
Abstract
Background:
Community pharmacies typically require patients to request medication refills. The appointment-based model (ABM) is a proactive approach that synchronizes refills and schedules patient–pharmacist appointments. These appointments provide opportunities for medication reviews, medication optimization and health promotion services. The primary aim of this study was to describe the types of patients who received an ABM service in a community pharmacy in Ontario in 2017. The secondary aim was to describe reimbursable clinical service uptake.
Methods:
In September 2017, the ABM was implemented across 3 Ontario community pharmacies within a Canadian pharmacy banner. Patients who filled at least 1 chronic oral medication and consented to enrolment were eligible. In December 2018, data were extracted from pharmacies using pharmacy management software. Descriptive statistics and frequencies were generated.
Results:
Analysis of 131 patients (51.1% female; mean ± SD age 70.8 ± 10.5 years) revealed patients were dispensed a mean ± SD of 5.1 ± 2.7 medications, and 73 (55.7%) experienced polypharmacy. Hypertension (87.8%) and dyslipidemia (68.7%) were the most common medical conditions. There were 74 (56.5%) patients who received ≥1 medication review service (MedsCheck). Of 79 unique drug therapy problems (DTPs) identified, the most common categories related to patients needing additional drug therapy and adverse drug reactions.
Discussion and conclusion:
Patients enrolled in the ABM were generally older adults experiencing polypharmacy. The ABM presented opportunities for DTP identification and delivery of reimbursed services. Findings support continued exploration of the ABM to support integration of clinical services within community practice.
Knowledge into Practice
The appointment-based model (ABM) in community pharmacy practice is associated with increased medication adherence and refills, detection of drug therapy problems and clinical service uptake.
Our study describes the demographics of patients enrolled in the ABM in a sample of Ontario-based community pharmacies and the reimbursable clinical services they received.
This study may be helpful for pharmacists implementing the ABM by supporting opportunities for the provision of clinical services and tailoring care according to patient need.
Introduction
Two-thirds of adults aged 74 years and older experience multimorbidity. 1 Multimorbidity, also known as 2 or more chronic medical conditions occurring in the same person, 2 often requires the concurrent use of several medications and an increased likelihood of polypharmacy (taking 5 or more medications). 3 Polypharmacy is linked to taking an inappropriately prescribed medication. 4 Pharmacists are ideally suited to manage these problems through deprescribing, improving medication adherence and optimizing chronic condition management and outcomes in older patients.5-7 The ability for pharmacists to provide these services within the community pharmacy setting, however, is impacted by capacity and resourcing, which is influenced by the time allotted to other community pharmacy responsibilities such as dispensing medications.7,8
Most community pharmacies expect patients to request their own medication refills, which is not ideal for pharmacist planning of proactive comprehensive clinical services for patients. 9 Patients typically request individual prescription refills on an unaligned schedule. This can result in patients running out of their medication, which contributes to nonadherence; this also forces patients to make multiple trips to the pharmacy to pick up medications. 10 For pharmacists, this can lead to interrupted and inefficient workflows, with pharmacies running out of medication stock and pharmacists having to contact the same prescriber multiple times for refills or therapeutic adjustments for the same patient. 10 Inefficient workflows, which contribute to reduced productivity, reduce time that pharmacists can spend providing clinical services in community pharmacies across the world.11-14 Lack of time is a top barrier to community pharmacist involvement in health promotion activities. 15
Mise En Pratique Des Connaissances
Le modèle sur rendez-vous (MRV) dans la pratique de la pharmacie communautaire est associé à une augmentation de l’observance thérapeutique et du renouvellement d’ordonnances, de la détection des problèmes de pharmacothérapie et de l’utilisation des services cliniques.
Notre étude décrit les caractéristiques démographiques des patients participant au MRV dans un échantillon de pharmacies communautaires de l’Ontario et les services cliniques remboursables qu’ils ont reçus.
Cette étude peut être utile pour les pharmaciens qui mettent en œuvre le MRV en soutenant les possibilités de prestation de services cliniques et en adaptant les soins aux besoins des patients.
