care system.
Background
Lyme disease is a bacterial infection caused by Borrelia burgdorferi and transmitted to humans through bites from infected black-legged (deer) ticks (Ixodes scapularis) and western black-legged ticks (Ixodes pacificus). 1 Both species exhibit regional distribution within Canada. Black-legged ticks are predominantly found in southeastern and south-central Canada and western black-legged ticks in British Columbia. 2 Although the Lunenburg region in southern Nova Scotia (NS) was the first to be declared endemic for Lyme disease, more than 20 years ago, all areas in NS are now considered to be at higher risk.3,4
Early treatment of Lyme disease (most commonly presenting as erythema migrans) with antibiotics typically results in full recovery, but if left untreated or inadequately treated, high-risk tick bites 1 may progress to disseminated Lyme disease and can involve the joints, heart, and nervous system. These later stages of Lyme disease can appear months after the tick bite and may lead to significant morbidity. 5 Since the first reported cases of Lyme disease in NS in 2002, cases across the province have continued to increase. 6 To prevent Lyme disease, antibiotic prophylaxis (in adults) with a single 200 mg dose of oral doxycycline within 72 hours of tick removal following a high-risk tick bite has been demonstrated to be effective and is recommended by the Infectious Diseases Society of America, the Association of Medical Microbiology and Infectious Disease Canada, and the Nova Scotia Infectious Disease Expert Group.1,7 A systematic review and meta-analysis of prophylaxis after tick bites (all ages and risk levels) showed a significant reduction in risk of Lyme disease for individuals who received prophylaxis compared with placebo, with a number needed to treat of 49. The risk was further reduced in those where the tick was engorged with blood, with a number needed to treat of 11. 7 Both a watch-and-wait approach and antibiotic prophylaxis with doxycycline are viable options for children following a high-risk tick bite. 8 To be classified a high-risk tick bite, all 3 of the following criteria must be met: (1) the attached tick was an identified adult or nymphal black-legged (Ixodes spp.) tick, (2) the tick was attached for 36 hours or longer, generally based on the degree of engorgement or by certainty about the time of tick acquisition, and (3) the tick bite occurred in an endemic area, which includes the province of NS.
Mise En Pratique Des Connaissances
Cette étude est la première au Canada à décrire les expériences des pharmaciens qui prescrivent la chimioprophylaxie pour la maladie de Lyme.
Après la mise en œuvre du pouvoir de prescription, les pharmaciens ont prescrit plus de la moitié (61,3 %) de toutes les ordonnances pour la prévention de la maladie de Lyme après une morsure de tique en Nouvelle-Écosse.
D’autres recherches sont nécessaires concernant l’impact sur les taux de la maladie de Lyme suite à la prescription par les pharmaciens de la chimioprophylaxie contre la maladie de Lyme, la pertinence de la prescription des pharmaciens et son impact sur le système de soins de santé.
Historically, patients present to family physicians, walk-in clinics, or emergency departments (EDs) for antibiotic chemoprophylaxis following a high-risk tick bite. However, as of June 2023, more than 145,000 people (almost 15% of the population) were on a waitlist for a primary care provider in NS. Lack of access to a primary care provider, increased demand for walk-in clinics, and overcrowding in EDs 9 may result in decreased access to care. Strategies to reduce demand for these resources are needed.
Recognizing pharmacist expertise in medication management and in response to increasing demand on primary care providers and EDs, the Nova Scotia College of Pharmacists enabled pharmacists to prescribe Lyme disease chemoprophylaxis for asymptomatic adults and children on August 1, 2021. 10 After Alberta, where pharmacists can prescribe all Schedule 1 drugs under specific criteria, NS was the second province in Canada to authorize pharmacists to prescribe for this indication. 11 This was followed by enablement of pharmacist prescribing for Lyme disease chemoprophylaxis in Ontario and New Brunswick.12,13 Because pharmacists are accessible health care providers in the community, they are uniquely positioned to provide timely access to antibiotic prophylaxis for Lyme disease following tick exposure. This study aims to describe experiences related to pharmacist prescribing for Lyme disease chemoprophylaxis and reports on the rate of prescribing for Lyme chemoprophylaxis relative to other prescribers in NS.
