
Abstract

To the Editor:
Chronic hand dermatitis (CHD; or hand eczema) is a common debilitating skin condition with a profound negative impact on quality of life. CHD encompasses multiple clinical presentations with diverse and complex pathophysiology. 1 Prior studies have shown that Staphylococcus aureus (S. aureus) colonization is common on the hands of those with CHD and is associated with severity, especially in the atopic dermatitis (AD) subtype. 2 Though the exact role of S. aureus in CHD pathophysiology remains unclear, it has been hypothesized that S. aureus could contribute to increased inflammation and chronicity.2,3
Building on a previous open-label study (NCT05293717) on the clinical efficacy of topical 1.5% ruxolitinib (JAK1/JAK2 inhibitor) in CHD, 1 this analysis examines treatment-associated changes in S. aureus colonization. In this small, open-label study, 15 participants (18–75 years) with recalcitrant, moderate-to-severe CHD applied ruxolitinib 1.5% cream twice daily to the hands for 12 weeks. 1 Study visits occurred every 4 weeks, including a 4-week post-treatment follow-up at week 16. At each study visit, skin swabs were taken from a dorsal, non-lesional area (selected to reduce site variability), along with assessments of disease severity (ie, Hand Eczema Severity Index/HECSI) and itch (ItchyQuant, 4 self-report numeric rating scale for itch severity ranging from 0 to 10, with 10 the worst itch imaginable). S. aureus abundance was measured by TaqMan-based quantitative PCR of the chromosomally encoded, femA gene, reported as relative colony forming units (rCFU). Statistical analyses were done in Prism and used a 0.05 significance level, with data reported as medians and interquartile range (IQR). Limitations of this pilot include the small cohort and open-label approach.
Treatment with topical 1.5% ruxolitinib in CHD was associated with significant decreases in S. aureus burden, itch, and severity (n = 15, Friedman’s test, S. aureus: P = 0.0013; ItchyQuant: P = 0.0019; HESCI: P < 0.0001; Fig. 1). By week 12 of treatment, S. aureus burden was significantly reduced, and symptom assessments showed marked improvement from baseline. However, 