In Canada, the responsibility for funding and organizing health care delivery rests predominantly with the provincial and territorial governments. In Ontario, pharmacists are remunerated for the provision of medication reviews for eligible patients, through a publicly funded program called MedsCheck and for drug therapy problem (DTP) identification and resolution services, through the Pharmaceutical Opinion Program.16,17 These programs aim to optimize medication use, encourage patients to be active members in their medication management and promote medication adherence. 16 Guidance provided by the Ontario Ministry of Health and Long-Term Care, the government unit overseeing these programs, recommends that an appointment be scheduled for eligible patients when conducting a MedsCheck. 16
Adoption of models that support appointments between pharmacists and patients has been shown to improve patient and pharmacy outcomes, particularly for older adults. 18 In the appointment-based model (ABM), the pharmacy team schedules all prescription refills and a patient–pharmacist appointment on the same date.19,20 During appointments, the pharmacist addresses medication-related issues (e.g., drug changes, side effect management), optimizes medication regimens (e.g., performs medication reviews, deprescribing) and provides health promotion services (e.g., immunizations, lifestyle education, disease state monitoring). The ABM is associated with increased medication adherence and refills,5,21-25 detection of DTPs,26,27 clinical pharmacy service uptake including vaccinations 28 and patient satisfaction.28,29
As the application of the ABM grows within community pharmacy practice, it is helpful to identify the demographic and other characteristics of individuals receiving care through this model in Canada. This type of information provides insight for community pharmacist teams wishing to adopt, refine and promote the program. The primary objective of this study was to describe key characteristics of patients enrolled in an ABM program within 3 community pharmacies under 1 pharmacy organization in Canada. The secondary objective was to describe reimbursable clinical services received by patients within the Ontario community pharmacy setting after enrolment in the ABM.
Methods
Study design
This was a retrospective descriptive cohort study. The study received approval from the University of Toronto Human Research Ethics Program (REB Protocol # 36810).
Setting
Three independent community pharmacies in Ontario operating within a community pharmacy banner volunteered to participate in the study. Additional pharmacies within the banner implemented the ABM program but were not involved in the study due to technological limitations in extracting data from their dispensing software.
