
Abstract
Background
Anatomical variations of origin of the internal carotid artery (ICA) are very uncommon and may pose a diagnostic and therapeutic challenge.
Objective
We report a case of direct origin of the right ICA from the innominate artery (aplasia of common carotid artery) and a case of duplication of right ICA in healthy patients who performed duplex ultrasound (DUS) for primary cardiovascular prevention screening.
Methods
In both cases, the ultrasound scan was performed both in a transverse plane and on the longitudinal axis, and in one of the two cases, a computed tomography angiography was performed to confirm the diagnosis. A review of the current literature about anatomical variations of origin of carotid arteries was also performed.
Results
The most frequent congenital anomaly is represented by the aplasia of the CCA, followed by the agenesis and by the duplication of the ICA. In most cases, the anomaly is discovered occasionally and symptoms are aspecific. Diagnosis is usually confirmed through a multimodality imaging approach, including DUS of extracranial carotid arteries, magnetic resonance imaging (MRI), and computed tomographic angiography. In most cases, treatment was conservative, with pharmacological therapy aimed at the symptoms.
Conclusion
The recognition of such variations is mandatory, particularly when the patient needs a surgical treatment that may involve the vessel with the anatomical variations.
Introduction
Duplex ultrasound (DUS) has become the mainstay for the first level imaging diagnosis of atherosclerotic disease of the supra-aortic trunks. 1
Indeed, DUS can provide important information about the morphology and the flow of the supra-aortic trunks, especially when lesions are detected and surgical treatment is indicated.
In such cases, anatomical variations of origin of the internal carotid artery (ICA) may pose a diagnostic and therapeutic challenge.
The ICA usually arise from the common carotid arteries (CCA) on both sides, but while the left CCA originates directly from the aortic arch, on the right side the CCA originates from the brachiocephalic trunk (or innominate artery). Then, the CCA bifurcates into the external carotid artery (ECA) and ICA at the level of the superior border of the thyroid cartilage. The ICA, after a vertical course upward, enters the skull via the carotid foramen of the temporal bone.
In rare cases, the ICA may not originate from the CCA at its normal site. Even though those anatomical variation of origins are uncommon, they should be properly recognized.
