
Abstract
Capsule Summary
Prospective real-world study evaluating low-dose abrocitinib (100 mg once daily) in Chinese adults with moderate-to-severe atopic dermatitis. Demonstrated rapid, regionally consistent efficacy with a favorable safety profile. Identified baseline immunoglobulin E ≥100 IU/mL as a predictor of delayed early response, supporting potential for personalized treatment strategies.
INTRODUCTION
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease characterized by intense pruritus and eczematous lesions.1,2 The immunopathogenesis of AD is predominantly driven by type 2 (Th2) immune responses, such as IL-4, and IL-13. 3 However, the disease phenotype can vary acorss population. For instance, Asian patients often exhibit a mixed Th2/Th17 (and Th22) signature, with studies reporting significantly higher Th17/Th22 gene expression and lower Th1/interferon activity in Asian AD skin compared to Western patients.4-6 This blended immune profile may influence treatment responses and efficacy.
Recent therapeutic advances for moderate-to-severe AD include not only IL-4/13–blocking biologics but also oral Janus kinase (JAK) inhibitors.7,8 Abrocitinib is an oral, once-daily JAK1-selective inhibitor approved for treating moderate-to-severe AD. 9 Phase 3 trials and real-world evidence demonstrate that abrocitinib provides rapid and significant clinical improvement, including rapid pruritus relief within 2 weeks and clinical benefits for both treatment-naive patients and those non-responsive to existing systemic therapies.10B11 -14 Comparative studies have even shown that abrocitinib can produce faster pruritus reduction than the IL-4/13 inhibitor dupilumab, such as greater improvement in itch at Week 2 and higher Eczema Area and Severity Index 75% improvement (EASI-75) achievement at Week 4, highlighting its rapid onset of action.15,16
Abrocitinib is available in two approved dose levels (100 mg or 200 mg once daily). The 100 mg dose is typically used as the starting and maintenance regimen. In general, the higher 200 mg dose yields higher efficacy rates in trials, but adverse effects are also more frequent.8,9,17 For example, nausea was reported in only 4.2–9.0% of patients on 100 mg versus 11.1–20.1% on 200 mg, and acne occurred in up to 3.2% on 100 mg versus up to 6.6% on 200 mg. 18 These dose-dependent safety differences underscore the need to balance benefit and tolerability in clinical use. 19
Despite strong evidence from phase 3 trials, real-world data on abrocitinib are still limited. In particular, there is a paucity of reports focusing exclusively on the 100 mg dose. A recent Chinese single center prospective cohort (n = 117) found that 74.3% of moderate-to-severe AD patients achieved EASI-75 at week 12 of abrocitinib therapy. 16 However, this study included a mix of dosing regimens and even allowed dose escalation during treatment, making it impossible to isolate the performance of the 100 mg dose. Another real-world series (n = 51) compared low-dose abrocitinib to upadacitinib over 24 weeks but evaluated only overall efficacy and safety outcomes. 20 Notably, neither study examined clinical improvement by body region (eg, head/face vs trunk/extremities) nor investigated baseline biomarkers or clinical factors that might predict treatment response. Thus, gaps remain in our understanding of the long-term effectiveness, safety, and region-specific effects of 100 mg abrocitinib, as well as the predictors of good response.
This prospective study aims to address these gaps by evaluating the 12-week efficacy and safety of abrocitinib 100 mg daily in Chinese adults with moderate-to-severe AD, with extended follow-up to 24 weeks in a subset. By integrating longitudinal clinical outcomes and biomarker data, this study seeks to clarify the role of low-dose abrocitinib in AD management and identify clinical predictors of response to inform personalized treatment strategies for this underserved population.
METHODS
Study Design and Participants
This single-center, prospective, observational cohort study was conducted in a real-world setting at Sichuan Provincial People’s Hospital, China, from January 2024 to February 2025. A total of 40 adult patients aged 18–65 years with moderate-to-severe AD were enrolled. Diagnosis was confirmed using Hanifin & Rajka criteria, 21 with severity defined by a SCORing Atopic Dermatitis (SCORAD) index ≥25. Eligible participants had discontinued systemic immunosuppressants for at least 4 weeks and had not received JAK inhibitors, biologics (eg, IL-4/IL-13 inhibitors), or other targeted immunomodulators within 16 weeks prior to enrollment. Exclusion criteria included active infections (hepatitis, tuberculosis), malignancies, pregnancy, severe hepatic/renal dysfunction, or uncontrolled comorbidities.