Methods
Design
This was a retrospective cohort study using linked health administrative data. This study used a pre-and-post design to compare prescribing for Lyme disease chemoprophylaxis for 16 months before (from April 1, 2020 to July 31, 2021) and 16 months after (from August 1, 2021 to November 30, 2022) implementation of pharmacist prescribing for Lyme disease chemoprophylaxis. The selection of this study period ensured at least 1 full season when Lyme disease transmission was most likely to occur before and after implementation of the service. Black-legged ticks remain active until the temperature is consistently below 4°C, with transmission most frequent in the summer months. 14
Participants and dataset
Patients were included in this study if they were dispensed a single dose of oral doxycycline from a community pharmacy within NS during the study period, irrespective of the dose. We included both adults and children. The pediatric dose was 4.4 mg/kg/dose and not all pediatric patients would have received 200 mg; a single dose of doxycycline dispensed from a community pharmacy was included. The primary indication for a single dose of oral doxycycline was prevention of Lyme disease following a tick bite. Evidence has also emerged for use of single-dose doxycycline for prevention of sexually transmitted infections; however, this indication was not studied in large-scale, randomized controlled trials or widely accepted during our study period.15,16 Administrative health data were linked by Health Data Nova Scotia, a data repository based at Dalhousie University, which provided access to deidentified data. 17 Details from those individuals dispensed a single dose of doxycycline as identified from the Drug Information System (DIS) were extracted. The DIS is a comprehensive medication profile for any individual dispensed medication from a community pharmacy throughout the province of NS. 18 Characteristics of those receiving the doxycycline prescriptions were abstracted from the Insured Patient Registry, which catalogues demographic information such as sex and date of birth, Insured Health Benefits Program eligibility, and individual geography (i.e., county or postal code).
Data collection
Data collected from the DIS included date of single-dose doxycycline dispensation, county where doxycycline was dispensed, and prescriber type (pharmacist, physician, nurse practitioner, other). Demographic data collected from the Insured Patient Registry (MASTER) were linked to DIS data and included patient age and patient county. Population counts for each county in NS were gathered from the Economics and Statistics Division of Nova Scotia.19,20 Rate of single-dose doxycycline prescribing per 1000 individuals in each county was calculated and compared. Statistics Canada 2021 population data were used to calculate rates before pharmacist prescribing authorization for Lyme disease chemoprophylaxis as well as overall rates for the study period. Statistics Canada 2022 population data were used to calculate rates after pharmacist prescribing authorization for this indication.
Analysis
The number of dispensations for Lyme disease chemoprophylaxis was reported by month and patient county. Patient age was also examined. For age, reporting included descriptive statistics of frequency, mean, and standard deviation. For each prescriber type, frequency was reported overall as well as before and after pharmacist prescribing authorization for this indication (August 1, 2021). For each county in NS, the frequency of single-dose doxycycline prescriptions was reported monthly and considered with respect to whether it occurred before or after pharmacists received prescribing authority. Using population data, we calculated rates of single-dose doxycycline prescriptions per 1000 people for each county. This study was approved by the Nova Scotia Health Research Ethics Board (REB 1028677).
Results
Between April 1, 2020 and November 30, 2022, a total of 12,549 prescriptions for single-dose doxycycline were dispensed to 11,310 unique individuals in community pharmacies throughout NS. During the study period, 9.9% (n = 1239) of these unique individuals received 2 or more single doses of oral doxycycline. The overall mean age of individuals included was 51.8 ± 22.0 years. Further information on patient demographics is provided in Table 1.
