
Abstract
Background:
Undervaccination is a public health issue that disproportionately affects underserved populations. Pharmacists are accessible health care professionals who have the potential to better reach communities. The aim of this study is to understand how organizational obstacles influence the pharmacist’s ability to meet underserved clients’ vaccination needs in community pharmacy.
Methods:
We conducted semi-structured interviews with key stakeholders in Quebec. Results were codified according to domains of the Consolidated Framework for Implementation Research.
Results:
Fourteen interviews were carried out with representatives from pharmacy associations, pharmacy chains and banners, integrated health and social service centres, and local Quebec Public Health departments. Barriers to promoting vaccination were identified in four areas: 1) vaccine service logistics, 2) the pharmacy setting, 3) external influences and 4) pharmacist’s knowledge and beliefs.
Discussion:
Technological tools accessible to pharmacists are sufficient but not user-friendly due to the lack of integration between the pharmacy software, the vaccine registry and the provincial appointment system. Technology limits access to vaccination for certain underserved populations. Moreover, the incentives linked to vaccination do not favour the vaccination of difficult-to-reach clients and they limit pharmacists’ ability to be proactive with vaccine recommendations. Pharmacists are more inclined to participate in mass vaccination campaigns, and delegating vaccine administration to nurses and technicians allows pharmacies to financially break even. Certain services such as travel health vaccination require an extended set of knowledge, which creates resistance for some pharmacists to integrate the role.
Conclusion:
Pharmacists are well-placed to improve vaccination uptake, but several technological and organizational barriers limit their ability to provide vaccination services and reach underserved communities. A better alignment between incentives and proactive promotion should be put forward to encourage pharmacists to actively identify and reach underserved populations.
Knowledge into Practice
Pharmacists are key contributors to vaccination and have become the dominant providers of influenza vaccines in Canada.
Technological and organizational barriers limit the efficiency, proactivity and motivation to identify vaccine needs of underserved patients.
Proactivity is also discouraged by the lack of timely access to vaccine-related information and integration with existing tools.
Incentives should be better aligned to encourage a broader set of activities related to vaccination, such as updating vaccine status, identifying vaccine gaps, improving education and motivational interviewing with vaccine-hesitant patients.
Background
Death associated with vaccine-preventable diseases remains 1 of the 10 most prevalent causes of mortality in Canada, responsible for approximately 7000 deaths annually. 1 Year after year, provinces fail to meet the established 95% vaccination rate for infants younger than 2 years of age or the 80% target for influenza and pneumonia for at-risk adults. 2 The COVID-19 pandemic revealed vaccine gaps that disproportionately affected individuals with low education, a poor perception of their own health or lack of regular access to a primary care physician. 3 These gaps revealed excess mortality in individuals living in low socioeconomic and ethnocultural neighbourhoods. 4 New challenges such as patient and health care provider vaccine fatigue, misinformation and the polarization of opinions are on the rise, which makes vaccine hesitancy 1 of the 10 threats to world health, according to the World Health Organization. 5
Pharmacists have demonstrated that they can be part of the solution to improve vaccination coverage. 6 In Canada, a 2017 study demonstrated that allowing pharmacists to vaccinate increased influenza coverage by 6% through improved service accessibility. 7 Since then, pharmacists have become the dominant vaccine providers as they have replaced physician offices as the most prevalent location in which to receive the influenza vaccine. 8 Quebec recently became 1 of the last provinces to allow pharmacists to prescribe and administer vaccines. 9 The COVID-19 pandemic accelerated the expansion of the scope of practice, allowing Quebec pharmacists to prescribe and administer all vaccines for those 6 years of age and older, travel health vaccines for those 2 years and older and influenza or COVID vaccines to patients of all ages.9,10
Integrating vaccination within Quebec pharmacies presents opportunities and challenges. Pharmacists are known as accessible, trustworthy and cost-effective providers.11 -13 In recent years, Quebec pharmacists have added various clinical responsibilities to their dispensing activities, such as prescribing for common conditions, adjusting chronic condition medications and prescribing laboratory tests. 14 Vaccination services must be integrated into existing and continuing-to-expand pharmacy services. Pharmacists control the services they provide but also must consider the business consequences. With vaccination services, pharmacists also connect with the existing network of Public Health, governmental entities and vaccination health care professionals to build synergies and reach underserved communities. 15
Mise En Pratique Des Connaissances
Les pharmaciens sont des contributeurs clés à la vaccination et sont devenus les principaux fournisseurs de vaccins antigrippaux au Canada.