All participants received oral abrocitinib 100 mg once daily (QD). During the first month, adjunctive therapies included calcineurin inhibitors (eg, tacrolimus/pimecrolimus) applied to sensitive areas (face/neck, vulva, axillae) and mild-to-moderate potency topical corticosteroids were used on other affected areas, both administered twice daily. After the first month, all topical therapies were discontinued per protocol unless clinically required; emollients were allowed for maintenance. Patients were evaluated at baseline, and at Weeks 2, 4, 12, and 24 (for those who completed treatment). The primary endpoints were efficacy and safety at Week 12, while secondary endpoints included sustained outcomes at Week 24.
This study was approved by the Ethics Committee of Sichuan Provincial People’s Hospital (No. 2023–383), and all participants provided written informed consent.
Clinical and Laboratory Assessments
Baseline demographic and clinical data included age, sex, BMI, disease duration, prior treatments for AD, atopic comorbidities, and lesion distribution patterns with specific focus on head/neck, hands/feet, and extensor/flexor surfaces of the extremities. Disease severity and treatment response were assessed using the SCORAD index, EASI, Investigator’s Global Assessment (IGA; 0–4 scale), and patient-reported outcomes, including the Peak Pruritus Numerical Rating Scale (PP-NRS), Atopic Dermatitis Control Tool (ADCT), Patient-Oriented Eczema Measure (POEM), and Dermatology Life Quality Index (DLQI).
Laboratory assessments included complete blood count, lipid panel, liver and renal function tests, hepatitis B/C serologies, and tuberculosis screening. Eosinophilia was defined as peripheral eosinophils ≥0.52 × 109/L, and elevated total IgE was defined as ≥100 IU/mL based on institutional reference ranges. All treatment-emergent adverse events (TEAEs) were documented and graded according to the Common Terminology Criteria for Adverse Events (v5.0). 22 Causality assessments were performed by blinded investigators.
Outcome Measures
The primary efficacy endpoints at Week 12 included the EASI-75 response rate (≥75% reduction in EASI score from baseline), IGA response rate (IGA ≤1 or ≥2-point improvement from baseline), and changes in EASI, SCORAD, and PP-NRS scores. Secondary endpoints included improvements in ADCT, POEM and DLQI, longitudinal changes in regional EASI subscores across anatomical regions (head/neck, trunk, upper/lower limbs) at Weeks 2, 4, and 12, and sustained efficacy outcomes at Week 24 for patients who completed treatment.
Statistical Analysis
Categorical variables were presented as frequencies (percentages), whereas continuous variables were reported as mean ± standard deviation or median (interquartile range, IQR), based on distribution assessed via the Shapiro–Wilk test. Longitudinal changes from baseline to Week 12 were evaluated using repeated-measures ANOVA with Bonferroni post hoc correction for parametric data, or Friedman tests with Dunn’s multiple comparisons adjustment for nonparametric data. To identify predictors of achieving EASI-75 at Weeks 2, 4, and 12, univariate logistic regression was first performed for each candidate predictor. Variables with P < 0.10 in univariate analysis or deemed clinically relevant were subsequently entered into multivariable logistic regression models. Multicollinearity was assessed using variance inflation factors (<5), and model fit was evaluated using residual diagnostics. Because enrollment was prospective and the final sample size could not be prespecified, multivariable analyses were considered exploratory and interpreted with caution. Primary inference was based on univariate analyses, while multivariable results are provided in Supplementary Appendix A1.
All statistical analyses were performed using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA). A two-sided P value <0.05 was considered statistically significant.
