
Abstract
Capsule Summary
Patients with sodium disulfite contact allergy more often report systemic symptoms to high-sulfite foods and beverages, especially wine and pickled products. Stronger patch test reactions were associated with greater reported symptom severity and frequency. Physicians should consider dietary counseling for select patients with sulfite contact allergy.
INTRODUCTION
Sulfites, including sodium disulfite and sodium metabisulfite, are well-established causes of allergic contact dermatitis (ACD) and received specific attention as the 2024 American Contact Dermatitis Society (ACDS) Allergen of the Year. 1 These compounds are widely used as preservatives in cosmetics, personal care products, and topical pharmaceuticals. Though relatively uncommon, sulfite contact allergy is often clinically relevant and has been shown to result from both personal product and occupational exposures. 2
Sulfites are also used as preservatives in food and beverages. High concentrations of sulfites are found in products such as wine, pickled foods, and condiments. Ingestion of sulfites has been associated with a range of systemic symptoms in sensitive individuals, a phenomenon often referred to as “sulfite intolerance.” Systemic symptoms reported in association with sulfite ingestion include respiratory symptoms, headaches, gastrointestinal distress, pruritus, urticaria, flushing, and angioedema.3,4 Controlled oral challenge studies have validated the symptom-provoking potential of sulfites, and one double-blinded study demonstrated dose-dependent headache development in susceptible patients.5,6
Although ACD and systemic sulfite intolerance have been individually documented, the potential relationship between the two remains unexplored. A retrospective case series by García-Gavín et al identified systemic symptom reports in 6 of 124 patients with positive patch tests to sodium metabisulfite, though documentation of noncutaneous symptoms was likely inconsistent. 7 A 1994 French study involving oral challenge and reintroduction testing found that 12 of 13 patch test-positive individuals were also diagnosed with sulfite intolerance. 8
The present study aims to address this gap by evaluating whether patients with positive patch test reactions to sodium disulfite report systemic symptoms after consuming high-sulfite foods, compared with a randomly selected group of sodium disulfite patch test-negative individuals. This work seeks to generate foundational data and inform clinical guidance for managing patients with contact allergy to sulfites.
METHODS
Study Design and Setting
This was a retrospective, observational, cross-sectional study conducted at the Park Nicollet Contact Dermatitis Clinic, a tertiary referral center in Minneapolis, MN, with an established patch test database of over 2000 patients. It was reviewed and approved by the HealthPartners Institutional Review Board (IRB# A24-284). All participants provided verbal informed consent and were compensated with a nominal gift card for completing a web-based survey.
Participants
Two study groups were identified:
Survey Instrument
Participants completed a standardized electronic questionnaire that assessed:
Occurrence of symptoms after ingestion of high-sulfite food or beverage triggers (eg, wine, dried fruits, grape juice, pickled foods). Type of systematic symptoms (eg, headache, gastrointestinal upset, respiratory symptoms, hives, or eczematous flares) after ingestion of high-sulfite foods or beverages. Frequency and severity (mild: no medicines/creams needed to control symptoms, moderate: medicines/creams needed to control symptoms, severe: emergency room/urgent care/other medical treatment needed to control symptoms) of symptom occurrence.
Survey data were collected and managed using Research Electronic Data Capture (REDCap). A copy of this survey is available in Supplementary Data. For sulfite-positive individuals, the strength of patch test reactions (borderline/doubtful [?], mild [1+], strong [2+], or very strong [3+]) was entered into REDCap by research coordinators alongside the survey responses.
Statistical Analysis
Participant responses were summarized overall and by sulfite patch test results. Among those reporting exposure to a given trigger, differences in symptom type and severity were assessed using Fisher’s exact tests. In participants with positive sulfite patch tests, associations between symptom presence/severity and strength of patch test reactions were similarly examined. Symptoms related to wine consumption were compared based on whether participants reported symptoms with all types of alcohol or only with alcohols known to contain sulfites. Given the exploratory nature of this study, analyses were not powered for hypothesis testing. P-values < 0.05 are reported as indicators of potentially meaningful differences but are not definitive. All analyses were conducted in R version 4.4.3.
RESULTS
Self-reported systemic symptoms after sulfite ingestion were significantly more common among patch-positive participants compared with controls (57.9% vs 26.8%, P = 0.005). The patch-positive group also reported symptoms to a greater number of individual food/beverage exposures with 23.7% of patch-positive patients reporting symptoms to over half of the high-sulfite foods they consume (Table 1, P = 0.001). Patch test-positive patients were more likely to report at least one trigger with moderate symptom severity, with 28.9% experiencing moderate symptoms compared with 12.2% of controls (P = 0.06).