Les obstacles technologiques et organisationnels limitent l’efficacité, la proactivité et la motivation à identifier les besoins en vaccins des patients mal desservis.
La proactivité est également découragée par le manque d’accès en temps utile aux informations relatives aux vaccins et par l’absence d’intégration avec les outils existants.
Les mesures incitatives devraient être mieux harmonisées afin d’encourager un ensemble plus large d’activités liées à la vaccination, comme la mise à jour du statut vaccinal, l’identification des lacunes en matière de vaccins, l’amélioration de l’éducation et des entretiens de motivation avec les patients qui hésitent à se faire vacciner.
Our objective is to understand how organizational obstacles influence the community pharmacist’s ability to meet underserved patients’ vaccination needs in the community pharmacy. Although our study centres on pharmacists, we have included stakeholder statements about pharmacy technicians and nurses in pharmacies, as they are key collaborators in vaccination services. We chose to include diversified perspectives from pharmacy representatives, health services and Public Health to gain a broader view of vaccination practices in community pharmacies. Exploring the barriers and facilitators to vaccination will promote further discussion about tools and support the need for pharmacists to better meet vaccine equity and coverage goals.
Methods
We performed a qualitative study with key vaccination stakeholders, with representation from the 5 following groups: 1) pharmacy associations, 2) pharmacy chains and banners, 3) integrated health and social service centres (IHSSC), 4) local Quebec Public Health departments and 5) the Ministry of Health. We collaborated with the Quebec Pharmacy Owners Association to identify and reach the most pertinent individuals from each group. Participants were recruited through purposive sampling based on diversity of viewpoints until no unique knowledge was obtained from new interviews. An initial sample size of 3 per group was estimated and thematic data saturation was reached once no new additional second-level themes were revealed. 16 We also recruited through snowball sampling by asking all participants to suggest any other relevant participants in the vaccination process. To ensure the validity of the findings, we followed the COnsolidated criteria for REporting Qualitative research (COREQ) checklist (Appendix 1, available online in Supplementary Materials). 17 Ethics approval was obtained by the University of Montreal Research Ethics Board (CERC-2021-1357). The results of this study were used for 2 separate research papers, with this paper focusing on the organizational aspects of community pharmacy vaccination, and the other analyzing the collaboration between pharmacists and the public sector.
Data were collected through semistructured interviews during the period from March 15 to June 7, 2022, via Microsoft Teams or Zoom platforms. Participants were initially contacted through email or by phone, and 3 reminders were sent in the absence of a response. The interview started with a short introduction to the interviewer, a community pharmacist and Master’s student with extensive vaccination experience. We reminded participants of the study objective and asked demographic survey questions. Participants were asked how they defined underserved populations in regard to vaccination. The interview was then separated into 3 topics: mass vaccination campaigns, routine vaccination initiatives (vaccinations occurring all year long during daily operation with or without an appointment) and collaborations within the health care system. Field notes were taken after each interview to document contextual details and nonverbal expressions.
Each interview was recorded, transcribed and anonymized. The main author segmented each interview into broad categories: underserved population characteristics, organizational factors, incentives, legal barriers and role in vaccination. Quotes were then classified according to 4 domains of the Consolidated Framework for Implementation Research in Pharmacy (CFIR) (Table 1) and themes. 18 Although some statements could belong in more than 1 category, we chose to include them in only 1 domain for the sake of simplicity. Discussions between the coauthors confirmed the data classification. Finally, the results were summarized by the main author and reviewed by the rest of the team.