RESULTS
Baseline Demographics and Clinical Characteristics
A total of 40 patients with moderate-to-severe AD were enrolled, including 24 males (60.0%) with a mean age of 43.95 ± 15.16 years and mean BMI of 24.38 ± 3.04 kg/m2. The median disease duration was 2.00 years (IQR: 0.30–5.70 years). Comorbid atopic conditions were present in 45.0% (18/40), most commonly allergic rhinitis (40.0%), followed by asthma (5.0%) and urticaria (7.5%). Cardiovascular or metabolic comorbidities were identified in 9 patients (22.5%), including hypertension (n = 4), hyperuricemia (n = 3), and hyperlipidemia (n = 2). The median baseline EASI score was 21.18 (IQR: 15.18–26.40). Half of the patients (50.0%, n = 20) had a history of smoking, and 72.5% (n = 29) reported alcohol use; 19 patients reported both smoking and alcohol use, and most continued these habits prior to treatment initiation.
Lesion distribution revealed predominant involvement of the head and neck in 62.5% (25/40), palmar or plantar involvement in 20.0% (8/40), and isolated sole involvement in 5.0% (2/40). Among patients with limb lesions (n = 39), 17.9% (7/39) had both flexural and extensor involvement, while 82.1% (32/39) had isolated involvement of extensor areas without flexural involvement. Median baseline total serum IgE was 111.00 IU/mL (IQR: 34.50–323.00), and median eosinophil count was 0.12 × 109/L (IQR: 0.07–0.18).
Prior treatments included topical corticosteroids (80.0%), Tripterygium wilfordii (n = 3), dupilumab (n = 2), cyclosporine (n = 1), and tofacitinib (n = 1). At Week 24, 22 patients (55.0%) completed treatment; 13 (32.5%) remained on therapy but had not yet reached Week 24, and 5 (12.5%) discontinued after Week 12 due to satisfactory improvement (n = 3), financial burden (n = 1), or preference to avoid oral therapy (n = 1). Baseline characteristics are detailed in Table 1.
Demographics and Baseline Characteristics of the Patients with AD
Data are provided as mean ± standard deviation.
