
Abstract
Background:
Pharmacist prescribing authority is expanding, while antimicrobial resistance is an increasing global concern. We sought to synthesize the evidence for antimicrobial prescribing by community pharmacists to identify opportunities to advance antimicrobial stewardship in this setting.
Methods:
We conducted a systematic review to characterize the existing literature on community pharmacist prescribing of systemic antimicrobials. We searched MEDLINE, EMBASE and International Pharmaceutical Abstracts for English-language articles published between 1999 and June 20, 2019, as well as hand-searched reference lists of included articles and incorporated expert suggestions.
Results:
Of 3793 articles identified, 14 met inclusion criteria. Pharmacists are most often prescribing for uncomplicated urinary tract infection (UTI), acute pharyngitis and cold sores using independent and supplementary prescribing models. This was associated with high rates of clinical improvement (4 studies), low rates of retreatment and adverse effects (3 studies) and decreased health care utilization (7 studies). Patients were highly satisfied (8 studies) and accessed care sooner or more easily (7 studies). Seven studies incorporated antimicrobial stewardship into study design, and there was overlap between study outcomes and those relevant to outpatient antimicrobial stewardship. Pharmacist intervention reduced unnecessary prescribing for acute pharyngitis (2 studies) and increased the appropriateness of prescribing for UTI (3 studies).
Conclusion:
There is growing evidence to support the role of community pharmacists in antimicrobial prescribing. Future research should explore additional opportunities for pharmacist antimicrobial prescribing and ways to further integrate advanced antimicrobial stewardship strategies in the community setting. Can Pharm J (Ott) 2021;154:xx-xx.
Knowledge Into Practice
Pharmacist prescribing practices have been previously described, but what is needed is a synthesis of the evidence for pharmacist prescribing of systemic antimicrobials.
Community pharmacist prescribing of antimicrobials is beneficial and well received by patients, and the integration of antimicrobial stewardship practices within this context is emerging. We found examples in the literature for pharmacist-led management of uncomplicated urinary tract infections, acute pharyngitis and chronic obstructive pulmonary disease exacerbation. Researchers and evaluators of pharmacist prescribing should consider including more measures of appropriate prescribing and antimicrobial resistance.
Pharmacists are uniquely positioned as accessible health care professionals for outpatient medical care and should have an important role in mitigating antimicrobial resistance. Current research shows that pharmacists are already helping to reduce unnecessary prescribing and increase the appropriateness of prescribing. As their prescribing role continues to advance, there is a need to learn more about how best to engage community pharmacists in more advanced antimicrobial stewardship strategies, which have been shown to be impactful in primary care.
Mise En Pratique Des Connaissances
Les pratiques de prescription des pharmaciens ont été décrites précédemment, mais il est nécessaire de faire une synthèse des données probantes concernant la prescription d’antimicrobiens systémiques par les pharmaciens.
La prescription d’antimicrobiens par les pharmaciens communautaires est bénéfique et bien accueillie par les patients et l’intégration des pratiques de gestion des antimicrobiens dans ce contexte est en train d’émerger. Nous avons trouvé dans la littérature des exemples de prise en charge par des pharmaciens d’infections urinaires non compliquées, de pharyngites aiguës et d’exacerbation de la maladie pulmonaire obstructive chronique. Les chercheurs et les évaluateurs de prescriptions des pharmaciens devraient envisager d’inclure davantage d’indications en ce qui a trait à la prescription appropriée et la résistance aux antimicrobiens.
Les pharmaciens occupent une position unique en tant que professionnels de la santé accessibles pour les soins médicaux ambulatoires et devraient avoir un rôle important dans l’atténuation de la résistance aux antimicrobiens. Les recherches actuelles montrent que les pharmaciens contribuent déjà à réduire les prescriptions inutiles et à accroître le caractère approprié des ordonnances. Alors que leur rôle de prescripteur continue de progresser, il est nécessaire d’en savoir plus sur la meilleure façon d’engager les pharmaciens communautaires dans des stratégies plus avancées de gestion des antimicrobiens, qui se sont révélées avoir une incidence sur les soins primaires.
Introduction
Antimicrobial resistance is a growing concern in Canada and globally. 1 It has been recognized that the vast majority of antimicrobials for humans are used in the outpatient setting and that a significant proportion of these may be inappropriate. In the United States, it is estimated that 30% to 50% of antibiotics prescribed outside of hospitals are inappropriate.2,3 A study of primary care practices in Canada estimated that antibiotics are prescribed unnecessarily for 15.4% of encounters. 4 While some pharmacists are already involved in outpatient antimicrobial stewardship activities and are having an impact on reducing inappropriate prescribing by physicians,5,6 there is an emerging opportunity for community pharmacists to help address antimicrobial resistance in the context of pharmacist prescribing.