Patients were eligible to be enrolled if they had filled at least 1 chronic oral medication and consented to medication synchronization and patient–pharmacist appointments. Patients were excluded if they changed pharmacies, died or did not complete a consent form on enrolment. The patient’s date of enrolment was recorded to identify a schedule for medication synchronization and appointments. Patient enrolment in the ABM program was at the discretion of pharmacy staff based on the inclusion criteria above.
Intervention
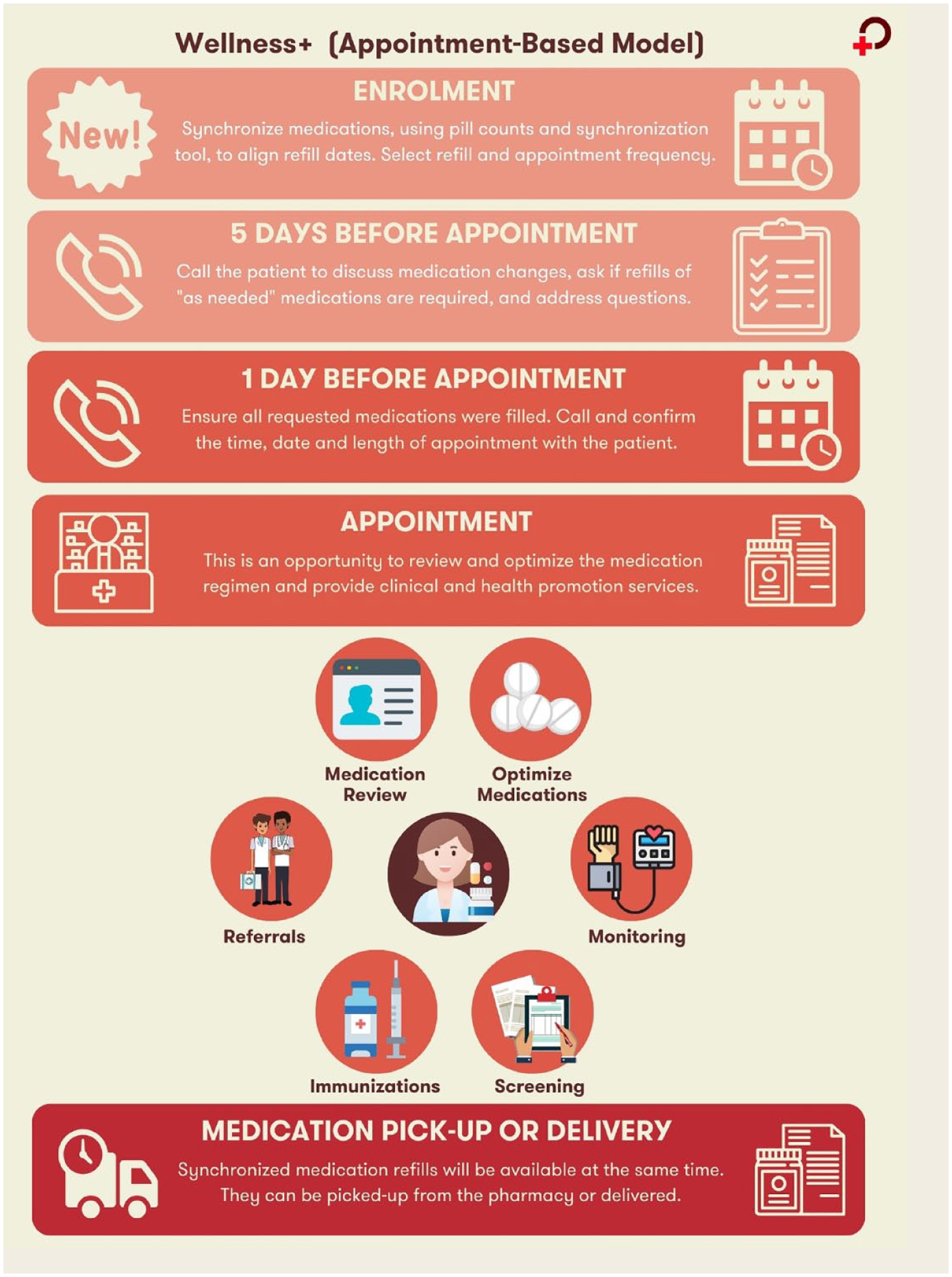
Timing and actions involved in the Wellness+ appointment-based model’s 2 key components: medication synchronization and patient–pharmacist appointments
Data sources and measures
Data were extracted from pharmacy dispensing software from September 2017 to December 2018. Patients were enrolled continuously throughout the data collection period. Data collection began on each patient’s enrolment date, which also served as the index date. Data collection ended on December 18, 2018, for all patients. The ABM program continued in pharmacies after data collection was complete.
The number of medications taken by each patient was determined by the number of unique chronic oral medications dispensed on the patient’s profile at the time of their enrolment into the ABM. Medications were included if they were (1) prescription medications dispensed to the patient and (2) chronic medications deemed as taken regularly for at least 3 months. Medications were excluded if they (1) were taken as needed, (2) did not have administration instructions (e.g., use as directed), (3) could be used for acute conditions (e.g., antibiotics, antivirals, laxatives, analgesics), (4) were not oral solid preparations (e.g., inhalers, sprays, eye/ear drops, patches oral liquids, suppositories, injections, creams) or (5) had a day’s supply that could not be calculated (e.g., medications being tapered or titrated where the day’s supply could not be ascertained from the number of pills and directions for use). Polypharmacy was defined as taking 5 or more medications, recognizing that this is likely an underestimate, as only chronic oral medications were considered. 30 The Anatomical Therapeutic Chemical (ATC) Classification of prescription medications was used to classify medications according to the organ or system upon which they act. 31
Medical conditions were included based on the explicit documentation of a condition in the patient’s pharmacy management system profile or documentation within the patient’s medication review(s) scanned into their profile. Medical conditions were also assigned if the patient was taking a medication where the indication could be confidently inferred according to typical clinical use and if the patient had no other medical condition documented for that medication (Appendix 3). Medical conditions were independently assigned using the clinical judgement of 2 pharmacists on the study team. A third pharmacist performed a quality check to ensure validity of the assigned conditions.