Data are provided as median [interquartile range].
AD, atopic dermatitis; EASI, Eczema Area and Severity Index; IgE, Immunoglobulin E; TEC, total eosinophil count.
Clinical Efficacy at Weeks 12 and 24
Significant improvements were observed in all clinical metrics—EASI, IGA, ADCT, PP-NRS, DLQI, POEM, and SCORAD—beginning at Week 2 and sustained through Week 12 (all P < 0.001; Fig. 1a–g). At Week 12, 60% (24/40) of patients achieved EASI-75, 42.5% (17/40) of patients achieved EASI-90, and 42.5% (17/40) met the IGA response criteria. The median EASI score was reduced by 90.77%. Other measures also showed substantial reductions: PP-NRS (−78.89%), ADCT (−76.47%), DLQI (−76.39%), and POEM (−81.82%).
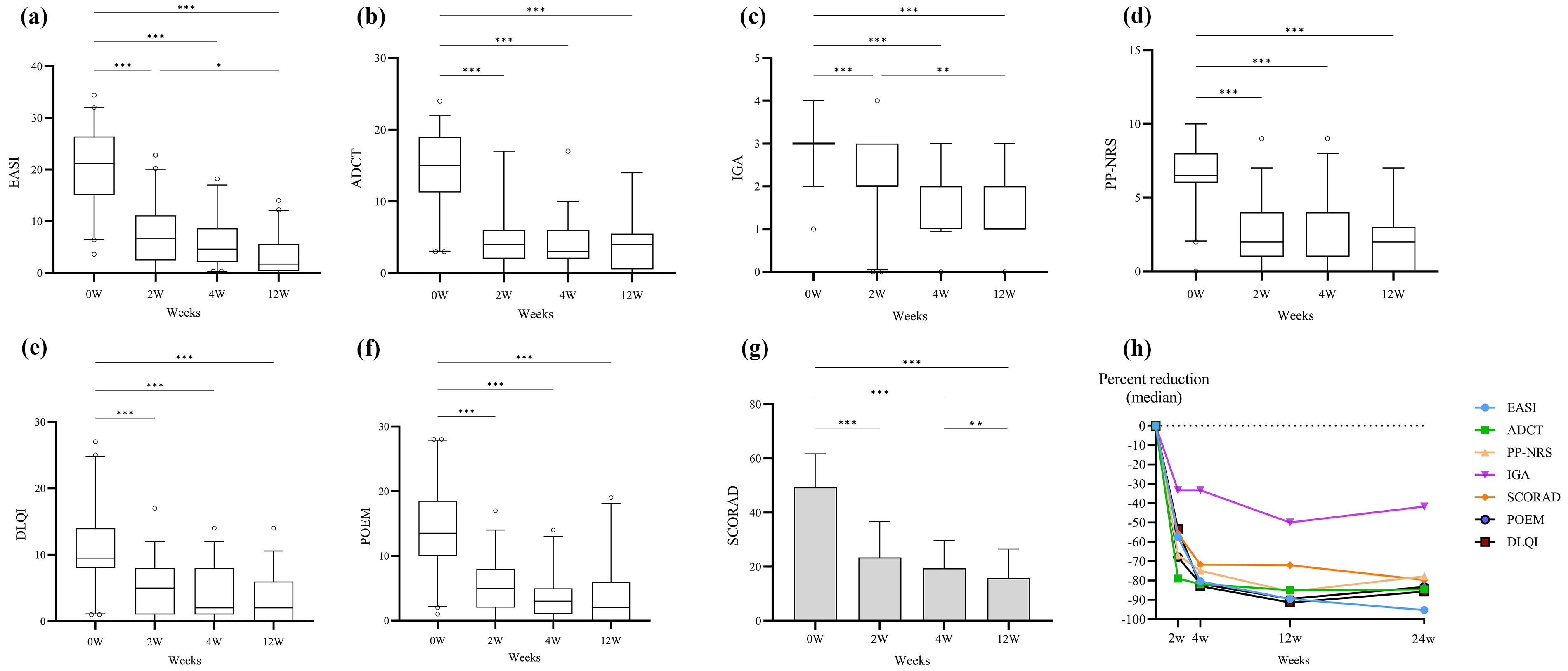
Changes in Clinical Scores and Percent Reduction from Baseline During 24-Week Abrocitinib Treatment. Eczema Area and Severity Index (EASI),
Among the 22 patients who completed 24 weeks of treatment, response rates remained consistent or improved. EASI-75 was achieved by 90.91% (20/22), EASI-90 was achieved by 68.18% (15/22), and the median EASI reduction reached 95.29%. The IGA response rate was 22.73%. SCORAD and ADCT scores continued to decline, while PP-NRS, POEM, and DLQI remained at similar levels. Notably, as topical therapy was stopped after Week 4, efficacy at Weeks 12 and 24 reflects abrocitinib 100 mg QD monotherapy (Fig. 1h).
Regional Efficacy Across Anatomical Sites
Among patients with regional lesions at baseline (n = 32 for head/neck; n = 28 trunk; n = 36 upper limbs; n = 20 lower limbs), EASI-75 rates increased over time. Head/neck lesions improved from 80.00% at Week 2 to 92.50% at Week 12, trunk from 72.50% to 85.00%, upper limbs from 67.50% to 82.05%, and lower limbs from 55.00% to 72.22%. Corresponding median percentage reductions in EASI subscores at Week 12 were: head/neck (−96.92%), trunk (−96.25%), upper limbs (−96.83%), and lower limbs (−68.99%) (Fig. 2a–b).