Internationally, community pharmacist prescribing is facilitated by various practice models for a variety of health conditions.7,8 In Canada, pharmacists in 9 provinces can independently prescribe medications under provincial legislation, although the extent varies from province to province. 9 In Alberta, pharmacists with Additional Prescribing Authorization (APA) are able to prescribe for a wide range of conditions; in the other 8 provinces, pharmacists can prescribe for a more limited number of ambulatory conditions. 9 Most significantly from an antimicrobial resistance perspective, almost all provincial programs permit pharmacists to prescribe systemic antimicrobials for certain infectious disease conditions. 10
As existing programs expand to include additional infectious conditions and new programs are established, an understanding of what is currently known on the topic of antimicrobial prescribing by community pharmacists will be crucial for advancing antimicrobial stewardship in this setting. A preliminary scan of the literature revealed a lack of systematic review articles characterizing pharmacist prescribing of systemic antimicrobials.7,11 The objective of this systematic review was to synthesize the existing evidence on community pharmacist prescribing of antimicrobials from an antimicrobial stewardship perspective, including public health impacts such as antimicrobial resistance.
Methods
We systematically conducted an evidence synthesis of published literature to answer the following 3 separate but related questions: 1) For which infectious conditions are pharmacists prescribing antimicrobials in the community pharmacy setting, and what models or tools are being used to facilitate this practice? (prescribing context); 2) What is the impact of their prescribing, and how is this being measured? (outcomes); and 3) To what extent are antimicrobial stewardship principles incorporated in study conceptualization, implementation and outcome measures? (incorporation of antimicrobial stewardship).
This systematic review focused on pharmacists practising in outpatient pharmacy settings who prescribe antimicrobials for common infectious conditions. For the purposes of this review, the term antimicrobials refers to systemic antibacterials, antifungals, anthelmintics and antivirals included in American Hospital Formulary System (AHFS) anti-infective class 8:00. 12
Search strategy
We conducted literature searches of 3 databases (MEDLINE, EMBASE and International Pharmaceutical Abstracts) for English-language articles published between 1999 and June 20, 2019. The complete search strategy is described in Appendix 1, available online at www.cpjournal.ca. To identify additional literature, we incorporated hand searches of reference lists of included articles and expert suggestions.
Study selection
Titles, abstracts and full-text screening were independently performed by 2 authors (FK, JW). Conference abstracts were screened by one author (FK or JW). Any disagreement was resolved by discussion and consensus. Disagreements that could not be resolved were reviewed by a third author (VL). Studies were included if the study objective focused on at least 1 of the 3 research questions.
Inclusion and exclusion criteria
To capture models where pharmacists are responsible for patient assessment and initiation of therapy, independent or supplementary pharmacist prescribing (i.e., prescribing using protocols or formularies) was included. However, dependent prescribing models such as collaborative practice agreements were excluded, as these involve referral of patients to a pharmacist after diagnosis by a licensed provider who is ultimately responsible for supervising patient care. 13
Articles were included if they reported on pharmacist prescribing of systemic antimicrobials or included at least 1 infectious condition for which pharmacists were able to prescribe an antimicrobial, excluding otic, ophthalmic and topical antimicrobials. We excluded reviews, letters, opinions and commentaries. We also excluded studies of pharmacists in inpatient settings, institutional settings (e.g., long-term care) or specialized ambulatory clinics (e.g., travel medicine, oncology, infectious disease), as well as studies from low- and middle-income countries and studies based on pharmacist self-reported data (e.g., pharmacist perceptions and opinions on prescribing).
Data extraction and synthesis
Data extraction for predefined variables was undertaken by one author (JW) and verified by a second author (VL). The relevance of study concepts or outcomes to antimicrobial stewardship was determined using a combination of frameworks such as Public Health Ontario’s Antimicrobial Stewardship Strategies 14 and other literature describing features of outpatient antimicrobial stewardship programs.15-17 To describe the current state and gaps in research, we categorized outcomes into the following categories relevant to antimicrobial stewardship: prescribing outcomes, patient-centred outcomes (i.e., clinical outcomes, health care utilization, access to care, patient satisfaction), costs and microbial measures (i.e., antimicrobial susceptibility or resistance patterns, community-associated Clostridium difficile infection rates, infection rates with multidrug-resistant organisms).16,17 Due to the broad inclusion criteria, we performed a descriptive analysis and identified themes related to the research questions.
Results
A total of 3790 unique citations were identified from the database search strategy, which also included 7214 conference abstracts. Three additional studies were included after hand-searching the reference lists of the included studies and expert suggestion. Altogether, 14 articles met the inclusion criteria (Appendix 2, available online at www.cpjournal.ca).