Description of consolidated framework for implementation research in pharmacy domains

Results
We conducted 14 interviews with participants from 4 of the 5 identified stakeholder groups. The demographic characteristics of participants can be found in Table 2. Despite our efforts to reach Health Ministry representatives, 3 of the recommended stakeholders did not reply to us and 1 declined to take part. Interviews lasted from 37 to 65 minutes. Relevant quotes are presented according to the 4 CFIR domains in Table 3.
Characteristics of participants

Participants were asked to self-report their work context based on size and population density. 19
Representative quotes selected according to CFIR domains
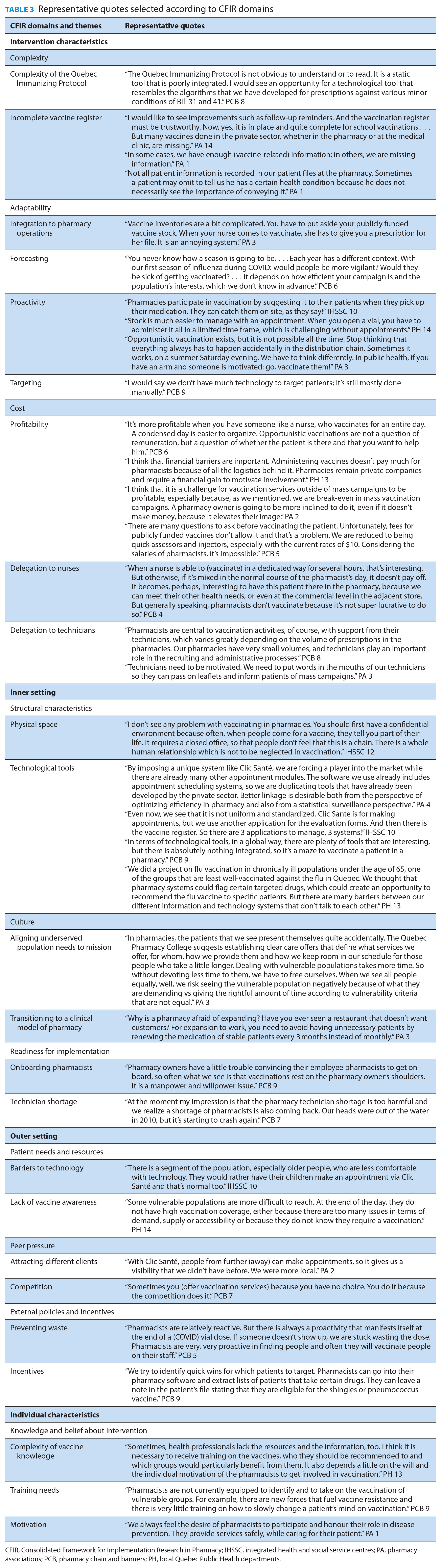
CFIR, Consolidated Framework for Implementation Research in Pharmacy; IHSSC, integrated health and social service centres; PA, pharmacy associations; PCB, pharmacy chain and banners; PH, local Quebec Public Health departments.
Intervention characteristics
Complexity
The discussion around vaccine service organizations centred on the complexity of their activity, adaptability and costs. Participants indicated that the tools that aid pharmacists in their vaccination activities provided sufficient information and fluidity to aid their vaccination activities. They suggested that although the Quebec Immunizing Protocol is a thorough guideline, it should be more user-friendly. Many also complained that the vaccine registry was incomplete. Assessing a patient’s eligibility for a vaccine is complex and pharmacists must deduce the patient’s illness based on his or her medication or rely on self-report. This may omit valuable information since the patient’s medical file is not shared between physicians and pharmacists. Public Health representatives suggested adding pop-ups to simplify the profile analysis.
Adaptability
Adapting vaccination activities to the pharmacy workflow was a challenge. Private and publicly funded vaccines both had different procedures and required keeping separate inventories of products that were sometimes identical. Chains and banner representatives reported that forecasting is a difficult and inflexible process during mass campaigns. Pharmacy owners had to predict how many private and publicly funded vaccines they wished to order many months prior to the vaccination season. Pharmacists complained that the eligibility criteria for publicly funded vaccines were not even made public when making the order. This affected pharmacists’ ability to plan ahead. The appointment-based model was widely used in pharmacies to better predict workload and resource use. Public Health representatives believed that pharmacists should promote vaccination whenever an opportunity presents itself. Although pharmacists are well-placed to identify patients, all interview participants agreed that pharmacists are mostly reactive to the client’s demands and display little proactivity in their recruitment.