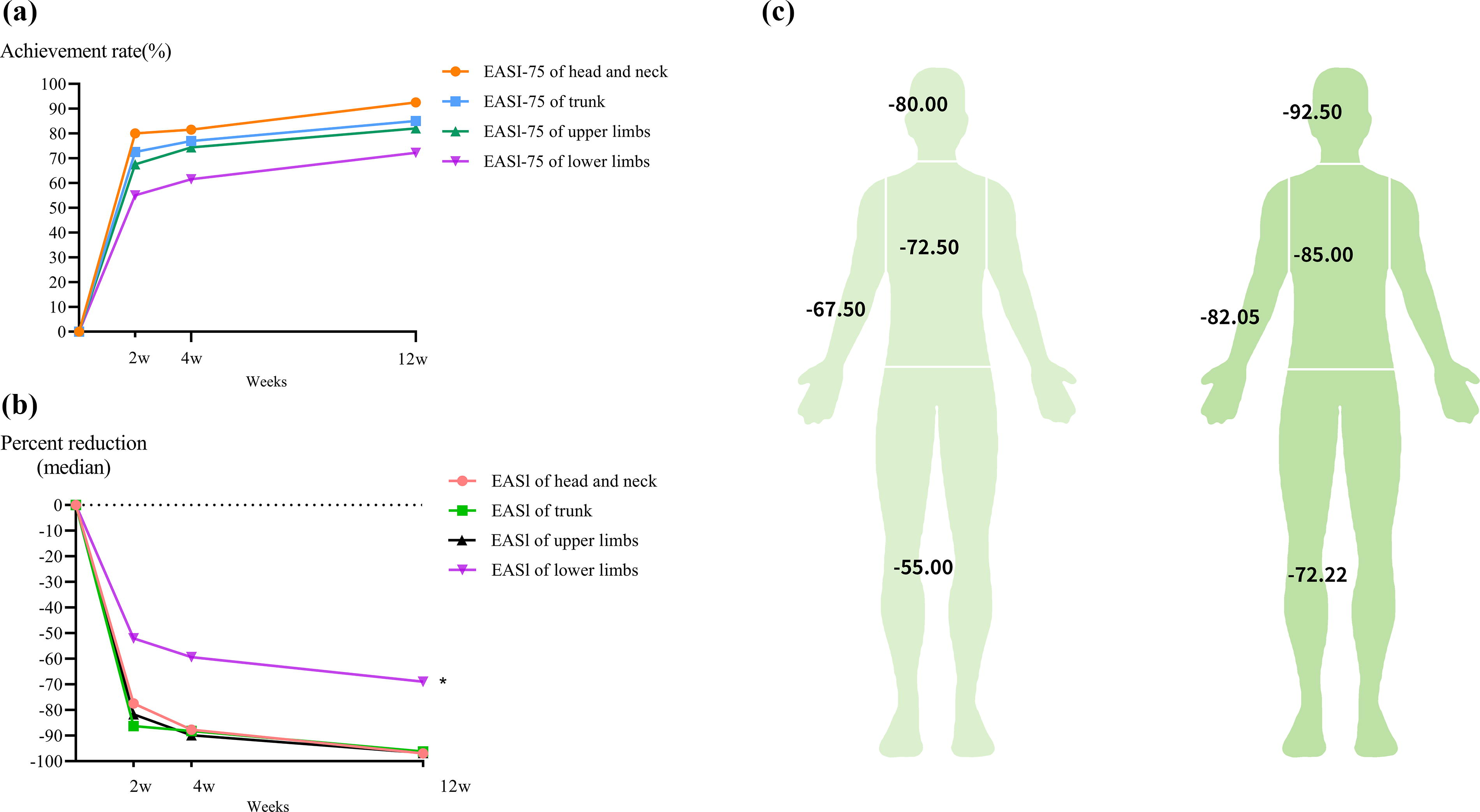
Anatomical Heterogeneity in EASI 75 Achievement and Score Reduction Across Body Regions.
Predictors of EASI-75 Response
In univariate logistic regression analysis, baseline total IgE ≥100 IU/mL was significantly associated with a lower likelihood of achieving EASI-75 at Week 2 (OR =0.20; 95% CI: 0.05–0.86; P = 0.030). Other candidate variables showed no statistically significant associations with EASI-75 at Weeks 2, 4, or 12 (Fig. 3). Concurrent involvement of both flexural and extensor areas at baseline showed a trend toward reduced Week 2 response (OR = 0.20; 95% CI: 0.03–1.20; P = 0.078), and age ≥45 years showed a trend toward higher Week 4 response (OR = 3.47; 95% CI: 0.90–13.31; P = 0.070). The “only extensor side” subgroup (n = 7) was excluded from comparative analyses owing to insufficient sample size relative to the flexural/extensor subgroup (n = 32).