Baseline demographics
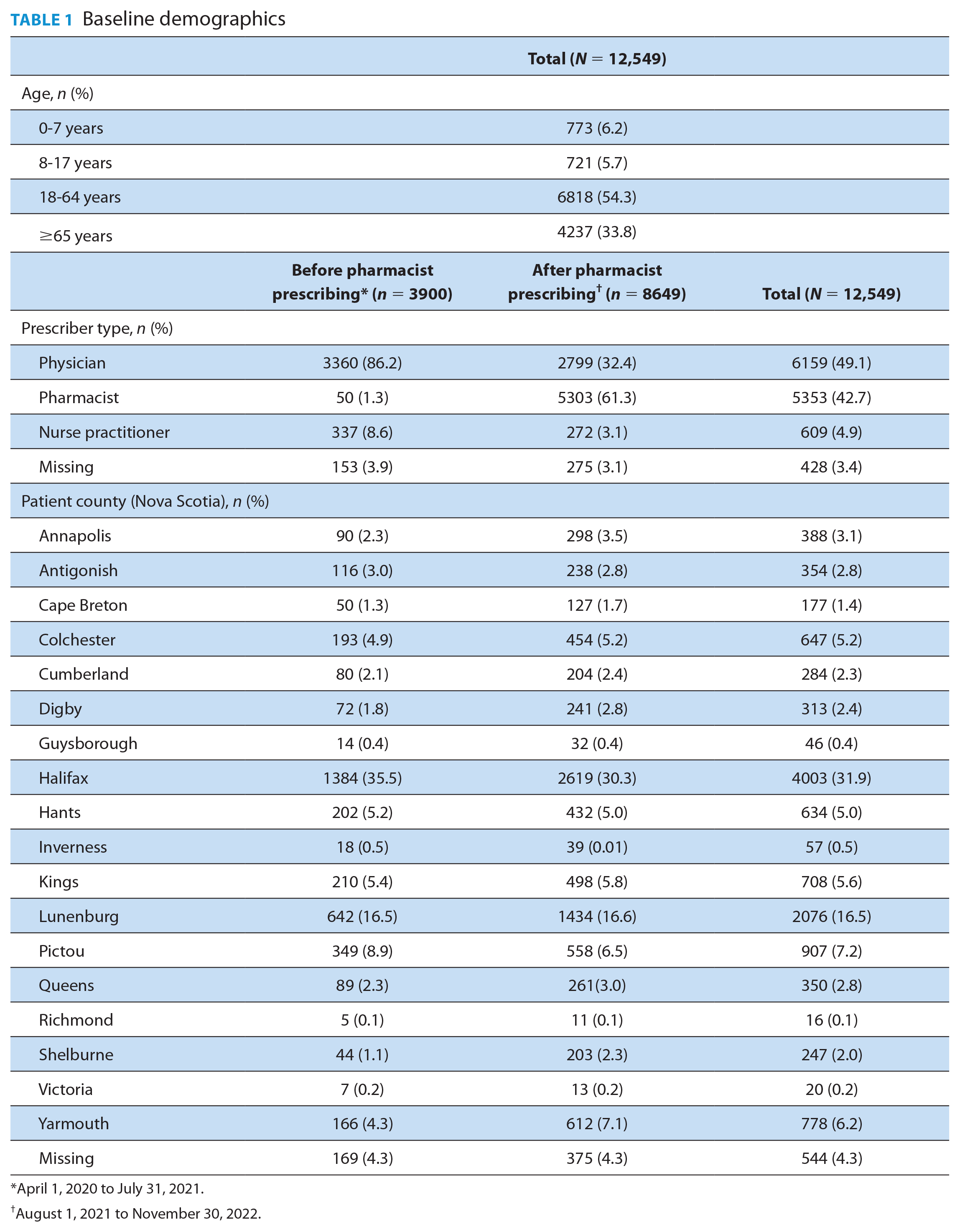
April 1, 2020 to July 31, 2021.
August 1, 2021 to November 30, 2022.
Doxycycline was dispensed from all 18 counties in NS. Although the counties with the highest numbers of single-dose doxycycline prescriptions were Halifax (n = 4003), Lunenburg (n = 2076), and Pictou (n = 907), when population size was taken into consideration, the counties with the highest rates of single-dose doxycycline prescriptions were Lunenburg (42/1000), Queens (34/1000), and Yarmouth (31/1000) in southern NS (Table 1).
In the 16 months before pharmacist prescribing authorization (April 1, 2020 to July 31, 2021), 3900 single-dose doxycycline prescriptions were dispensed. Following pharmacist prescribing authorization (August 1, 2021 to November 30, 2022), 8649 single-dose doxycycline prescriptions were dispensed.
Before pharmacist prescribing was authorized, May and June had the highest number of single-dose doxycycline prescriptions dispensed. After pharmacist prescribing authorization, the highest rates of dispensations for a single-dose doxycycline prescription occurred in June, October, and November (Figure 1), suggesting the greatest tick exposure in spring and fall.
