
Abstract

Introduction
Influenza is an important public health concern, especially among vulnerable populations such as young children, seniors, individuals with chronic medical conditions and immunocompromised patients. 1 It is estimated that influenza infection leads to 12,200 hospitalizations and 3500 deaths annually in Canada. 2 Fortunately, vaccination can prevent influenza infection and the spread of the virus. A vaccine is developed annually for each influenza season based on the circulating viral strains expected to be dominant during the season. 3 It can take up to 2 weeks after administration before an influenza immunization is effective in providing protection against influenza, 1 and thus early immunization each influenza season is important. Publicly funded community pharmacy influenza programs exist in all Canadian provinces and 1 territory (Table 1). Alberta and British Columbia were the first to support publicly funded community pharmacy influenza immunization programs, offering the service since the 2009/2010 influenza season. At the other extreme, Quebec and the Yukon offered the service for the first time this 2020/2021 influenza season, and no service exists in the Northwest Territories or Nunavut. The purpose of this research brief is to introduce the Ontario Pharmacy Evidence Network (OPEN) Atlas of Community Pharmacy Influenza Immunizations tool and describe the uptake of influenza immunization services in Ontario over time. Our case example may help support pharmacy influenza immunization service planning and similar immunization planning for coronavirus disease 2019 (COVID-19).
Summary of publicly funded community pharmacy influenza immunization services across Canada*
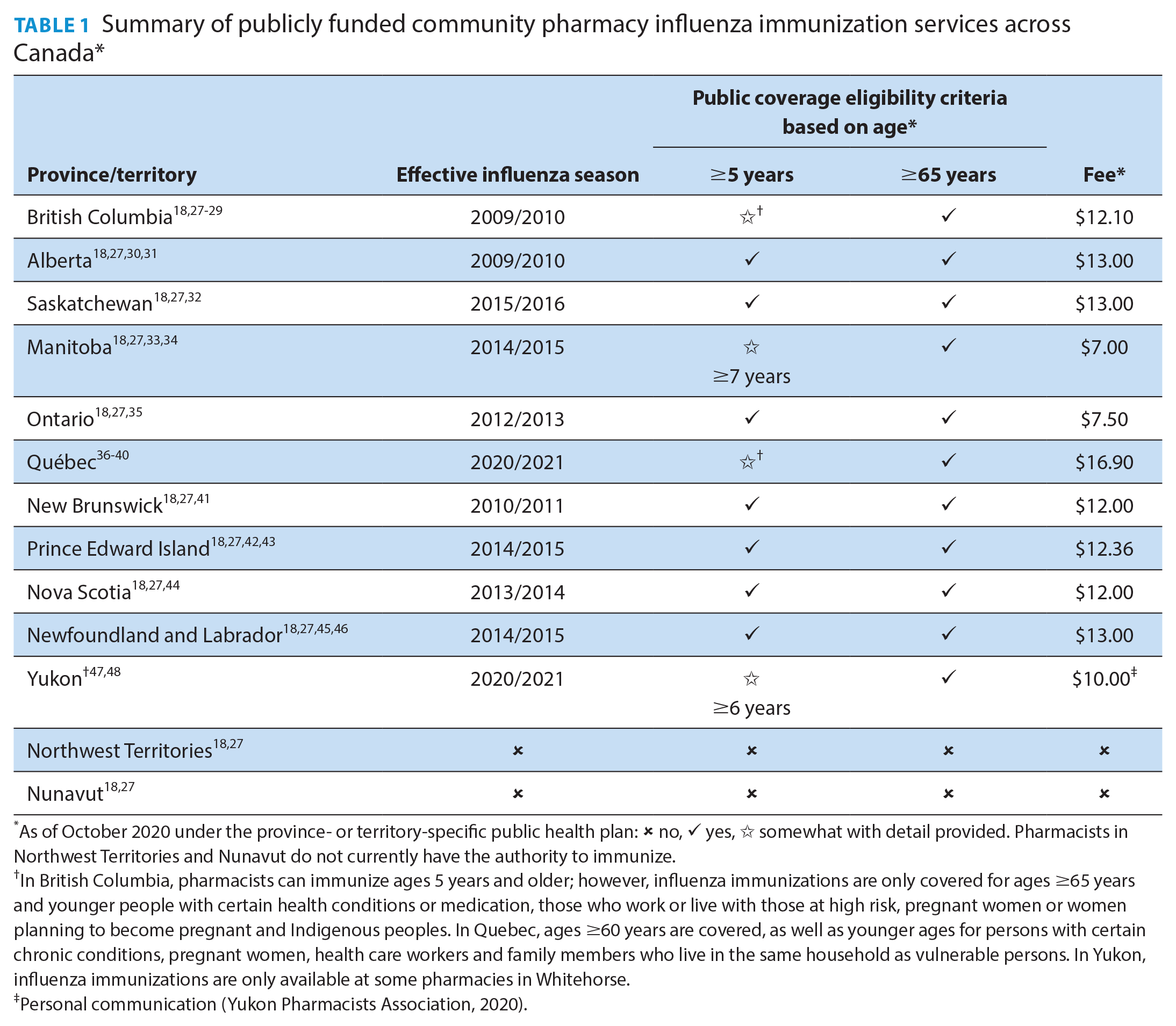
As of October 2020 under the province- or territory-specific public health plan: ✘ no, ✓ yes, ☆ somewhat with detail provided. Pharmacists in Northwest Territories and Nunavut do not currently have the authority to immunize.