Reported Symptoms Related to Consumption of High-Sulfite Items Compared Between Patients with Positive and Negative Patch Testing Results (N = 82)
All summary statistics are presented as n (%).
Percentages calculated with number of individuals reporting having consumed trigger as denominator.
P-values are from Fisher’s Exact tests comparing the two groups.
Wine was the most frequently reported trigger, with 58.1% of patch-positive participants reporting symptoms following consumption compared with 25.6% in the patch-negative group (P = 0.006). Other high-sulfite foods such as sauerkraut (20.9% vs 0%, P = 0.009) and grape juice (16.0% vs 0%, P = 0.023) showed differences in symptom provocation associated with patch test-positive compared with patch test-negative individuals.
Type and severity of symptoms are shown in Table 2. Headaches, flushing, and gastrointestinal symptoms were the most common symptoms across all foods and beverages investigated. There were no severe symptoms reported with the consumption of surveyed triggers. Across triggers, patch-positive patients were more likely to report avoiding consumption due to symptoms as compared with patch-negative patients.
Type and Severity of Symptoms Related to Consumption of High-Sulfite Items Compared Between Patients with Positive and Negative Patch Testing Results Who Reported Symptoms Related to Trigger (N = 33)
All summary statistics are presented as n (%); Percentages calculated with number of individuals reporting having symptoms related to trigger as denominator; Cells with “—” represent items with no eligible responses (eg, no participant in group reporting symptom).
Pos, positive patch test patients; Neg, negative patch test patients.
Exploration into symptoms related to alcohol consumption found that 77.8% of patch test-positive participants reported experiencing symptoms more than half the time or always when consuming wine as compared with 50.0% of the patch-negative group (Table 2). Among patch test-positive patients who reported symptoms associated with wine consumption (n = 18), 55.6% reported their symptoms only occurred when consuming wine and not with other alcohol consumption (Fig. 1). The other 8 (44.4%) reported at least one symptom that was triggered by wine and other high-sulfite alcohol (beer and/or cider) and no symptoms with liquor or other alcohols not associated with sulfite content.