We identified patients who had received clinical services from their pharmacist. This could be a completed medication review (via the MedsCheck program) and/or a prescriber recommendation (via the Pharmaceutical Opinion Program). Documentation in the patient’s profile was reviewed to determine if clinical service provision occurred prior to, on the date of or following enrolment in the ABM. The provision of a MedsCheck medication review included any type of MedsCheck available in Ontario (i.e., MedsCheck Annual, MedsCheck Diabetes, MedsCheck Home and MedsCheck Follow-up). 16 Patients are eligible for a MedsCheck once per year (except for MedsCheck Follow-up, which can be provided more frequently) if they are taking 3 or more chronic medications and are eligible for provincial drug coverage. Visibility to MedsChecks conducted prior to each patient’s enrolment in the ABM was not available. 16 It was assumed that all patients enrolled in the study were eligible for a MedsCheck.
Data analysis
Means and standard deviations were calculated for continuous variables and proportions were calculated for categorical variables. Descriptive statistics and frequencies were analyzed using Stata version 16. 32
Results
Demographics
There were 131 participants across the 3 participating community pharmacies. The mean ± SD age of patients was 70.8 ± 10.5 years, and 51.1% were women (Table 1). Patients were dispensed an average of 5.1 ± 2.7 chronic oral prescription medications. Polypharmacy, defined as taking 5 or more included medications, was experienced by 55.7% of patients.
Baseline demographics of patients enrolled in the appointment-based model at 3 community pharmacies within a pharmacy banner in Ontario, Canada (N = 131)
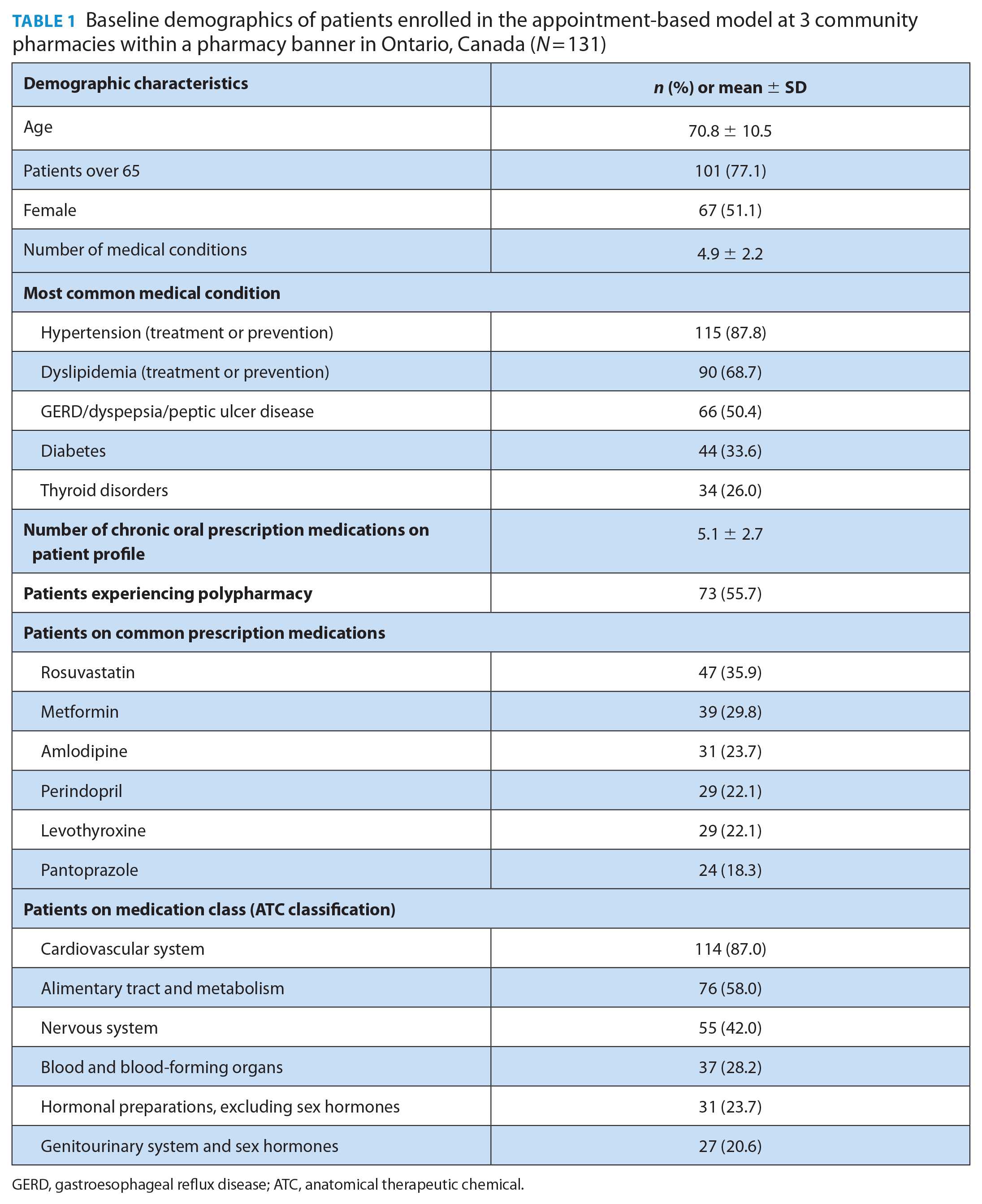
GERD, gastroesophageal reflux disease; ATC, anatomical therapeutic chemical.