In British Columbia, pharmacists can immunize ages 5 years and older; however, influenza immunizations are only covered for ages ≥65 years and younger people with certain health conditions or medication, those who work or live with those at high risk, pregnant women or women planning to become pregnant and Indigenous peoples. In Quebec, ages ≥60 years are covered, as well as younger ages for persons with certain chronic conditions, pregnant women, health care workers and family members who live in the same household as vulnerable persons. In Yukon, influenza immunizations are only available at some pharmacies in Whitehorse.
Personal communication (Yukon Pharmacists Association, 2020).
Methods
The OPEN Atlas of Community Pharmacy Influenza Immunizations tool provides interactive descriptive summaries for 3 indicators: trends (monthly number of immunizations by region and type [injection or intranasal]), age and sex (counts and rates by age groups and sex and overall age distribution by sex) and maps (regional age- and sex-standardized rates). Detailed methods have been summarized previously. 4 In brief, the Ontario Drug Benefit Database was used to identify all influenza immunization claims submitted by community pharmacies from program launch in October 2012 to March 31, 2020 (2012/2013 to 2019/2020 influenza seasons), and the Registered Persons Database was used to determine patient age, sex and postal code at the time of first service delivery. These data sets were linked using unique encoded identifiers and analyzed at ICES. Statistics Canada data were used to obtain population estimates by age group, sex and region, as well as spatial boundaries for maps.4-6
Persons under 5 years (pharmacies in Ontario can only immunize individuals aged 5 years and older), with missing age or sex, or with death date before the first pharmacist-administered immunization date, were excluded. Patients with missing postal code were excluded from regional analyses. Only the first pharmacy influenza immunization claim per patient within each influenza season was considered.
Results
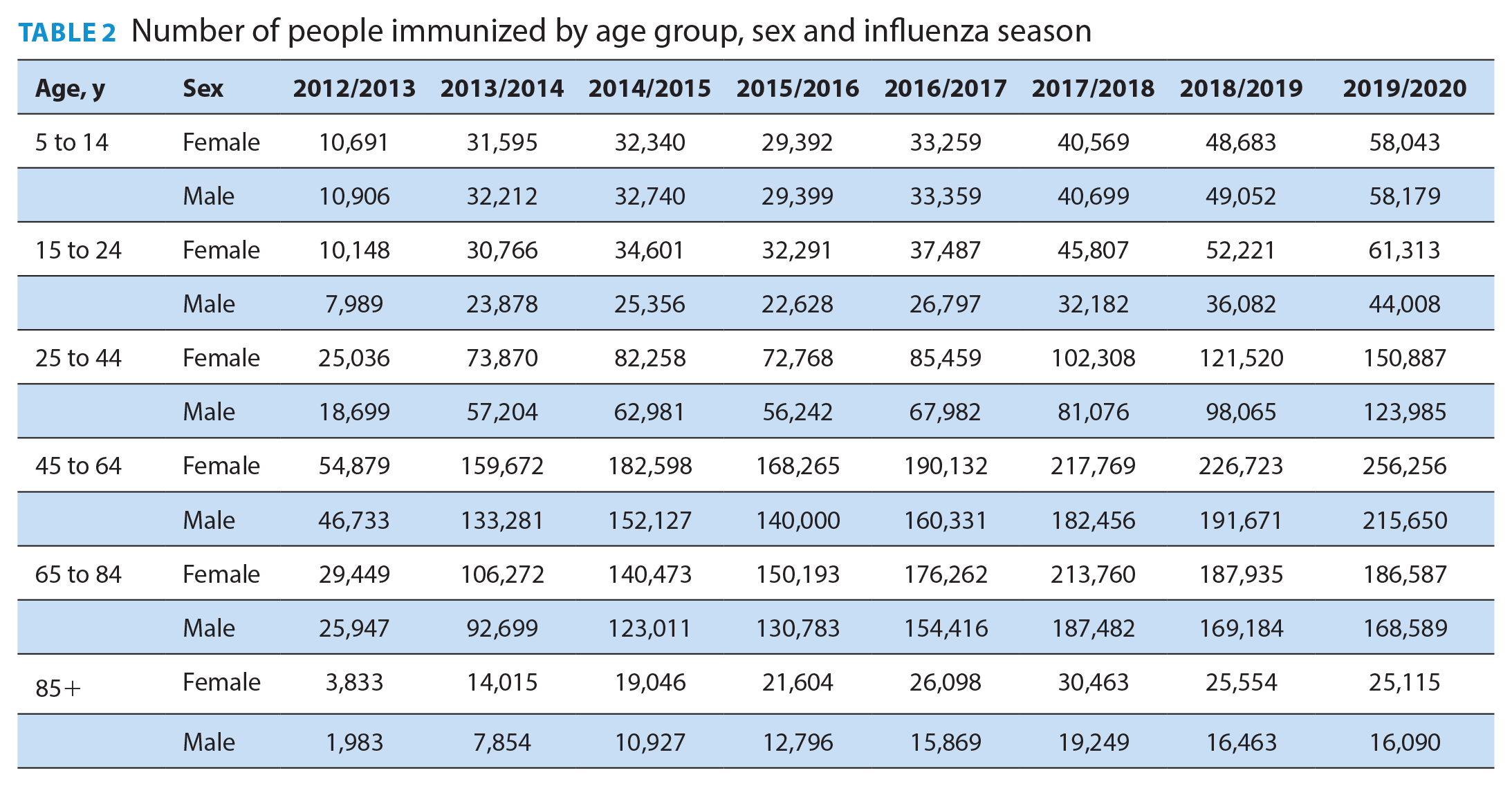
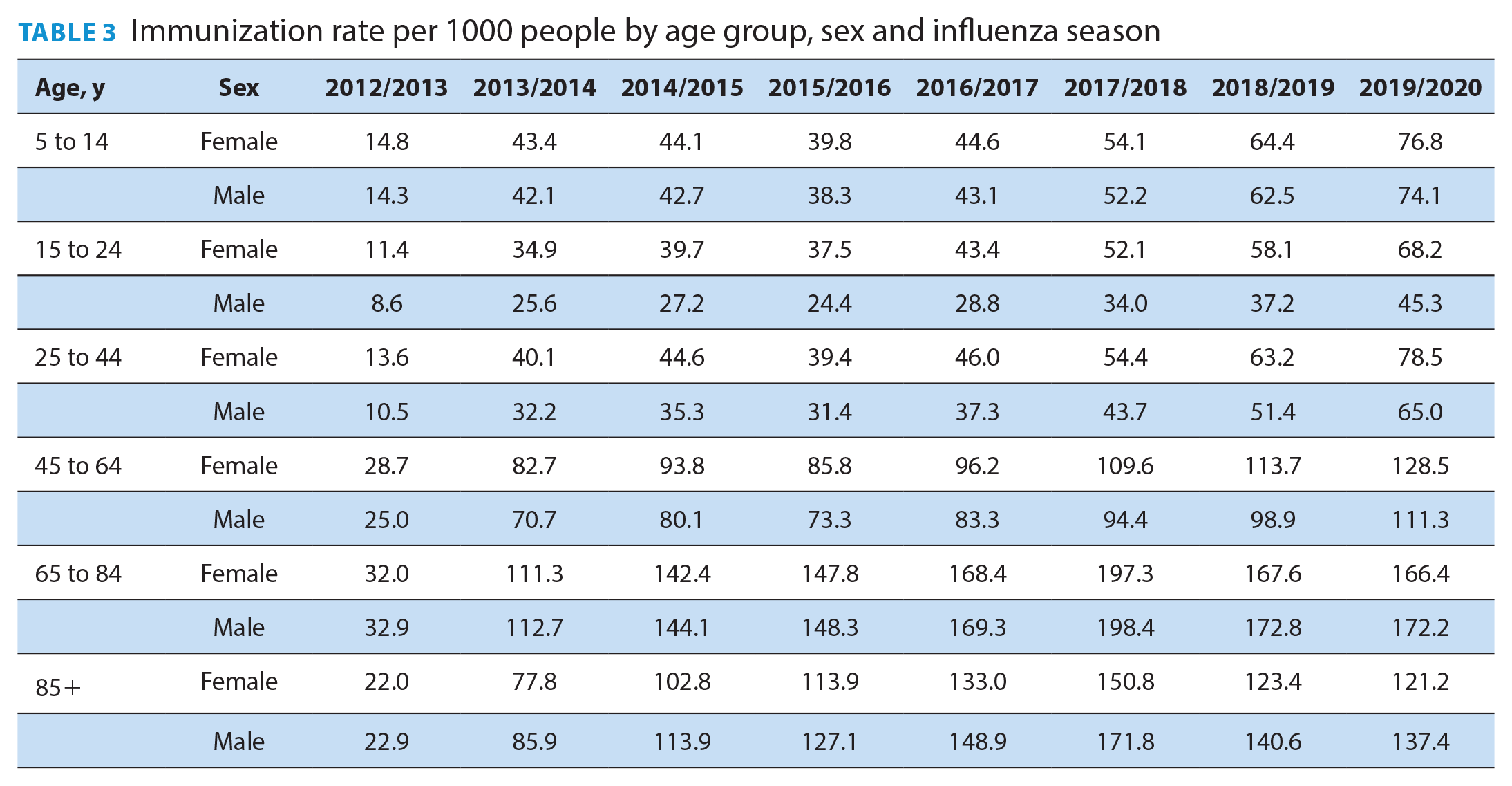
A total of 7,563,556 immunizations were administered in community pharmacies to 3,109,827 unique patients over the 2012/2013 to 2019/2020 seasons. The number of immunizations increased over time, starting from a low of 246,293 in 2012/2013 and reaching a high of 1,364,702 in 2019/2020. Results are presented as histograms in an interactive format as part of the OPEN Atlas of Community Pharmacy Influenza Immunizations tool and summarized numerically by age and sex in Tables 2 and 3. Most immunizations were completed in November of each season (Figure 1). Intranasal immunizations were only covered during