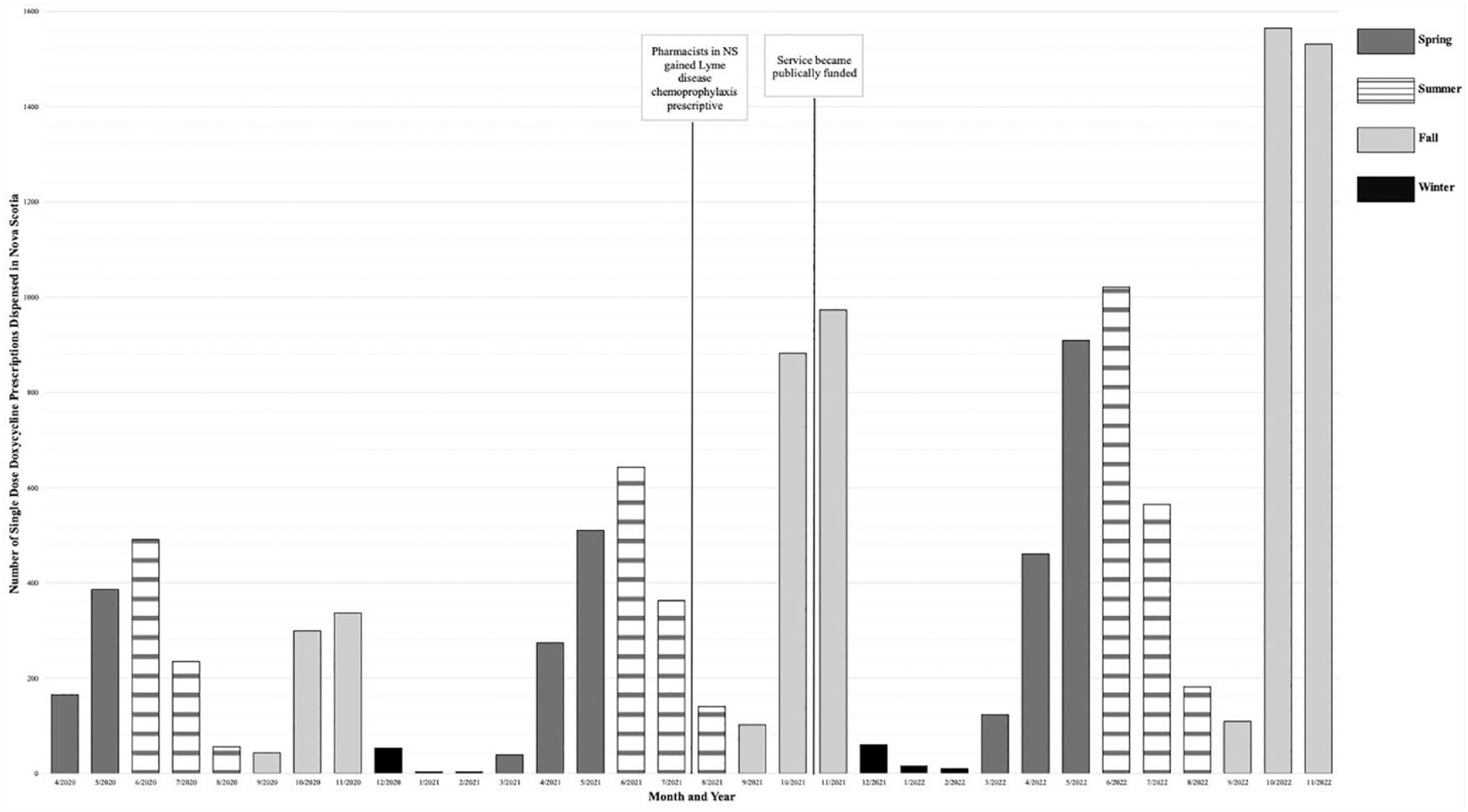
Number of single-dose doxycycline prescriptions dispensed in Nova Scotia (April 2020 to November 2022)
Prescribers predominantly included physicians, nurse practitioners, and pharmacists. During the study period, 49.1% (n = 6159) of single-dose doxycycline prescriptions dispensed were written by physicians, 4.9% (n = 609) were written by nurse practitioners, and 42.7% (n = 5353) were written by pharmacists. Prescriber type could not be identified through administrative data in a small proportion of prescribers (3.4%) during the study period. Before pharmacists in NS had the authority to prescribe for this indication, physicians wrote 86.2% of single-dose doxycycline prescriptions. Pharmacists were identified as prescribers in 1.3% of single-dose doxycycline dispensations, likely as a result of collaborative practice agreements. In the 16 months following August 1, 2021, prescribing of single-dose doxycycline by physicians decreased to 32.4% of all prescriptions dispensed, with pharmacists prescribing 61.3% of all single-dose doxycycline prescriptions dispensed in NS.