Participants had an average of 4.9 ± 2.2 medical conditions. Hypertension (87.8% of patients had this condition), dyslipidemia (68.7%) and gastroesophageal reflux disease/dyspepsia/peptic ulcer disease (50.4%) were most common.
Among the 131 participants, the most frequently dispensed prescription medications were rosuvastatin (35.9% of patients were on this medication), metformin (29.8%), amlodipine (23.7%), perindopril (22.1%), levothyroxine (22.1%) and pantoprazole (18.3%).
The most commonly used class of prescription medications was cardiovascular medication, with 87% of participants taking a medication within this class.
In total, there were 982 patient visits to the pharmacies after enrolment in the ABM program. Patients had an average of 7.5 ± 5.1 visits over the course of their enrolment period, with an average of 295.8 ± 126 days of enrolment. The majority (91.6%) of follow-ups consisted of refill visits and could also include patient–pharmacist appointments where clinical services such as MedsChecks were provided.
Clinical services
There were 82 unique MedsCheck medication reviews provided during the study period. Overall, 74 (56.5%) participants received 1 or more MedsCheck medication review service while enrolled in the ABM program (Table 2). Over half (58.5%) of the 82 MedsCheck services completed while enrolled in the ABM were Annual MedsChecks, while 20.7% were a Follow-Up MedsCheck, 19.5% were a Diabetes MedsCheck and 1.2% were a Home MedsCheck. MedsCheck services most often occurred on the day of enrolment (52/82 or 63.4%) than at subsequent appointments. Almost half of the MedsCheck services (47.6%) noted the identification of 1 or more DTPs, with 53 DTPs noted across all MedsCheck services delivered. The most common DTPs noted during MedsCheck services delivered were “needs additional drug therapy” (22.6%), “therapeutic duplication” (22.6%) and “adverse drug reaction” (17.0%).