the 2015/2016 to 2018/2019 seasons, representing 1.6% of total immunizations over those seasons. One might anticipate that removing intranasal immunizations as an option could translate into lower pediatric immunization rates, yet we found that immunization rates in community pharmacy were highest in the 2019/2020 season compared to any prior season for age groups younger than 65 years. Of interest, intranasal immunizations were added back as a publicly funded option during the 2020/2021 season on November 30, 2020. 7 Displacement from a reduction in public health influenza programs likely played a role in the increased use of community pharmacy influenza program over time in Ontario. The Atlas provides cross-sectional summaries, and thus we cannot comment on the longitudinal change within specific individuals, but results identifying higher rates over time among those aged younger than 65 years are encouraging.
Number of people immunized by age group, sex and influenza season
Immunization rate per 1000 people by age group, sex and influenza season
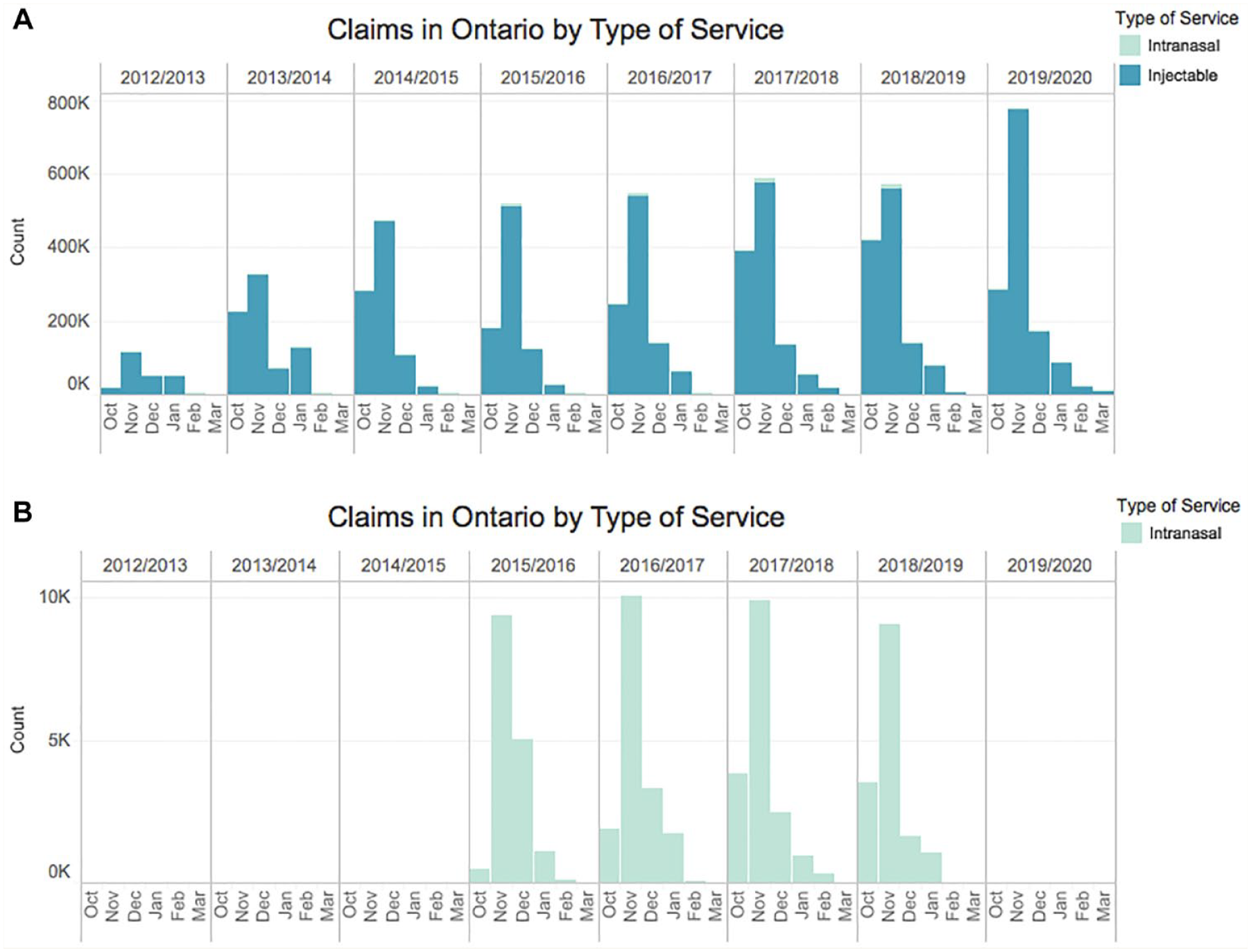
Monthly number of community pharmacy influenza immunizations in Ontario*
Among those aged 65 years or older, counts and rates were highest in the 2017/2018 influenza season. Of interest, the high-dose influenza vaccine that was highly marketed to seniors was not available for administration as part of the publicly funded program in community pharmacies for the 2018/2019 and 2019/2020 seasons but was available through physician offices. 8 The drop in community pharmacy immunization services among seniors when they were encouraged to be vaccinated with the high-dose vaccine, yet could not receive it through pharmacies, is not surprising. The impact of the inconvenience to seniors during those seasons and thus possible residual impact on community pharmacy influenza services are unknown. Fortunately, the high-dose vaccine was available both through physician offices and community pharmacies for the 2020/2021 influenza season. 8
More females (n = 1,704,958) than males (1,404,869) were immunized in pharmacies. However, after adjusting for population size and age group, immunization rates were higher among older men than women (Table 3). Over time, the age- and sex-standardized rates of immunizations increased across Ontario, yet regional variation in rates persisted (animated GIF, available at www.cpjournal.ca). In the 2019/2020 season, as an example, the age- and sex-standardized immunization rates were higher in eastern areas compared to central densely populated areas, with the lowest rate of 54.3/1000 persons in the Central West region and the highest rate of 158.4/1000 persons in the Champlain region. Similar patterns were observed across all seasons.