Cost
Pharmacists were also concerned with cost and reimbursement for vaccine activities. On one hand, participants indicated that mass campaign vaccinations broke even with pharmacists as vaccinators. Many pharmacies chose to delegate vaccination activities to nurses as it was easier to dedicate 1 person to vaccines for an entire day. On the other hand, opportunistic vaccination was described as not cost-effective, although some pharmacists still chose to offer the service. Technicians were mentioned many times as key players in vaccination. They helped spread the word to patients, booked appointments, facilitated vaccine operations and assisted in the administrative paperwork.
Inner setting
Structural characteristics
The interview participants focused on structural characteristics of pharmacies, culture and readiness for implementation. Participants described pharmacies as well-designed to offer a confidential and professional environment. Many tool-related comments centred around the new provincial booking system called Clic Santé. Participants discussed the benefits of having a standardized appointment platform, such as a convenient experience for patients and public health surveillance. However, this platform duplicates existing platforms developed by the private sector and is not integrated with other systems. Some reported that more could have been done to optimize efficiency and avoid data entry repetition.
Culture
Pharmacy representatives reported that underserved populations are not the focus in vaccine promotion and a culture change must be made to better cater to them. Reimbursement does not compensate for the amount of time required to engage effectively with vaccine-hesitant patients, who are more likely to be in underserved groups. Pharmacy association participants suggested that incentives should better reflect the conception that all patients do not require the same amount of time. Most participants acknowledged that pharmacies are undergoing a transition to a more clinical model of care. It was proposed that in order to take advantage of vaccination opportunities, pharmacies must make their dispensing activities more efficient and must free up some time for value-added activities such as vaccination. Participants cited the example of renewing medication every 3 months for stable patients to save time.
Readiness for implementation
Participants reported different views on the readiness to implement vaccination services. Although many pharmacists received their vaccination training in Quebec, pharmacy chains and banners mentioned that pharmacy owners struggled to onboard their employee pharmacists. As pharmacies have a busy workload, many owners personally took on the leadership of implementing vaccine services. Technician and pharmacist shortages were also a barrier, as it is difficult to implement changes with new employees.
Outer setting
Patient need and resources
During the interviews, it was mentioned that vaccine services were influenced by patient needs, competition between pharmacies, vaccine policies and incentives. Although vaccination services were easy to promote, some clients were not aware they should receive a vaccine. Patients younger than 65 with chronic conditions were cited by Public Health representatives as 1 of the most undervaccinated groups at risk for influenza and pneumococcal infection. The use of technology was reported as a great way to promote one’s services, is appreciated by younger clients and could attract new clients. Nevertheless, online bookings could create barriers for others, such as elderly and immigrant populations. Individuals with low technological literacy needed support from their children or a friend to make an appointment. Patients wanted an accessible and simple vaccination experience.
Peer pressure
As vaccination services became more prevalent in pharmacies, competition was mentioned as a motive for pharmacy owners to vaccinate during mass campaigns. It was mentioned by chain and banner representatives that sometimes a pharmacy only chose to vaccinate in order to offer similar services as their competitor.
External policies and incentives
Pharmacy associations, chains and banners underlined the important influence of incentives on vaccination services. Since pharmacists are compensated through a fee-for-service model, the system encourages them to find quick wins. Pharmacists listed some targeting strategies, such as extracting lists of patients with specific medical conditions or targeting through existing programs (e.g., blister pack patients, chronic follow-up programs). As some vaccines have short stability once opened, pharmacists displayed creativity to recruit patients rather than wasting a dose when a cancellation occurs. This can be explained by the fact that publicly funded vaccines were free for the patient, but pharmacists were only reimbursed for the wholesaler fee if the vaccine was administered. Some pharmacists were also discouraged from participating in routine vaccinations because of the obligation to book an appointment prior to ordering the vaccine, and some multidosed publicly available vaccines. For example, to administer a human papillomavirus vaccine to a teen who missed their vaccine at school, a pharmacist had to book 10 appointments that meet the eligibility criteria before ordering the vaccine as it was only available in a 10-dose multidose vial.