There were 6 studies conducted in Canada,10,18-22 6 in the United Kingdom,23-28 1 in New Zealand 29 and 1 in the United States 30 (Table 1). The study designs included 5 interventional studies without comparison,18,23-25,28 3 observational studies,20,21,26 2 nonrandomized controlled trials,19,27 1 before-after uncontrolled study, 29 2 economic analyses22,30 and 1 environmental scan. 10 Interventional studies without comparison were evaluations of program implementation or interventions that reported outcomes without comparison to preimplementation or to a control group. All 14 studies included a declaration on conflicts of interest. Thirteen studies reported on funding sources. Of these, 5 did not receive any external funding.18,20,25,26,30 The other studies reported funding from an academic institution,10,24 government, 23 professional association,19,21,23,29 foundation21,22,27 or private industry.24,29 Six of the included studies specifically described remuneration for pharmacist services: fees were paid by patients in 2 studies,18,24 paid by the study itself in 2 studies19,25 and paid to the pharmacy through government reimbursement in 2 studies.28,31 An environmental scan of Canadian provinces reported the status of pharmacist remuneration for each province, which was variable. 10
Overview of studies evaluating pharmacist prescribing of antimicrobial agents
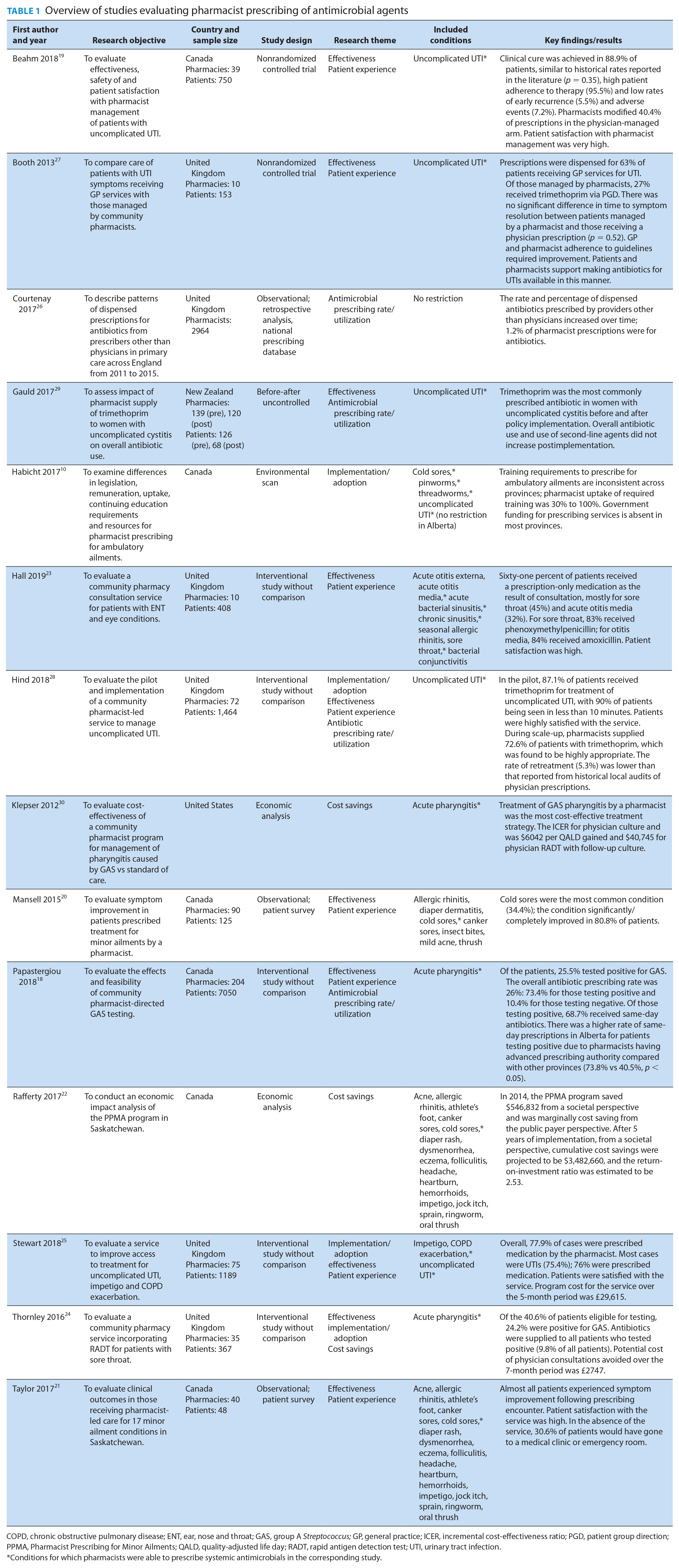
COPD, chronic obstructive pulmonary disease; ENT, ear, nose and throat; GAS, group A Streptococcus; GP, general practice; ICER, incremental cost-effectiveness ratio; PGD, patient group direction; PPMA, Pharmacist Prescribing for Minor Ailments; QALD, quality-adjusted life day; RADT, rapid antigen detection test; UTI, urinary tract infection.
Conditions for which pharmacists were able to prescribe systemic antimicrobials in the corresponding study.