Discussion
This study is the first in Canada to describe community pharmacist prescribing of single-dose doxycycline to prevent Lyme disease following a tick bite. Retrospective data from this study demonstrated an overall increase in the number of single-dose doxycycline prescriptions dispensed in NS, with the number more than doubling in the 16 months after pharmacists began prescribing for this indication. Following the implementation of prescribing authority, pharmacists became the most frequent prescribers of single-dose doxycycline. Prescriptions by physicians remained stable despite increased dispensation. This suggests that the expanded scope of pharmacists to prescribe for this indication may have led to a decreased burden on other areas of the health care system.
Since Lyme disease became a nationally notifiable disease in Canada in 2009, the number of confirmed human cases of Lyme disease in Canada has steadily risen (from 144 in 2009 to 3147 in 2021). 21 This will inevitably continue to increase with the expansion of ticks across Canada. Evidence suggests this is attributed to multiple factors, with a warming climate being a primary contributor allowing for continued expansion of the tick population in Canada. 22 As 1 example, it is estimated that ticks are expanding their range in Quebec by 18 km per year and that by 2027, 90% of Quebec’s population will live in a tick-endemic area. 23 Warmer temperatures also allow ticks to be active longer during the year while also permitting humans to engage in more outdoor activities, increasing the probability of humans encountering ticks.24,25 Lyme disease in humans and geographical areas of risk are monitored by Health Canada; however, data on the tick population are not reported. 21 One strategy for surveillance of the tick population in Canada is through eTick, a Canadian image-based identification and population monitoring platform created in 2014. Data from eTick provide further support that more individuals are encountering ticks across Canada. When considering both black-legged (deer) ticks (Ixodes scapularis) and western black-legged ticks (Ixodes pacificus), 2419 ticks were identified on humans through this platform between April 1, 2020 and July 31, 2021. Of these, 332 were reported in NS. In the 16 months following authorization of pharmacist prescribing of Lyme chemoprophylaxis, from August 1, 2021 to November 30, 2022, a total of 3193 ticks were identified on humans nationally, with 514 of these being reported in NS. 26 These data suggest the possibility that more individuals recognized tick bites during this time. Increased tick exposure is likely contributing to the increased number of single-dose doxycycline prescriptions. Due to the voluntary reporting on this platform, it is difficult to conclude that these numbers are representative of tick bites in the general population.
Another explanation for the increase in prescribing for high-risk tick bites is ease of access to prescribing. Although the total number of doxycycline prescriptions by physicians was similar before and after implementation of expanded scope, the proportion of physician prescriptions declined. This may be a result of easier access to the service for patients without a primary care provider or in regions with less access to EDs or walk-in clinics. Pharmacists are among the most accessible health care professionals in NS, with expertise in pharmacotherapy. Individuals who may not have previously sought out post-tick exposure care due to accessibility challenges may have been more likely to access care in a community pharmacy setting. We predict a continued growing need for access to post-tick exposure chemoprophylaxis across Canada. It is also important to consider that public funding of pharmacist prescribing for this indication likely contributed to high uptake. If public funding is not provided in other jurisdictions, data may not be generalizable. It is likely that fewer patients would access care from pharmacies if they were required to pay out-of-pocket.
Limited published literature is available on experiences related to pharmacist prescribing for Lyme disease chemoprophylaxis internationally. One small study through a pharmacy-run clinic in the United States reported improved appropriateness of doxycycline prescribing and decreased primary care visits following a tick bite when patients accessed a pharmacist for post-tick exposure care. 27 Another study in the United States evaluated pharmacist Lyme disease chemoprophylaxis prescribing at a single community pharmacy under a collaborative practice agreement. Although patient satisfaction was high, only 8 patients participated in this study. No patients in the study developed symptoms of Lyme disease. 28 Additional studies are needed that evaluate pharmacist prescribing for this indication in community pharmacy settings and in a Canadian context. Future research should evaluate how pharmacist post-tick exposure care is affecting Lyme disease infection rates, patient satisfaction, and use of other sectors of the health care system. Appropriateness of single-dose doxycycline dispensed to prevent Lyme disease should also be evaluated.