Clinical services uptake*
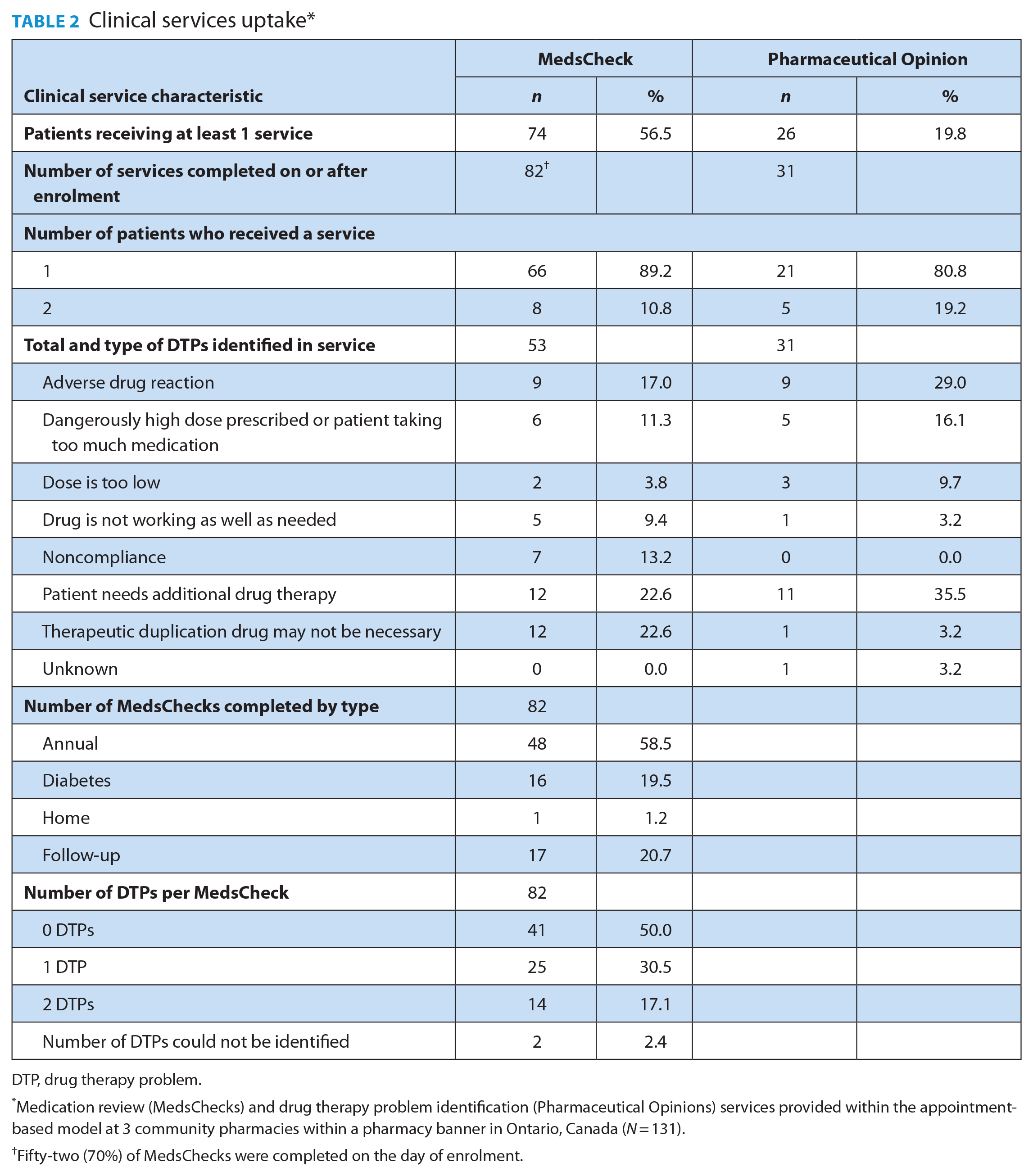
DTP, drug therapy problem.
Medication review (MedsChecks) and drug therapy problem identification (Pharmaceutical Opinions) services provided within the appointment-based model at 3 community pharmacies within a pharmacy banner in Ontario, Canada (N = 131).
Fifty-two (70%) of MedsChecks were completed on the day of enrolment.
Overall, 26 (19.8%) participants received 1 or more Pharmaceutical Opinions (POs) as part of the Pharmaceutical Opinion Program while enrolled in the ABM for a total of 31 POs during the study period (Table 2). Each PO corresponded to 1 DTP; thus, a total of 31 DTPs were identified across all POs. The most common DTPs identified from POs were “needs additional drug therapy” (35.5%), “adverse drug reaction” (29.0%) and “dose too high” (16.1%). There were a number of medications implicated in DTPs identified through POs with no one medication or therapeutic class having a significantly higher incidence than others.
Only 16 patients received a MedsCheck(s) and PO(s). Five of these patients had the same DTP identified (i.e., same patient, same medication, same date) in the MedsCheck and PO documentation. A total of 79 unique DTPs were identified across MedsCheck and PO clinical services throughout this study.