Individual characteristics
Knowledge and belief about intervention
Interview participants commented on a pharmacist’s need for training, the knowledge required about vaccines and the motivation behind successful vaccine operations. Although pharmacists are required to receive training on basic vaccine administration techniques, cardiopulmonary resuscitation and vaccine register entries, the mandatory training was often described as insufficient. Pharmacists had little training on travel health vaccination, catch-up schedules and vaccination of immunocompromised patients. Some participants complained that pharmacists lacked the tools and communication training to address vaccine-hesitant patients. Vaccine eligibility criteria are also complex and require an intricate knowledge of infectious disease risks. The vaccine literature is also constantly evolving, especially during the COVID period. These obstacles explain why pharmacists needed strong individual motivation to stay up-to-date on vaccine development, while also keeping current on their regular therapeutic continuing education.
Discussion
Pharmacists are now important vaccinators; however, the workflow and organizational barriers must be addressed in order to maintain and/or grow that role. Our results allowed us to gather perspectives from a broad range of stakeholders that have a strong comprehension of the pharmacy context. It revealed a strong motivation for pharmacists to contribute to vaccination efforts despite organizational barriers. These obstacles appear to limit their efficiency, proactivity and motivation to identify underserved patients.
Organization of vaccination services and technology
According to most participants, inefficient technology tools and the lack of access to vaccination data are frustrations for pharmacists. The vaccine register was cited as not user-friendly as it does not pair with other software used in pharmacies. Having access to the vaccine registry is the first step to obtaining timely vaccine information, as only 12 of the 33 countries where pharmacy-based vaccination is permitted have access to all vaccine records. 20 Although many improvements are proposed by the participants, coordinating a single system with the different software programs used by health care professionals is a huge challenge. Knowing a patient’s vaccine history is essential to properly evaluating a patient’s vaccine needs, as access to the medical file is also lacking for pharmacists. Participants are asking for the registry to analyze missing and recommended vaccines in a simple and efficient visual aid. Similar technological needs are mentioned in the literature, such as app-based support and an increased use of telemedicine in vaccination consultations. 21
Technological difficulties add on to other frequently mentioned obstacles to vaccine implementation in pharmacies, such as the lack of time and competing priorities.22-24 The provincial appointment platform is a great tool to save time with data entry and booking appointments. Participants observed that the use of technology provides publicity and optimizes appointment schedules but may not serve all clients, including those with low technological access or ability.
Aligning incentives to action
According to our interviews, pharmacists are more inclined to participate in mass vaccination campaigns than to provide routine vaccinations, predominantly for economic reasons. Participants described the remuneration fees between $9 and $11 per vaccination as break-even only when there is a possibility to dedicate a vaccinator for an extended period of time. Remuneration fees are heterogeneous across Canada, the United States and Great Britain. 25 Sufficient reimbursement is a predictor of a pharmacist’s willingness to get involved in vaccination. 26 A cost-utility analysis in the context of Ontario suggests that a $15 consultation fee in favour of influenza vaccination is hypothesized to be cost-effective and to improve uptake in seniors. 27 Improved compensation for both administration and advocating for vaccination will therefore encourage proactivity, vaccine confidence and coverage.