Analysis of the included studies resulted in the identification of several broad themes, most commonly effectiveness (n = 10)18-21,23-25,27-29 and patient experience (n = 8).18-21,23,25,27,28 Other themes were implementation and adoption (n = 4),10,24,25,28 antimicrobial prescribing rate or utilization (n = 4)18,26,28,29 and cost savings (n = 3).22,24,30
Prescribing context
Six studies described pharmacist prescribing for uncomplicated urinary tract infection (UTI) or cystitis,10,19,25,27-29 4 studies described prescribing for acute pharyngitis or sore throat18,23,24,30 and 4 described prescribing for cold sores.10,20-22 Other conditions were acute otitis media, 23 acute bacterial sinusitis, 23 chronic bacterial sinusitis, 23 chronic obstructive pulmonary disease (COPD) exacerbation 25 and pinworms and threadworms. 10 Seven studies described pharmacists prescribing antimicrobials using independent authority,10,18-22,26 whereas 6 described protocol-based prescribing models including Patient Group Direction (PGD).23-25,27-29 One economic study did not explicitly assume a model of prescribing. 30 Prescribing model (independent or supplementary) was related to the jurisdiction rather than health condition; independent prescribing models were described for all studies in Canada, with 1 example in the United Kingdom, whereas multiple studies described supplementary models in the United Kingdom, with 1 example in New Zealand.
Outcomes
The impact of pharmacist prescribing was frequently measured using a combination of prescribing and patient-centred outcomes (Table 2). Reporting on prescribing outcomes tended to be descriptive and was included in 8 studies; all 8 reported on antimicrobial prescribing rate or utilization,18,23-29 while 2 included drug selection26,29 and 2 examined guideline concordance.27,28 For patient-centred outcomes, health care utilization (e.g., primary care clinic/office visits, hospital/emergency room visits) (n = 9),18-21,23-25,27,28 patient satisfaction (n = 8)18-21,23,25,27,28 and access to care (n = 8)18-21,24,25,27,28 were most commonly reported.
Types of study outcomes reported
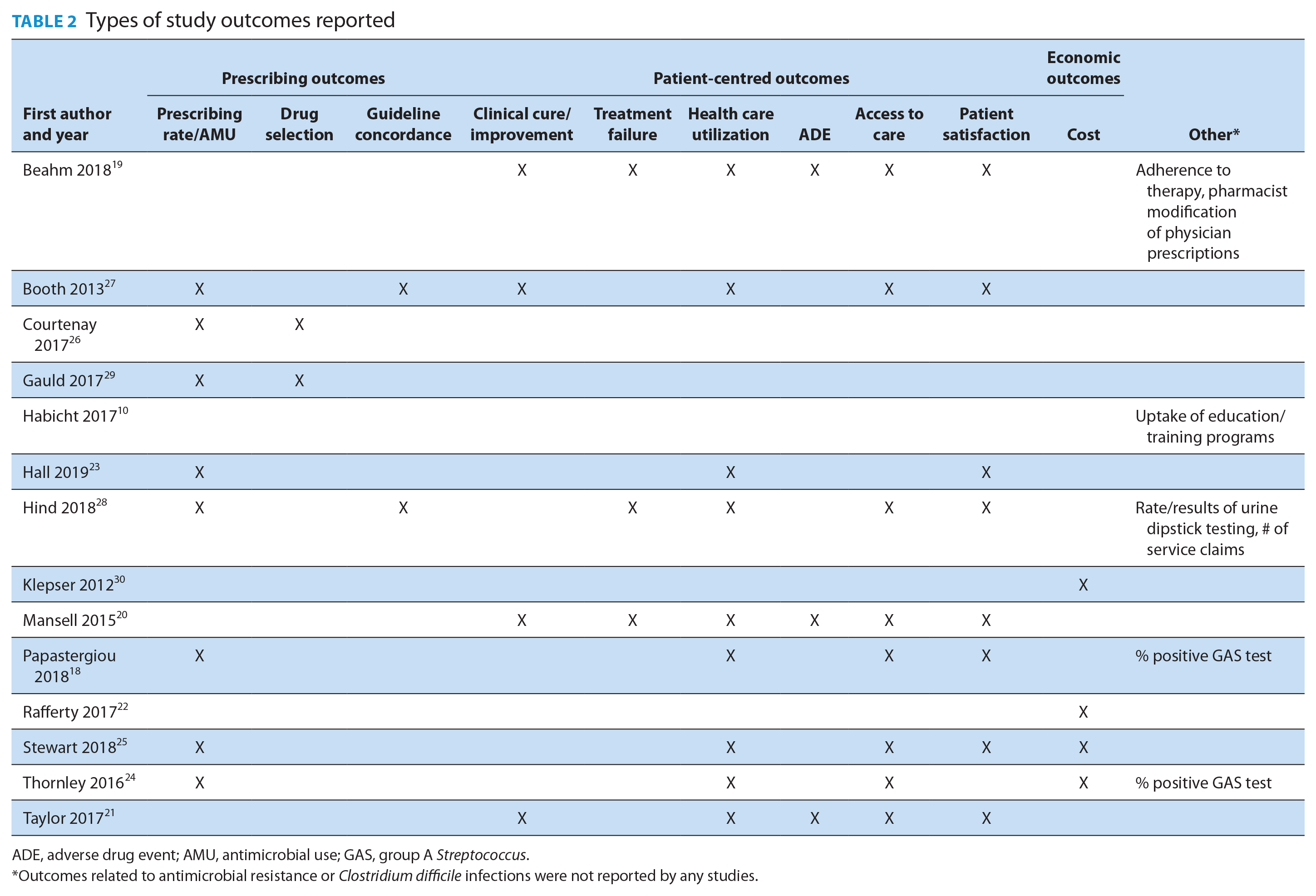
ADE, adverse drug event; AMU, antimicrobial use; GAS, group A Streptococcus.