Discussion
In this study, an ABM approach was implemented in 3 independent community pharmacies in Ontario. Consistent with the literature from studies on ABMs used in US pharmacies, patients were older adults living with multiple medical conditions and polypharmacy.26,27 Further, cardiovascular conditions remained the most common disease states among patients receiving care through the ABM in the Canadian environment. 27 These findings may be helpful for pharmacists in tailoring their clinical service offerings to those at risk of major adverse cardiovascular events (e.g., completing smoking cessation certification, stocking influenza and pneumococcal vaccines, being confident in leveraging shared decision-making tools for cardiovascular risk calculation, having patient handouts preprinted). Further, pharmacists can focus their clinical preparation on reviewing hypertension and dyslipidemia guidelines and landmark trials to assist with identifying DTPs for this patient demographic in the ABM and otherwise. As more research on patients receiving care through ABM is published, additional considerations for other prominent medical conditions can emerge and be optimally utilized.
Our findings demonstrate the ABM is a potential support to providing reimbursable clinical pharmacy services, such as MedsCheck medication reviews and POs, within the community pharmacy environment. It is also notable that different types of medication reviews were carried out within the sample studied, demonstrating pharmacists could tailor medication reviews based on patient context. In our study, approximately 1 in 10 visits involved a formal MedsCheck or PO service and over half of the patients (56.5%) received 1 or more MedsCheck medication reviews despite the average length of enrolment being less than a year. The provision of MedsCheck medication review service in this study is higher than was found in other studies.33,34 Dolovich et al. 33 previously reported that approximately 1 in 9 Ontarians (11.1%) received a MedsCheck Annual between 2007 and 2013. Over half of the older adult population who received MedsCheck Annual services received a single MedsCheck Annual over the study period. 33 Ignacy et al. 34 found that 17.3% of Ontarians eligible for public drug coverage received a MedsCheck Annual over a 1-year study period. The higher service provision in our study may have been a result of the clinical opportunity to provide a MedsCheck service within the structure of the ABM, as well as the patient population being composed of older adults experiencing polypharmacy. About 1 in 5 MedsCheck medication review services provided in this study were for follow-up care. This low proportion of formal follow-up services provided reinforces findings from the existing literature and appears to be a consistent issue within community pharmacy practice. 33 The proportion of follow-up in this study may also reflect participants’ varying enrolment periods in the ABM program, where formal follow-up may have occurred outside of the study period. While the ABM was designed to promote continuity of care with different service offerings at follow-ups (which may have been informally or formally documented), this may represent an opportunity to incorporate formal medication review follow-up services into the structured ABM program over a longer program implementation period. 33
Of the medication review services provided, almost half included the identification of 1 or more DTPs. This is lower than the rates of DTPs experienced by older adult primary care populations. 35 It is also less than reported by others who have implemented the ABM. 26 This may have been because our DTP criteria were restricted to prescription medications (e.g., did not include publicly funded vaccines, over-the-counter medications or education/counselling), and those eligible for PO reimbursement (i.e., those with private drug coverage) were ineligible. Additional opportunities to help patients optimize their medications and resolve drug therapy problems likely exist and should be addressed to optimize implementation of the ABM. In terms of the most frequently identified DTPs, our study found that those optimizing medication regimens (needs additional drug therapy) and addressing medication safety issues (therapeutic duplication, adverse drug reaction, dose too high) were highest. This highlights the important role pharmacists can play, when clinical services are implemented, to ensure health conditions are addressed while preventing unsafe or improper medication use.
Strengths of this study include the intervention being conducted by multiple community pharmacists within their existing pharmacy practice sites of different sizes and time in operation, which may promote generalizability. Similar to other studies, the implementation of the ABM was aided by staff engagement and proactive organization of the program.36,37 This highlights the potential to adopt the ABM while maintaining other routine responsibilities.