There are several limitations of this study to consider. Aside from an increasing tick population, other factors may have contributed to the increase in single-dose doxycycline prescriptions observed. Radio, television, and social media reported on pharmacists being able to assess tick bites in NS, with most media coverage coming around the time it became publicly funded (October 29, 2021). Some individuals may have been unaware that tick bites should be assessed by a health care professional prior to learning about this service in the media, which may have driven health care-seeking behaviour. Although this media attention may have increased awareness, we did not see a similar increase in the number of patients seeking care for tick bites from other prescribers. An increase in single-dose doxycycline dispensations may have also resulted from an increase in the tick population in NS, which may have skewed results. This study also relied on accurate documentation by health care professionals. We were not able to evaluate appropriateness of prescribing or patient outcomes following assessment for tick bites due to lack of access to this data. In addition, we did not have access to data on patients who were assessed for Lyme disease chemoprophylaxis in a pharmacy who did not receive a single-dose doxycycline prescription. Since an assessment that determined no need for prophylaxis is arguably of similar value to an assessment that led to a prescription, our findings likely underestimate the total impact of pharmacist prescribing for this service. Our study period also occurred during the COVID-19 pandemic, which resulted in reduced access to health care resources throughout Canada. In addition, public health restrictions limited indoor social gatherings and more Canadians may have turned to outdoor activities during these periods. It is possible that the pandemic affected Lyme disease chemoprophylaxis prescribing patterns. A final limitation to consider is the possibility that single-dose doxycycline may be dispensed for other off-label indications. Despite emerging evidence supporting the use of single-dose doxycycline to prevent sexually transmitted infections, we anticipate minimal impact because large-scale, randomized controlled trials were not published until after the study period ended.15,16 Furthermore, pharmacists in NS cannot prescribe for this indication so this evidence would not affect data on pharmacist prescribing of doxycycline.
Conclusion
This study provides important insight into the impact of pharmacist-prescribed Lyme disease chemoprophylaxis in NS. Pharmacists have become the primary source of consultation for Lyme chemoprophylaxis. Increased accessibility of this service is associated with an increased number of single-dose doxycycline prescriptions. This study demonstrates that patients are willing to receive care from pharmacists for tick bites, and it serves as an example of how pharmacists may be better positioned within primary care to address the health needs of a population.
Footnotes
Author Contributions:
T. Ramsey, T. Hatchette, S. Campbell, A. Bishop, and E. Black conceptualized the study; E. Black acquired the funding and provided data access; T. Ramsey, S. Trenaman, T. Hatchette, S. Campbell, A. Bishop, M. MacInnis, K. Hurley, and E. Black developed the method; M. Bell and S. Trenaman analyzed the data; T. Ramsey, S. Trenaman, T. Hatchette, S. Campbell, A. Bishop, M. MacInnis, K. Hurley, and E. Black interpreted the results; M. Bell and E. Black wrote the original manuscript; T. Ramsey, S. Trenaman, T. Hatchette, S. Campbell, A. Bishop, M. MacInnis, and K. Hurley reviewed and edited the manuscript; all authors approved the final version of this manuscript.
Declaration of Conflicting Interests:
Since completing this project, Dr. Emily Black has received funding from Shoppers Drug Mart to explore pharmacist prescribing for infectious diseases and from Pfizer Canada for unrelated work on immunizations. Other authors have no financial or personal relationships with commercial entities to disclose.
Disclaimer:
The data used in this report were made available by Health Data Nova Scotia of Dalhousie University. Although this research analysis is based on data obtained from the Nova Scotia Department of Health and Wellness, the observations and opinions expressed are those of the authors and do not represent those of either Health Data Nova Scotia or the Department of Health and Wellness.
Funding:
This project received grant support from the Dalhousie Pharmacy Endowment Fund and the Drug Evaluation Alliance of Nova Scotia.