Discussion
Over 3 million Ontarians have been immunized against influenza in community pharmacies, representing about 23% of the population aged 5 or more years. Community pharmacy–administered influenza vaccinations increased quickly over the first 3 years of the program, from 246,293 patients in 2012/2013 to 898,458 in 2014/2015, and over 1 million residents have been immunized for influenza in community pharmacies annually since the 2016/2017 season. The initial slow uptake during the first influenza season in Ontario likely relates to delays, as community pharmacies had to apply for and obtain access to publicly funded influenza vaccines, as well as undergo public health pharmacy inspections, and pharmacists required injections training.9,10 The increase in utilization over time is likely attributed to increased supply and demand. Over time, more pharmacies have started to advertise and offer the service, while fewer public health influenza clinics are being held and public perception of the benefit of influenza immunizations has improved.11-14
The Canadian national immunization coverage goal is 80% for high-risk groups, including adults aged 65 years or older and those aged 18 to 64 years with chronic medical conditions. 15 Although rates have increased over time, national immunization coverage estimates for adults aged 65 years still do not meet national targets. 16 Immunization rates are estimated to have increased in Canadian jurisdictions that permit pharmacist administration of influenza immunizations, providing encouraging evidence of the impact of community pharmacy immunization programs on public health.17,18
The 2020/2021 influenza immunization season began with many anticipating higher immunization rates, attributed to the ongoing COVID-19 pandemic that has radically changed health care delivery, perceived harms from viral infections and thus benefits of vaccination.19,20 Indeed, more vaccines were ordered in anticipation of increased demand. 8 Results from the COVID-19 Ontario Prescription Drug Utilization Tool show that the number of community pharmacy influenza immunizations in October 2020 was over 3 times higher than that in October 2019. 21 The PharmD curricula in Ontario include injection training and thus new pharmacy graduates are able to provide immunization services without additional training. In fact, trained pharmacy students contribute toward community immunization services during co-op work terms and clinical rotations. 22 The Canadian Pharmacists Association provided guidance to support 2020/2021 pharmacy immunization services with public health considerations related to the ongoing COVID-19 pandemic. 23 Still, there is a potential residual impact of the lack of high-dose vaccine availability and resultant decline in pharmacy immunizations among Ontario residents aged 65 years or older during the 2018/2019 to 2019/2020 immunization seasons. It will be interesting to see how the numbers and rates change in the 2020/2021 immunization season compared to prior years.
The recent ability for some pharmacies to test for COVID-19 and provide COVID-19 immunizations has put the spotlight on pharmacies as a hub for public health and health care service delivery.24-26 The OPEN Atlas of Community Pharmacy Influenza Immunizations tool may become instrumental for future public health resource planning in community pharmacies. The trends in Ontario may be helpful to provide guidance to other jurisdictions as they launch immunization programs and to inform health policy decision-making, for both seasonal influenza and COVID-19. We encourage other Canadian provinces and territories to consider building similar interactive atlas tools to help track public health services delivered in community pharmacies. ■
Supplemental Material
sj-gif-1-cph-10.1177_17151635211034207 – Supplemental material for The Ontario Pharmacy Evidence Network Atlas of Community Pharmacy Influenza Immunizations
Supplemental material, sj-gif-1-cph-10.1177_17151635211034207 for The Ontario Pharmacy Evidence Network Atlas of Community Pharmacy Influenza Immunizations by Maha Chaudhry, Nancy He, Nancy M. Waite, Sherilyn K. D. Houle, Jeffrey C. Kwong and Suzanne M. Cadarette in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Acknowledgements
Preliminary results were presented at the Ontario Pharmacy Evidence Network Summit in March 2019 and Pharmacy Experience Pharmacie conference in June 2019. The authors acknowledge Meagan Hatch for contributing to the summary of pharmacy influenza services across Canada.
Funding:
This research was supported by a grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC, ministry grant no. 6674) and the Leslie Dan Faculty of Pharmacy. This study was supported by ICES, which is funded by an annual grant from the MOHLTC. All analyses were completed at the ICES University of Toronto site, supported by the Leslie Dan Faculty of Pharmacy. Parts of this material are based on data and information compiled and provided by the MOHLTC, the Canadian Institute for Health Information (CIHI) and IQVIA Solutions Canada Inc. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. We thank IQVIA Solutions Canada Inc. for use of their Drug Information file.
Author Contributions:
All authors contributed to study design, interpreting study results, critical review of the manuscript and approved the final version submitted for publication. SMC was responsible for project funding, administration and staff/student supervision. NH completed analyses at ICES and MC prepared tables and figures.
Conflict of interest statement:
The authors report no conflicts of interest.
Ethical considerations:
ICES is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act. Section 45 authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects conducted under section 45, by definition, do not require review by a Research Ethics Board. This project was conducted under section 45 and approved by ICES’s Privacy and Legal Office.
Data availability:
The data set from this study is held securely in coded form at ICES. While data-sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() . In addition, the OPEN Atlas Interactive Tool will be made publicly available on a research website.
. In addition, the OPEN Atlas Interactive Tool will be made publicly available on a research website.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.