Outcomes related to antimicrobial resistance or Clostridium difficile infections were not reported by any studies.
Overall, pharmacist prescribing in these studies was found to be safe and effective and was associated with a positive patient experience (Table 1). High levels of clinical cure or symptom improvement following pharmacist prescribing were reported in all 4 studies evaluating this outcome.19-21,27 For patients with UTI, 2 studies reported low rates of early recurrence or need for retreatment following pharmacist management,19,28 and another study found no significant difference in time to symptom resolution between patients managed by a pharmacist and those receiving a physician prescription. 27 Patients with UTI also presented significantly sooner from the time of symptom onset to pharmacists compared with physicians.19,27 In general, patients expressed high levels of satisfaction with pharmacist-led management18-21,23,25,27,28 and indicated being able to access care sooner and/or with greater convenience.18-21,25,27,28
Seven studies describing health care utilization outcomes found that pharmacist-led care, including prescribing, was associated with actual or potential avoidance of other health care utilization (Table 1).18,20,21,24,25,27,28 Of the 3 studies that reported on health care utilization following a pharmacist encounter, 2 found low rates of reconsultation with other health care providers (3%-4%),20,23 and 1 found a very low rate of physician or emergency department visits due to adverse events (0.7%). 19
Cost was the focus of 2 economic analyses22,30 and was included in 2 other studies (Table 1).24,25 One economic impact analysis of a broader provincial ambulatory ailments program found significant cumulative cost savings from a societal perspective and a positive return on investment (ROI) ratio 5 years postimplementation. 22 The other economic analysis, comparing pharmacist-led treatment of group A Streptococcus (GAS) pharyngitis to physician management, found the pharmacist strategy to be the most cost-effective. 30
Incorporation of antimicrobial stewardship
Seven of 14 studies identified antimicrobial stewardship as a consideration for study design and incorporated antimicrobial stewardship strategies (Table 3) that either resulted in improvement or helped identify areas for improvement in antimicrobial prescribing (Table 1).18,19,24-26,28,29 Two studies conducted drug-use evaluation to identify trends and opportunities for antimicrobial stewardship.26,29 One study described education and training specific to antimicrobial stewardship for pharmacists prior to implementing a community pharmacy service to manage UTI, impetigo and COPD exacerbation. 25 Papastergiou et al. 18 and Thornley et al. 24 examined the impact of a rapid antigen detection test (RADT) in community pharmacies as a way to decrease unnecessary antibiotic use for acute pharyngitis and found that this strategy resulted in an overall prescribing rate of 26% 18 and 24%. 24 Several studies implemented uncomplicated UTI treatment guidelines/pathways/algorithms for pharmacist prescribing.25,28,29,27 In the National Health Service (NHS) Grampian project, all cases of pharmacist prescribing of trimethoprim for uncomplicated UTI were determined to be appropriate. 28 Gauld et al. 29 found no increase in overall antibiotic use or use of second-line agents postimplementation of pharmacist prescribing for uncomplicated UTI. Additionally, in the RxOUTMAP study, pharmacists performed prescription optimization for 40% of antibiotic prescriptions written by physicians. 19