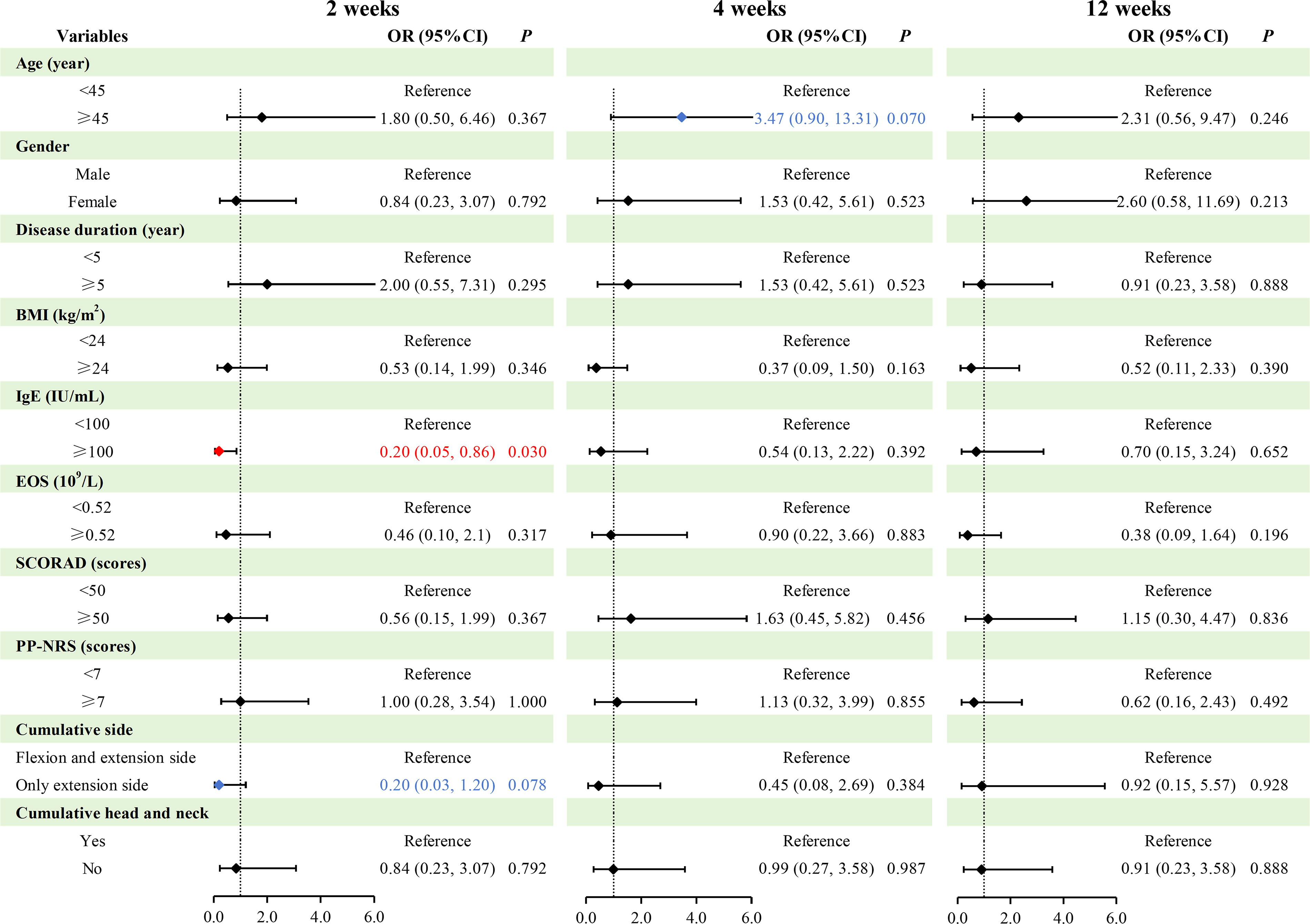
Univariate Logistic Regression Analysis of Factors Associated with EASI 75 Achievement across Observation Weeks. At Week 2, patients with atopic dermatitis (AD) and baseline total IgE ≥100 IU/mL was significantly associated with a lower likelihood of achieving EASI-75 (OR =0.20; 95% CI: 0.05–0.86; P = 0.030).No other candidate variables showed statistically significant associations at Weeks 2, 4, or 12.