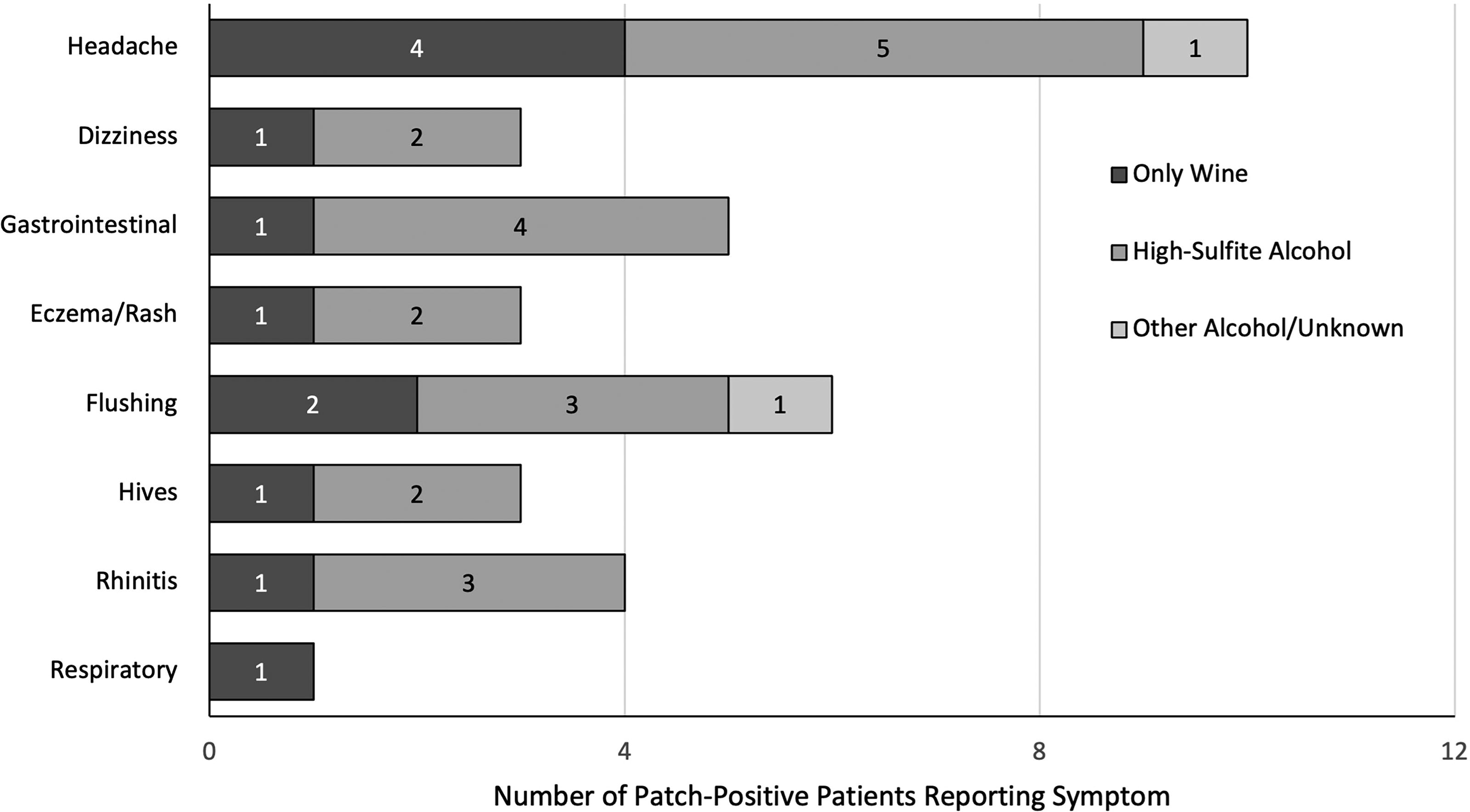
Reported symptoms related to alcohol consumption among patients with positive patch testing results who reported symptoms related to wine consumption (N = 18).
Among the patch test-positive group, stronger patch test reactions were associated with a higher likelihood and severity of symptoms. Of the patch-positive patients with strong or very strong reactions who had consumed at least one trigger (n = 11), 72.7% reported symptoms following sulfite ingestion (Fig. 2a). Similar positive correlations were observed between patch test strength and severity of symptoms (Fig. 2b).
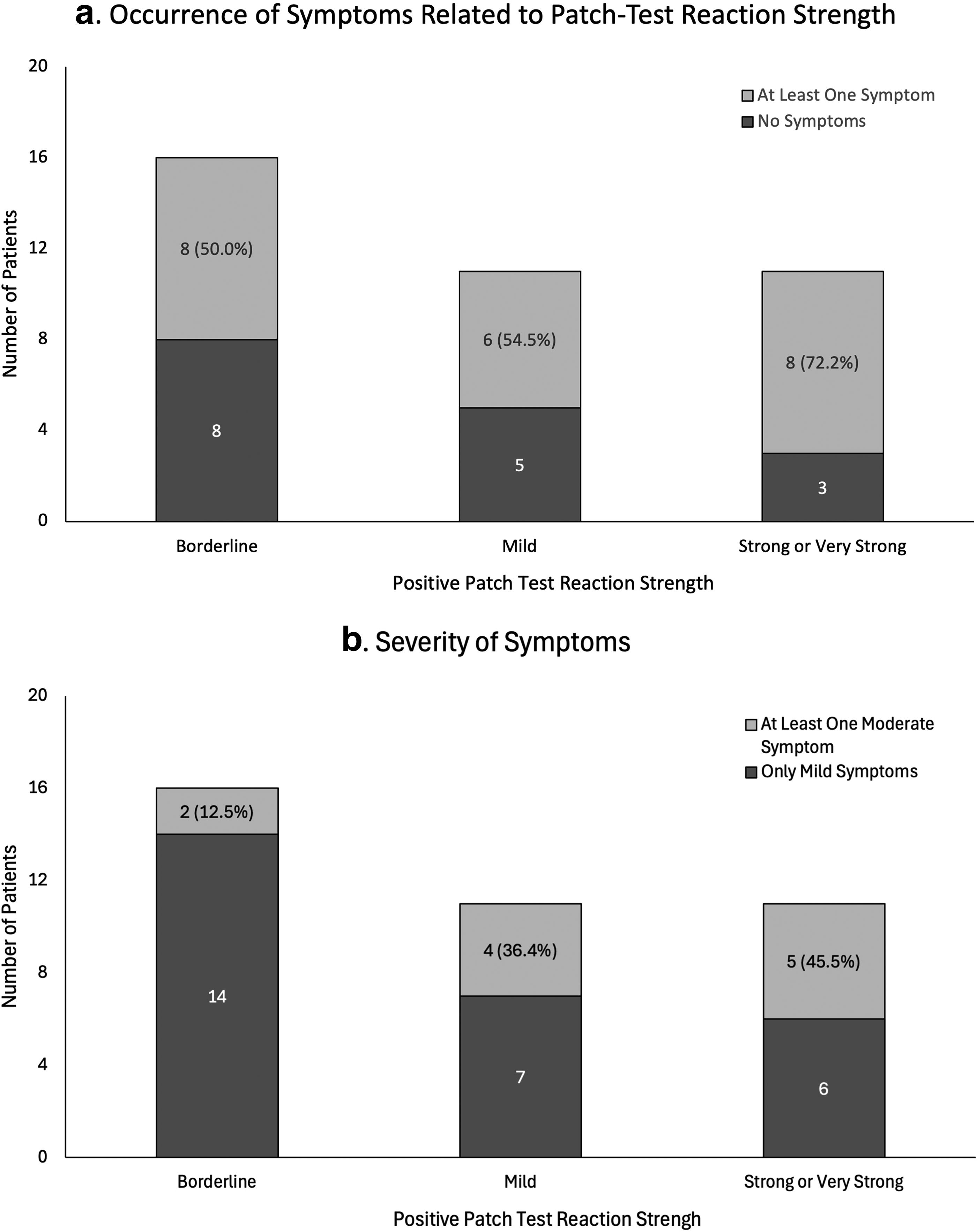
Reported symptoms
DISCUSSION
Main Findings
This study provides the first retrospective, controlled evaluation of systemic symptoms following sulfite ingestion reported in patients with confirmed contact allergy to sodium disulfite. Our findings demonstrate that individuals with positive patch tests were significantly more likely to report adverse reactions to high-sulfite foods and beverages, compared with patch test-negative controls. These associations were reflected not only in symptom frequency but also in the diversity of triggering foods and symptom severity. Although differences by patch test reaction strength did not reach statistical significance, a consistent trend emerged in which stronger patch test reactions were associated with increased symptom reporting.
Wine was the most common trigger. To differentiate between potential reactions to the sulfite content of wine and reactions attributable to its alcohol content, patients were asked about their symptoms to other alcoholic beverages. More than half of the patients who noted symptoms to wine reported these symptoms were specific to wine and did not occur with other alcoholic beverages. The remaining patients reported symptoms occurred with wine and beer or cider, alcohols also known to have sulfites, but not with liquor or other alcohols not associated with sulfite content.
Mechanistic Considerations
While type I hypersensitivity or nonimmunological processes have traditionally been implicated in sulfite intolerance, 9 our results raise the possibility that type IV-mediated processes—or overlapping nonimmunological pathways—may be related to symptom development in some individuals.