4 weeks after treatment cessation (Week 16), all parameters exhibited a reversal: S. aureus burden, itch intensity, and HECSI scores increased (indicating worsening; Fig. 1). S. aureus burden and itch levels were no longer significantly different from baseline, while clinical severity remained partially improved (Fig. 1). Of note, as expected, a greater baseline S. aureus abundance was found in atopic (n = 7; 2,342 [122.6, 31,718]) versus non-atopic CHD (n = 8; 87.38 [38.43, 2,655] rCFU; P = 0.0205, Mann–Whitney test), with greater degree of changes in S. aureus burden noted in this group after treatment.
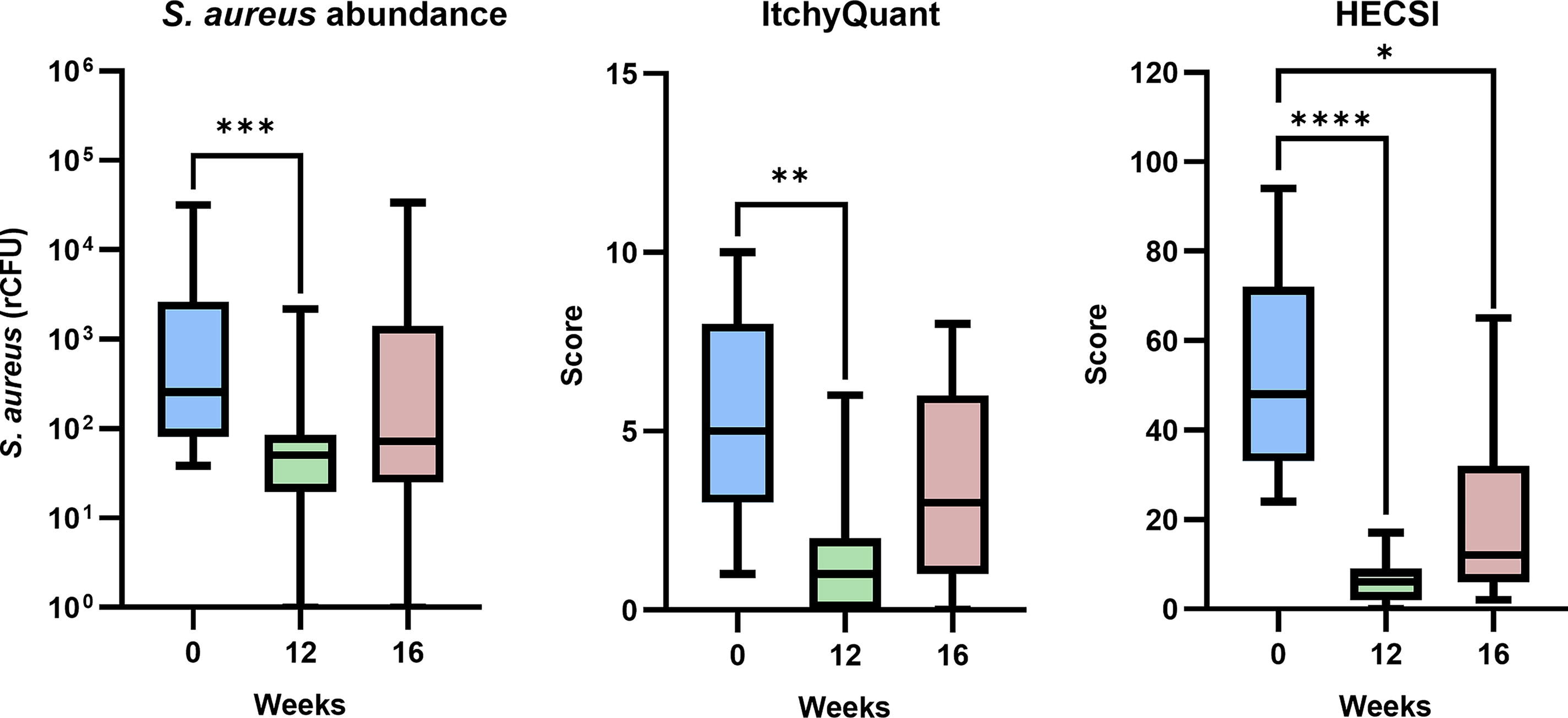
S. aureus burden, itch, and severity significantly improved after 12 weeks of treatment with topical 1.5% ruxolitinib, with trends toward worsening after treatment discontinuation for 4 weeks (16 week). S. aureus burden (rCFU), Dunn’s multiple comparison: week 0 versus week 12, P = 0.0008; week 0 versus week 16, P = 0.2037; week 12 versus week 16, P = 0.2037. ItchyQuant, Dunn’s multiple comparison: week 0 versus week 12, P = 0.0030; week 0 versus week 16, P = 0.5127; week 12 versus week 16, P = 0.1657. HECSI, Dunn’s multiple comparison: week 0 versus week 12, P < 0.0001; week 0 versus week 16, P = 0.0105; week 12 versus week 16, P = 0.2037; N = 15, *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001.
Consistent with prior studies, S. aureus was detected on non-lesional skin of individuals with moderate-to-severe CHD, with greater baseline burden in the AD subtype. For the first time, we report that topical ruxolitinib treatment in CHD is associated with significant reduction of S. aureus burden, in addition to clinical improvement. Further, a reversed trend was observed after stopping ruxolitinib for 4 weeks, with increased S. aureus burden and itch returning towards baseline values while severity assessment (HECSI) remained improved, possibly suggesting that off treatment, subclinical inflammation in CHD might allow for S. aureus (re)-colonization. Further studies are needed to investigate the underlying role of S. aureus in CHD and the direct or indirect (eg, inflammatory-mediated) mechanism of ruxolitinib.