Overview of antimicrobial stewardship strategies incorporated
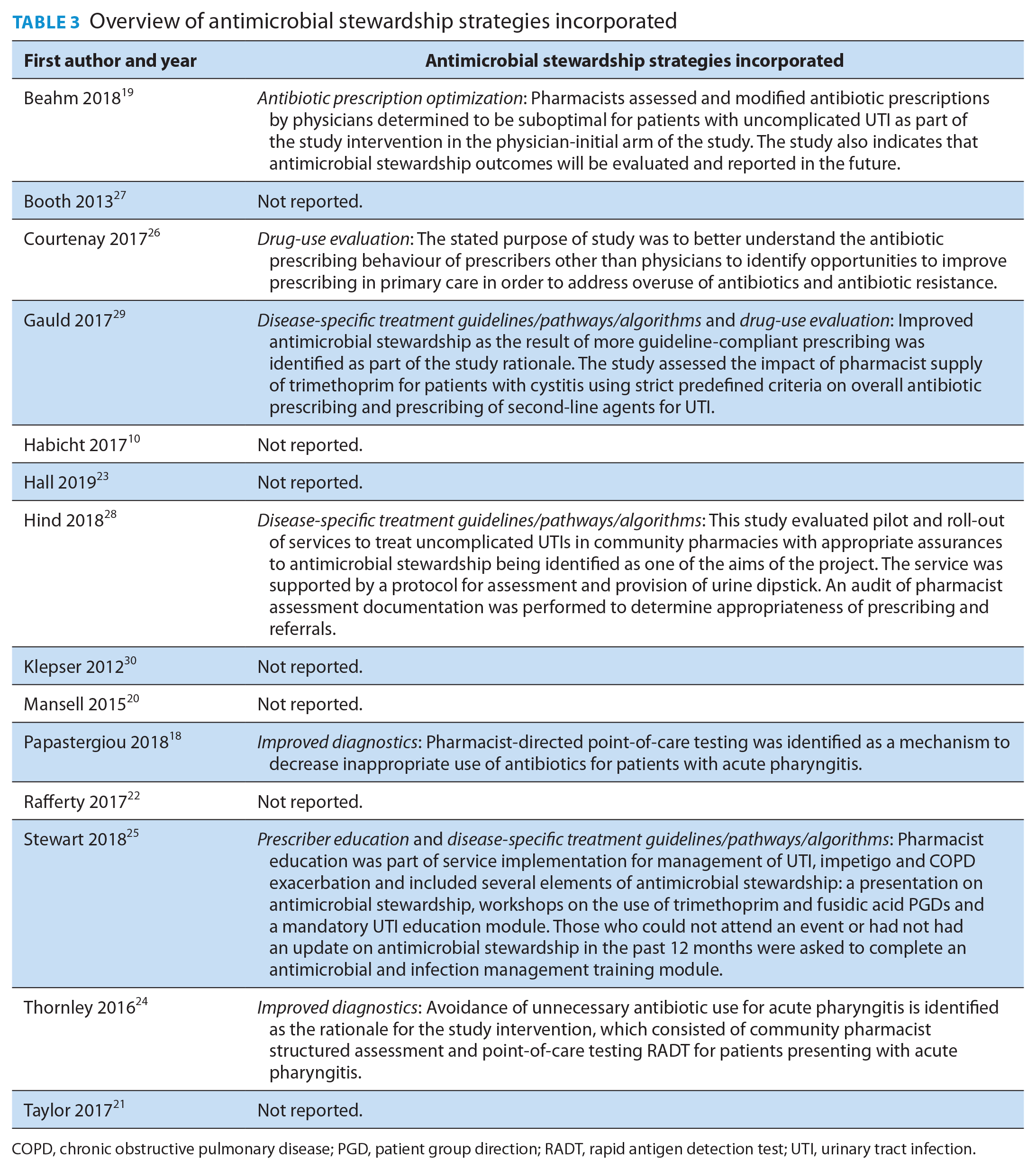
COPD, chronic obstructive pulmonary disease; PGD, patient group direction; RADT, rapid antigen detection test; UTI, urinary tract infection.
We observed notable overlap between outcomes considered relevant to outpatient antimicrobial stewardship16,17 and those included in the 14 studies (Figure 1). Eight studies included at least 1 antimicrobial prescribing outcome; all 8 reported on antimicrobial prescribing rate,18,23-29 2 reported on drug selection26,29 and 2 assessed guideline concordance.27,28 No studies reported on duration of therapy, antimicrobial escalation or de-escalation, use of antimicrobials for indications where antimicrobials are unnecessary or rarely required or vaccination rates. Eleven of 14 studies included at least 1 patient-centred outcome relevant to antimicrobial stewardship. Four studies reported on cost outcomes.22,24,25,30 No studies reported microbial or resistance measures. One study indicated that further analysis of antimicrobial stewardship outcomes would be reported in the future. 19
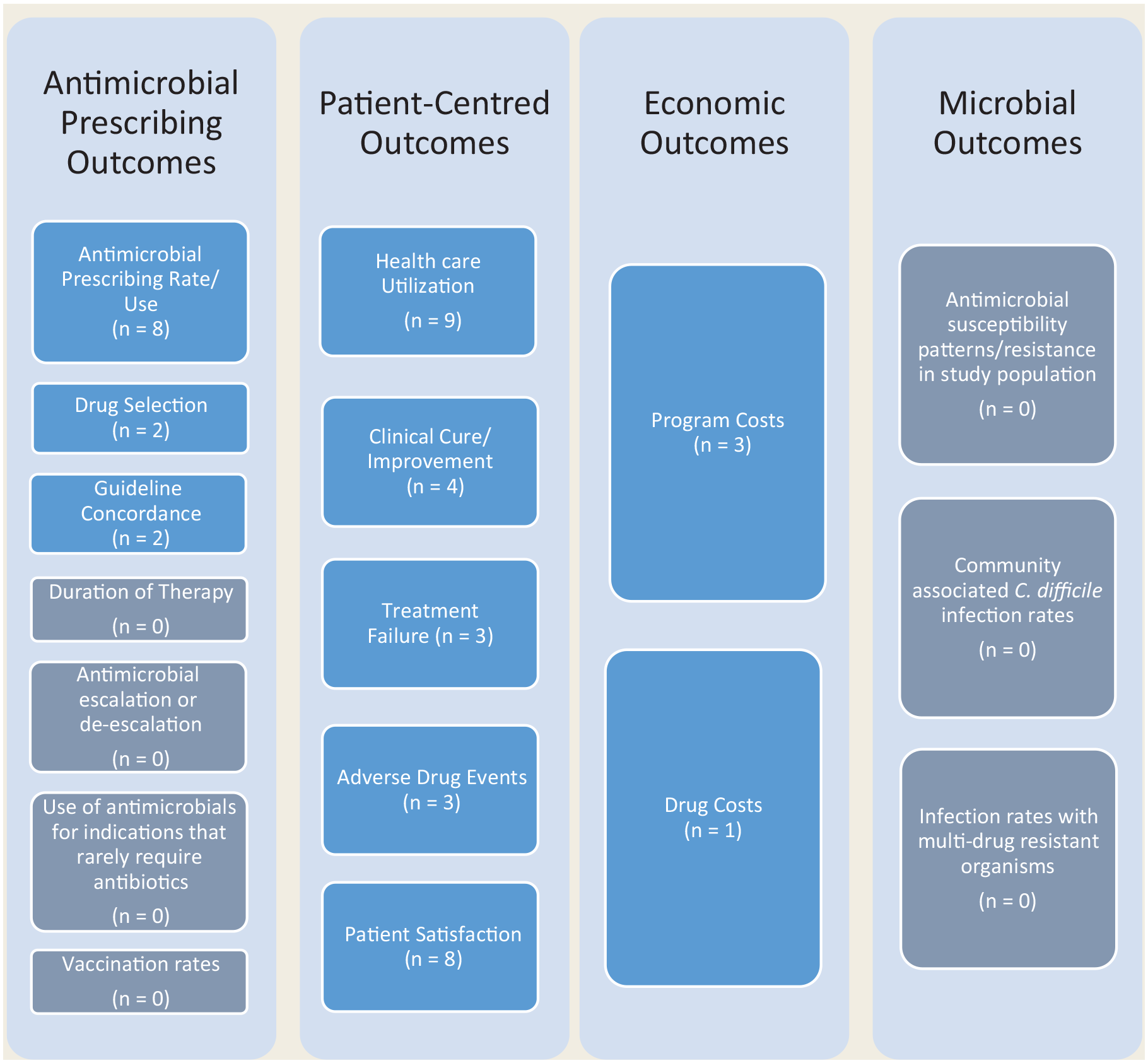
Mapping of outcomes from included studies to outcomes relevant to outpatient antimicrobial stewardship programs
Discussion
In this systematic review, we found both the role of pharmacists in antimicrobial prescribing and the integration of antimicrobial stewardship practices in the community pharmacy setting to be associated with patient benefits, health care system benefits and high patient satisfaction. The literature describes both independent and supplementary prescribing models for community pharmacists.
The most common health conditions for which community pharmacists prescribed antimicrobials were uncomplicated UTI, acute pharyngitis and cold sores. Studies found pharmacist prescribing to be effective and safe; for uncomplicated UTI, pharmacist management was associated with high rates of clinical cure, low rates of recurrence and low rates of adverse events requiring a physician or emergency department visit.19,27,28 There is also evidence that pharmacist prescribing for uncomplicated UTI does not increase overall antibiotic use or use of second-line agents. 29
Half of studies (n = 7) reported inclusion of 1 or more strategies for the purposes of advancing antimicrobial stewardship: improved diagnostics,18,24 disease-specific treatment guidelines,25,28,29 prescriber education, 25 antibiotic prescription optimization 19 and drug-use evaluation.26,29 Six of these studies aimed to improve prescribing for acute pharyngitis18,24 or uncomplicated UTI.19,25,28,29 Two studies highlight the role of pharmacists in improving prescribing for acute pharyngitis, which has been identified as a condition with a high rate of unnecessary antibiotic prescribing among primary care physicians, as it is frequently of viral etiology. 