The biological plausibility of a relationship between systemic reactions and delayed-type hypersensitivity has precedence. A 2022 case report by Cussans et al described a patient with a strong positive patch test to sodium metabisulfite who developed recurrent, symmetrical intertriginous rashes after consuming a sulfite-rich diet. 10 Although oral challenge was declined, the clinical presentation was consistent with systemic allergic dermatitis, and the patient remained symptom-free after dietary sulfite avoidance. The authors concluded this was the first documented case of a type IV systemic allergic reaction to dietary sulfites.
Clinical Implications
Patients with confirmed contact allergy to sodium disulfite may benefit from education about dietary sulfite sources. Clinicians should consider advising these individuals on strategies such as food diaries or elimination trials if systemic symptoms are suspected. While avoidance of topical exposures remains standard, dietary counseling may be an appropriate adjunct for select patients.
Limitations
This study has several limitations. First, it relies on patient self-report of systemic symptoms, which introduces the potential for recall bias and subjective interpretation of symptom severity. Because no oral challenge testing was performed, it is not possible to confirm whether reported reactions were definitively caused by sulfites. Additionally, while the survey was distributed to both sulfite patch test-positive and negative patients, selection bias may exist if patients who experienced symptoms were more likely to respond. The study also does not account for other food sensitivities, dietary habits, or comorbidities that could influence symptoms. Finally, because our goal was to gather foundational data in an underexplored area, our analysis was not powered with the intention of detecting statistically significant differences between groups, and results should be interpreted as descriptive rather than inferential.
Future Directions
Future research is necessary to explore and further classify the phenomenon of systemic sulfite sensitivity. Further prospective studies with blinded oral challenge testing and larger sample sizes would be useful to more definitively establish any relationships between contact allergy to sulfites and systemic intolerance.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.