Given the limited sample size (<10 events per variable), multivariable logistic regression was performed only as an exploratory analysis, including Ig E, age, and several clinically relevant variables (Supplementary Appendix A1). In this exploratory model, baseline total Ig E ≥100 IU/mL remained associated with lower odds of achieving EASI-75 at Week 2 (adjusted OR = 0.17; 95% CI: 0.03–0.99; P = 0.048) after adjustment for age, sex, BMI, and eosinophil count. At Week 4, age ≥45 years was associated with higher odds of response (adjusted OR = 4.97; 95% CI: 1.08–22.79; P = 0.039). No significant associations were observed at Week 12. These multivariable findings should be interpreted with caution due to the small sample size and are presented only to illustrate potential trends.
Safety and Adverse Events
All 40 patients were included in the Week 12 safety analysis, and 22 patients were followed through Week 24. A total of 13 TEAEs were reported. The most common were respiratory-related events (n = 5, 12.5%), including dry cough (n = 3) and upper respiratory tract infection (n = 2). Gastrointestinal AEs (n = 4, 10.0%) included constipation (n = 2), diarrhea (n = 1), and Helicobacter pylori-associated gastritis (n = 1). Additional TEAEs included dizziness (n = 2, 5.0%), herpes simplex (n = 1), and hypercholesterolemia (n = 1). Importantly, no major adverse cardiovascular events (MACE) were observed during the study period.
All TEAEs were graded as mild to moderate (Grade 1–2), and none led to treatment discontinuation. Except for the case of Helicobacter pylori-associated gastritis (deemed unrelated), all events were considered possibly related to abrocitinib. Notably, 92.3% of TEAEs occurred within the first 12 weeks, and no new events were reported during Weeks 12–24.
DISCUSSION
This prospective real-world study demonstrates that low-dose abrocitinib (100 mg QD) provides rapid and sustained clinical benefits in Chinese adults with moderate-to-severe AD, with a favorable safety profile. Significant reductions in EASI, SCORAD and pruritus scores were observed as early as Week 2, aligning with abrocitinib’s established rapid onset of action seen in phase 3 trials. 11 By Week 12, EASI-75 and EASI-90 response rates of 60% and 42.5%, respectively—modestly exceeding some trial data9B10 -12,17 and closely matching recent real-world reports from Asian cohorts.23-25 Notably, efficacy was sustained through Week 24, with EASI-75/EASI-90 rates rising to 90.91%/68.18% among completers, reinforcing the durability of response with prolonged therapy.13,14,26 These outcomes are particularly relevant given that prior real-world studies reporting higher efficacy evaluated mixed-dose regimens or permitted dose escalation, 16 whereas our cohort exclusively received the 100 mg dose.
The safety profile further supports the clinical utility of this low-dose regimen. All TEAEs were mild to moderate (Grades 1–2), predominantly respiratory and gastrointestinal in nature, consistent with abrocitinib’s known safety spectrum.9,18 Crucially, 92.3% of TEAEs occurred within the first 12 weeks, with no new events or discontinuations during extended exposure up to Week 24, underscoring the tolerability of long-term monotherapy. Importantly, in our cohort, 50.0% had a smoking history, 72.5% reported alcohol use, and nine had cardiometabolic comorbidities. Despite these baseline risks, no MACE occurred during follow-up. This observation is consistent with pooled global phase 2/3 trial data, where MACE incidence was low (0.18%) and comparable to placebo, 27 as well as with Chinese real-world studies—one evaluating 12 weeks of mixed abrocitinib 100 mg/200 mg use and another assessing 100 mg once daily for 24 weeks—both of which reported no MACE.16,20
A novel observation of this study lies in the anatomical heterogeneity of treatment response. An EASI-75 response in the head and neck region was observed in 80% of patients as early as Week 2, increasing to 92.5% by Week 12, suggesting rapid and near-complete lesion resolution in this traditionally difficult-to-treat area. This contrasts with slower or attenuated responses observed in the head/neck region in global phase 3 trials of abrocitinib 15 and other JAK inhibitors.28B29 -31 The superior regional efficacy observed in our cohort may be partly attributed to population-specific pharmacodynamic characteristics, as prior studies have reported faster and more robust responses to abrocitinib in Chinese patients with AD compared with those treated with dupilumab.16,24 The pathogenesis of AD in the head and neck region is associated with Th17 pathway activation, distinct microbial colonization, and unique local skin barrier characteristics,32,33 all of which contribute to greater therapeutic challenges. Given these complex immune drivers, our findings raise the possibility that abrocitinib may exert superior regional efficacy by modulating a broader array of inflammatory pathways—including IL-4, IL-13, IL-22, IFN-γ, and potentially non-Th2 cytokines34,35—thereby addressing the multifaceted nature of inflammation in this area.