4 In these studies, pharmacist-facilitated RADT for acute pharyngitis resulted in a prescribing rate of 26% 18 and 24%, 24 in contrast to previous studies of primary care physicians in these same jurisdictions where antibiotics were prescribed to 62% to 70% of patients presenting with acute pharyngitis.4,32 Pharmacists can also play a key role in improving appropriateness of prescribing due to their high adherence to prescribing criteria and role in optimizing prescriptions generated by physicians.19,28 While the RxOUTMAP substudy reporting on the antimicrobial stewardship outcomes was not yet published at the time of our search, it was able to show that community pharmacists’ prescribing was also highly appropriate in this context. 33
The landscape of pharmacist antimicrobial prescribing in the community setting is comparable to that in the hospital setting as it relates to prescribing models and positive impact,34-36 except that the role of pharmacists in hospital antimicrobial stewardship programs (ASPs) is much better defined and well established.37,38 As seen in this systematic review, pharmacist involvement in outpatient antimicrobial stewardship has traditionally been described as relating to education, guideline development and implementation, point-of-care testing and patient counselling,5,6 and we note gaps in their involvement in more advanced primary care–focused evidence-based ASP strategies such as public commitment posters, viral prescriptions and shared decision making. Public commitment posters entail clinicians displaying a message about committing to appropriately prescribe antibiotics. This has been shown to reduce inappropriate antibiotic prescribing for acute respiratory infections by 20% in primary care clinics 39 and may be very feasible to implement in community pharmacies given that this requires few resources. Viral prescriptions and shared decision making could potentially be integrated into patient counselling activities, especially in the context of pharmacist-led management of acute pharyngitis, otitis media and sinusitis. Pharmacists could provide patients presenting with probable viral infections with a “prescription” that contains written educational information and non-antibiotic management options. This strategy has previously been identified to be useful by community-based physicians and patients. 40 Finally, pharmacists may help improve patient understanding of the risks and benefits of antibiotic therapy through shared decision making, which been associated with significant reductions in antibiotic use for acute respiratory infections, while also improving patient satisfaction with the decision-making process.41,42 Although this is a more resource-intensive strategy, pharmacists have successfully leveraged shared decision making for other health conditions, and we believe that this could be adopted for antimicrobial stewardship in the community pharmacy setting, as existing tools are readily available.38,39 Further research should evaluate the feasibility and impact of including these advanced strategies in the community pharmacy setting.