In both our results and the literature, pharmacists were described predominantly as reactive vaccinators. 28 Pharmacists are well-placed and capable of using a variety of promotional methods to effectively encourage vaccination to their patients. As accessible and trusted health care professionals, a strong recommendation from a pharmacist is known as one of the most efficient strategies to promote vaccination. 29 Examples of proactivity were cited in the interviews, such as generating a list of vulnerable patients according to their medication, leaving bag stuffers when they pick up their medications and promoting vaccines at the right moment (i.e., offering the pertussis vaccine to pregnant women when dispensing prenatal vitamins). 30
Tailoring pharmaceutical services to underserved communities: A necessity for vaccine efficacy and equity
The pharmacy is undergoing a transition from a predominantly dispensing-driven model to a clinical model of care. 31 Pharmacies seek to reorganize their operations to increase predictability and free up time for value-added activities such as vaccinations. Vaccination services are not limited to the act of vaccinating patients but also consist of offering vaccination to underserved populations. Targeted approaches consist of applying priority to a subgroup within a broader defined population. 32 Pharmacy technicians are key contributors to vaccination as they can initiate conversations with eligible patients, administer vaccines in some provinces and help in documentation activities. 33 The decision to get vaccinated, particularly for vaccine-hesitant patients, can be tentative, and pharmacists must seize the opportunity when it arises. We believe that health care professionals have the responsibility to adapt the care they provide according to need. We must not seek to provide equal care to all but rather to provide equitable care, thus allowing more time for underserved clients.
Pharmacists should be granted opportunities similar to medication reviews to identify missing vaccinations and establish a vaccine schedule plan. All Canadian provinces except Quebec and Manitoba reimburse this activity for selected clients. 34 Little focus is presently put on targeting eligible patients in Quebec since no incentives are attached to validating the vaccine status, educating patients on their needs and promoting vaccination. We, however, advocate for a separate structure as medication reviews and vaccination reviews require distinct data collection and training. We hope that seizing opportunities during routine pharmacist activities will improve the convenience and timing of their recommendations, 2 of the most impactful determinants of vaccination for patients. 35 Training also goes beyond knowledge. Through assertive and culturally relevant communication, pharmacists may better personalize their vaccine conversations according to health status, geography and cultural determinants.36,37
Limitations
We interviewed representatives of associations and groups whose opinions may not correspond to the views of all pharmacists or vaccination stakeholders. Our interviews were conducted during eventful times for pharmacists, from March to June 2022. The provincial COVID vaccination campaign remained important in the media and pharmacists had just acquired the rights to prescribe antivirals against COVID and dispense publicly funded vaccines. We believe these changes may have brought a more positive outlook to clinical activities.
Conclusion
Our study highlights many barriers to implementing equitable vaccination services in Quebec. These obstacles appear to limit the efficiency, proactivity and motivation of pharmacists to identify underserved patients. Incentives should be better aligned to a broad set of activities related to vaccination, such as updating the vaccine status, identifying vaccine gaps and improving education. Proactivity and important vaccination uptake tools tend to be discouraged because of the lack of timely access to vaccine-related information and integration with existing tools. Although technology is usually time-saving, it may limit the accessibility of vaccination to patients with low technology literacy.
As pharmacists are accessible health care professionals, a reflection on vaccine policies and incentives is necessary to promote vaccine equity and optimize logistics within the pharmacy. ■
Supplemental Material
sj-pdf-1-cph-10.1177_17151635241269988 – Supplemental material for Key stakeholder perspectives on delivery of vaccination services in Quebec community pharmacies
Supplemental material, sj-pdf-1-cph-10.1177_17151635241269988 for Key stakeholder perspectives on delivery of vaccination services in Quebec community pharmacies by Alexandre Chadi, Daniel J. G. Thirion, Nancy M. Waite and Pierre-Marie David in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Acknowledgements
We would like to thank Pierre-Marc Gervais from the Quebec Pharmacy Owners Association for his contribution and contacts.
Author Contributions:
Research protocol, questionnaires and analysis grid were designed by A. Chadi, D. J. G. Thiron and P.-M. David. A. Chadi recruited the participants, performed the interviews, transcribed and codified the findings. Classification was confirmed through discussions among all coauthors. The manuscript was written by the main author (A. Chadi) and reviewed by the rest of the team (P.-M. David, D. J. G. Thirion, N. M. Waite).
Declaration of Conflicting Interests:
The authors have no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding:
This work was supported by the Sanofi Chair in ambulatory pharmaceutical care of University of Montreal and a grant by Pfizer without rights of scrutiny, propelled by MITACS. The funding organizations had no input into the study.
Supplemental Material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.