In contrast, responses in the lower extremities were comparatively slower (EASI-75: 68.99% at Week 12), which is inconsistent with data on baricitinib and upadacitinib that reported higher response rates in lower limbs.29-31 Notably, no significant difference in treatment efficacy was observed between flexural and extensor surfaces, suggesting that regional therapeutic resistance may not be driven by glandular density or skin structure. Instead, factors such as mechanical friction, reduced lymphatic clearance, or site-specific immune milieus may contribute to attenuated responses in the lower limbs, warranting further investigation.
Our biomarker analysis identified baseline IgE ≥100 IU/mL as a predictor of delayed early response (Week 2 EASI-75 OR = 0.20, P = 0.030), aligning with evidence that elevated IgE impedes JAK inhibitor efficacy.31,36 IgE is a key antibody mediating type I hypersensitivity reactions. By binding to high-affinity receptors on mast cells and basophils, it triggers the release of inflammatory mediators and plays a pivotal role in the pathogenesis of atopic dermatitis. 37 Although no definitive correlation has been established between IgE levels and AD severity, it demonstrates predictive value for therapeutic response.38-40 Our findings imply IgE-mediated pathways may transiently resist initial JAK-STAT modulation.
Patients aged ≥45 years showed a trend toward higher Week 4 EASI-75 response, with statistical significance reached only in multivariable analysis, while univariate analysis showed a P value <0.1. Although limited by sample size, this observation aligns with prior studies: a Chinese real-world cohort reported higher 12-week EASI-90 rates in patients aged ≥60, 16 and post hoc analyses of abrocitinib trials found improved responses in patients aged 41–50 and ≥50 years. 41 Age-related immune changes may underlie these findings. Aging skin shows increased Th1 and Th17 markers and decreased Th2 and Th22 cytokines in patients with AD, 42 which could affect responsiveness to JAK inhibitors targeting these pathways. 43 However, further studies are needed to confirm these hypotheses.
Study limitations include the single-center design and modest sample size (n = 40), which may affect generalizability. The small sample size also constrained the stability and interpretability of multivariable logistic regression, particularly given the commonly cited requirement of at least 10 events per predictor variable. Nevertheless, the direction and magnitude of associations in the multivariable models were generally consistent with those observed in univariate analyses, lending support to the robustness of the primary findings. While 24-week follow-up provides valuable real-world insights, longer observation is essential for chronic AD management—particularly to track relapse in early discontinuators (n = 5). Recent findings suggest that abrocitinib may contribute to skin barrier restoration (eg, via filaggrin-2 upregulation) 44 and IgE reduction. 20 These potential effects suggest disease-modifying capabilities similar to those seen with biologics, 45 and may differentiate abrocitinib from other JAK inhibitors. Long-term studies are needed to confirm these observations. Future research is warranted to delineate the mechanistic basis of regional efficacy heterogeneity and to validate serum IgE and patient age as potential biomarkers for predicting the temporal dynamics of JAK inhibitor responses.
CONCLUSION
This real-world study demonstrates that low-dose abrocitinib is both effective and well-tolerated in Chinese adults with moderate-to-severe atopic dermatitis. The consistent improvement observed across anatomical regions—including the traditionally challenging head and neck area—combined with preliminary biomarker findings, underscores its therapeutic value and potential for personalized treatment. These results support the use of low-dose abrocitinib as a safe and effective long-term option in routine clinical practice, while highlighting the necessity for further research to elucidate region-specific mechanisms and validate predictive factors of treatment response.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.