Limitations of this study include its focus on 3 community pharmacies within a single community pharmacy banner in Ontario, restricted medication inclusion criteria and use of dispensing software to capture clinical service uptake. As only chronic oral prescription medications were included in the analysis, patients may have appeared less medically complex, with a lower prevalence of polypharmacy. Since clinical service uptake was measured through dispensing software, only services eligible for reimbursement were captured, and thus service uptake as well as DTP detection may have been underestimated. Further, the study assumed all patients were eligible for MedsChecks, which may have overestimated the number of eligible patients, as some may have already had a reimbursed MedsCheck within the previous time period prior to ABM, making them ineligible for a reimbursed service and resulting in a conservative calculation of uptake. Patients were also enrolled for different periods of time, which may have limited the full view of services they received. It is also important to note that this study did not set out to compare uptake of MedsCheck and Pharmaceutical Opinion programs with and without implementation of the ABM program. Our results suggest that more research is needed to better understand the impact of the ABM program on clinical service uptake. Future prospective studies could aim to catalogue all dispensed medications and capture clinical services and DTPs addressed during appointments irrespective of reimbursement availability for a set period of time for each patient. Moving forward, the feasibility of implementing the ABM could be evaluated looking at length of appointments, impact on staffing requirements and cost-benefit analysis.
Conclusion
Patients enrolled in the ABM program within a set of 3 Ontario-based pharmacies that were part of a Canadian community pharmacy banner group were most likely to have cardiovascular health conditions and included older adults with multimorbidity experiencing polypharmacy. The study demonstrated that the ABM may have contributed to the relatively high uptake of reimbursable MedsCheck medication reviews compared to previously reported rates in Ontario. However, more research is needed to understand the role of the ABM on MedsCheck Follow-Up services specifically. Pharmacists were able to identify and address drug therapy problems to promote medication safety and ensure that health conditions were effectively managed. Future studies on the benefits and facilitators to implementing the ABM would assist with implementation and uptake of this approach to community pharmacy practice. Efforts to scale the ABM to more medically complex patients, increase DTP identification rates and incorporate formal MedsCheck Follow-Up services may enhance the value of this proactive model of pharmacy care. ■
Supplemental Material
sj-pdf-1-cph-10.1177_17151635241241686 – Supplemental material for The appointment-based model in community pharmacies: Patient demographics and reimbursable clinical services uptake in Ontario
Supplemental material, sj-pdf-1-cph-10.1177_17151635241241686 for The appointment-based model in community pharmacies: Patient demographics and reimbursable clinical services uptake in Ontario by Tiana Tilli, Annalise Mathers, Qiqi Lin, Saleema Bhaidani, Jen Baker, Louis Wei, Paul Grootendorst, Suzanne M. Cadarette and Lisa Dolovich in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Acknowledgements
We thank the pharmacy staff at the study sites who implemented the appointment-based model and assisted with the collection of pharmacy management system data. We also recognize the students who helped at various stages of this project: Brian Tang for the development of the medication synchronization tool; Pooja Patel, Sara Rezahi, Lauren Tailor, Rachel Wong and David Zhaung for data analysis; and Divy Kochar and Shirley Fan for their work in reviewing and updating the literature on the appointment-based model.
Funding:
This work was supported by an Innovation Fund Grant from the Canadian Foundation for Pharmacy (CFP) and through in-kind support from Wholehealth Pharmacy Partners and the University of Toronto’s Leslie Dan Faculty of Pharmacy.
Industry Sponsorship:
This study was not sponsored by industry.
Author Contributions:
AM, TT, QW and LD take full responsibility for the integrity of the data, accuracy of the data analysis and overall content as guarantors. LD is the principal investigator. SB, JB, LW, AM and LD conceptualized the study. SB applied for funding, with the support and guidance of LD and AM. LW performed the initial literature review. SB, JB, LW, AM, SMC, LD and TT designed the study. SB, JB, LW, AM, TT and QW acquired and analyzed the data. PG performed the statistical analysis. AM, TT, QW, PG and LD were involved in interpreting the data. TT and AM drafted the manuscript. All authors reviewed and approved the final version. All authors state that they had complete access to the study data that support the publication.
Informed Consent:
Informed consent was not required for this article.
Declaration of Conflicting Interests:
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Statement of Human Rights:
The study received approval from the University of Toronto Human Research Ethics Program (REB Protocol # 36810).
Data Availability Statement:
The data underlying this article cannot be shared publicly to maintain the privacy of individuals and pharmacies that participated in the study. The data will be shared on reasonable request to the corresponding author.
Supplemental Material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.