Although we observed significant overlap between reported study measures and those relevant to outpatient ASPs, there was variability in the operationalization of pharmacist prescribing across studies, as well as the types of conditions included. More comprehensive inclusion of antimicrobial prescribing and microbial outcomes in future studies will help increase alignment with the aims of antimicrobial stewardship and improve generalizability of results.
Some limitations to this systematic review should be noted. First, our search only included published literature. However, based on the diversity of published literature included, we believe that the results of our systematic review are a reasonable reflection of the available evidence on the topic of interest. Second, while we were unable to perform a formal quality appraisal due to the wide variability of study designs and lack of a single appropriate quality assessment tool, it should be noted that since the studies included in this review were not randomized controlled trials, there is an inherent risk of bias. Yet, given the challenges with conducting randomized controlled trials of pharmacist prescribing compared with usual care (e.g., pharmacist workflow, uptake of pharmacist prescribing authority), nonrandomized controlled trials and before-after uncontrolled studies are more pragmatic and may be the next best level of evidence in this context. Sources of funding such as private industry may also present additional bias; however, all studies included a statement on conflict of interest, and of the 2 studies that received funding from private industry, explicit details on conflict of interest were provided.24,29
Conclusion
Our systematic review highlights the available evidence demonstrating that community pharmacist prescribing of antimicrobials is associated with benefits to patients and the health care system as well as a high degree of patient satisfaction. Our review also identified an existing foundation to further advance antimicrobial stewardship in the community pharmacy setting as pharmacists are already helping to reduce unnecessary prescribing while increasing appropriateness. In order to expand pharmacists’ role in addressing antimicrobial resistance, future research should explore additional areas for pharmacist prescribing of antimicrobials, provide opportunities to incorporate advanced antimicrobial stewardship strategies and include more comprehensive evaluation of pharmacist prescribing with respect to antimicrobial prescribing and microbial outcomes in the community setting. ■
Supplemental Material
sj-pdf-1-cph-10.1177_1715163521999417 – Supplemental material for Community pharmacist prescribing of antimicrobials: A systematic review from an antimicrobial stewardship perspective
Supplemental material, sj-pdf-1-cph-10.1177_1715163521999417 for Community pharmacist prescribing of antimicrobials: A systematic review from an antimicrobial stewardship perspective by Julie Hui-Chih Wu, Fatima Khalid, Bradley J. Langford, Nathan P. Beahm, Mark McIntyre, Kevin L. Schwartz, Gary Garber and Valerie Leung in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Supplemental Material
sj-pdf-2-cph-10.1177_1715163521999417 – Supplemental material for Community pharmacist prescribing of antimicrobials: A systematic review from an antimicrobial stewardship perspective
Supplemental material, sj-pdf-2-cph-10.1177_1715163521999417 for Community pharmacist prescribing of antimicrobials: A systematic review from an antimicrobial stewardship perspective by Julie Hui-Chih Wu, Fatima Khalid, Bradley J. Langford, Nathan P. Beahm, Mark McIntyre, Kevin L. Schwartz, Gary Garber and Valerie Leung in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Acknowledgements
The authors thank Susan Massarella from Knowledge Services, Public Health Ontario for designing and conducting the literature search.
Author Contributions:
JW conceptualized the project, designed the research, screened titles and abstracts and full text, extracted data, analyzed data, interpreted the data, cowrote the final draft and critically revised the paper for intellectual content. FK conceptualized the project, designed the research, screened titles and abstracts and full text, interpreted the data and critically revised the paper for intellectual content. BL conceptualized the research, interpreted the data and critically revised the paper for intellectual content. NB and MM interpreted the data and critically revised the paper for intellectual content. KS and GG conceptualized the project, interpreted the data and critically revised the paper for intellectual content. VL supervised the project, extracted data, analyzed data, interpreted the data, cowrote the final draft and critically revised the paper for intellectual content. All authors approved the final draft of the manuscript.
Conflict of Interest:
None.
Funding:
The authors received no financial support or industry sponsorship for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.