The aim of this paper is to report a case of direct origin of the right ICA from the innominate artery in a 61-year-old male and a case about a duplication of right ICA in a 53-years-old female. Both performed a DUS as part of a primary cardiovascular prevention screening, for which both patients gave their consent to the anonymous publication of the case. The rarity of the described conditions challenged the team to search for relevant examples in the existing scientific literature in order to discuss the phenomena in a broader sense. Thus, a systemic review of the current literature about anatomical variations of origin of carotid arteries was also performed according to the PRISMA methodology.
Case report 1
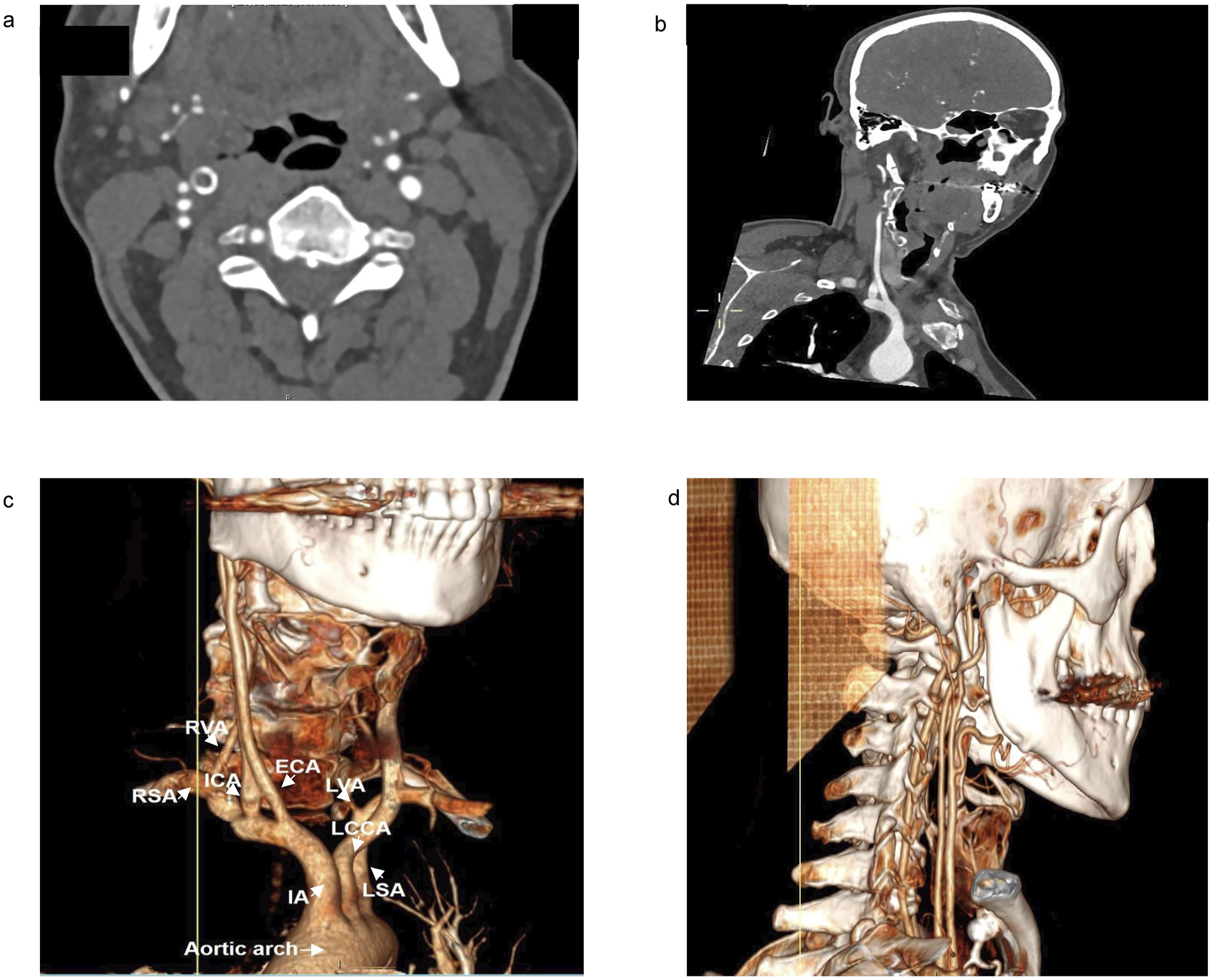
A 61-year-old man was evaluated at our hospital as part of a screening. His medical history was unremarkable and the patient was asymptomatic. During the visit, a DUS of the carotid arteries was performed. On the left side, ICA and External Carotid Artery (ECA) originated from the CCA and a small homogeneous hypoechoic plaque (20%) of the ICA was seen. On the right side, instead of CCA we found two parallel arterial vessels (Figure 1(a)) from the base of the neck and throughout the explorable tract: one of the vessels showed a monophasic low-resistance flow which identifies that vessel as the ICA (Figure 1(b)); the other one showed triphasic high-resistance flow which identifies that vessel as the ECA (Figure 1(c)). A third arterial vessel, with the same triphasic high-resistance flow, was suggestive of the Superior Thyroid Artery (Figure 1(d)). None of these three vessels had plaques. The patient accepted to undergo a contrast enhanced CT scan for a better evaluation of the anatomy of the carotid arteries from their origin at the level of the aortic arch. The CT scan showed aplasia of the CCA on the right side, while the left carotid artery had a normal anatomy. Right ICA and right ECA originated directly from the Brachiocephalic Trunk (Figure 2). Since the patient was asymptomatic, a conservative treatment and regular follow-up was suggested to the patient, particularly for the non-stenotic plaque on the left ICA. Representative DUS images of CCA agenesis: 1a: two parallel arterial vessels from the base of the neck and throughout the explorable tract; 1b: pulsed Doppler showed a monophasic low-resistance flow which identifies that vessel as the ICA; 1c: pulsed Doppler showed triphasic high-resistance flow which identifies that vessel as the ECA; 1d: a third arterial vessel, with the same high-resistance triphasic flow on pulsed Doppler, was suggestive of the superior thyroid artery. Representative TC images of CCA agenesis: 1a/b: Transverse and longitudinal images of CCA agenesis; 1c/d: 3D reconstruction of CT images of CCA agenesis, revealing the origin of right ICA and right ECA directly from the IA and their parallel course.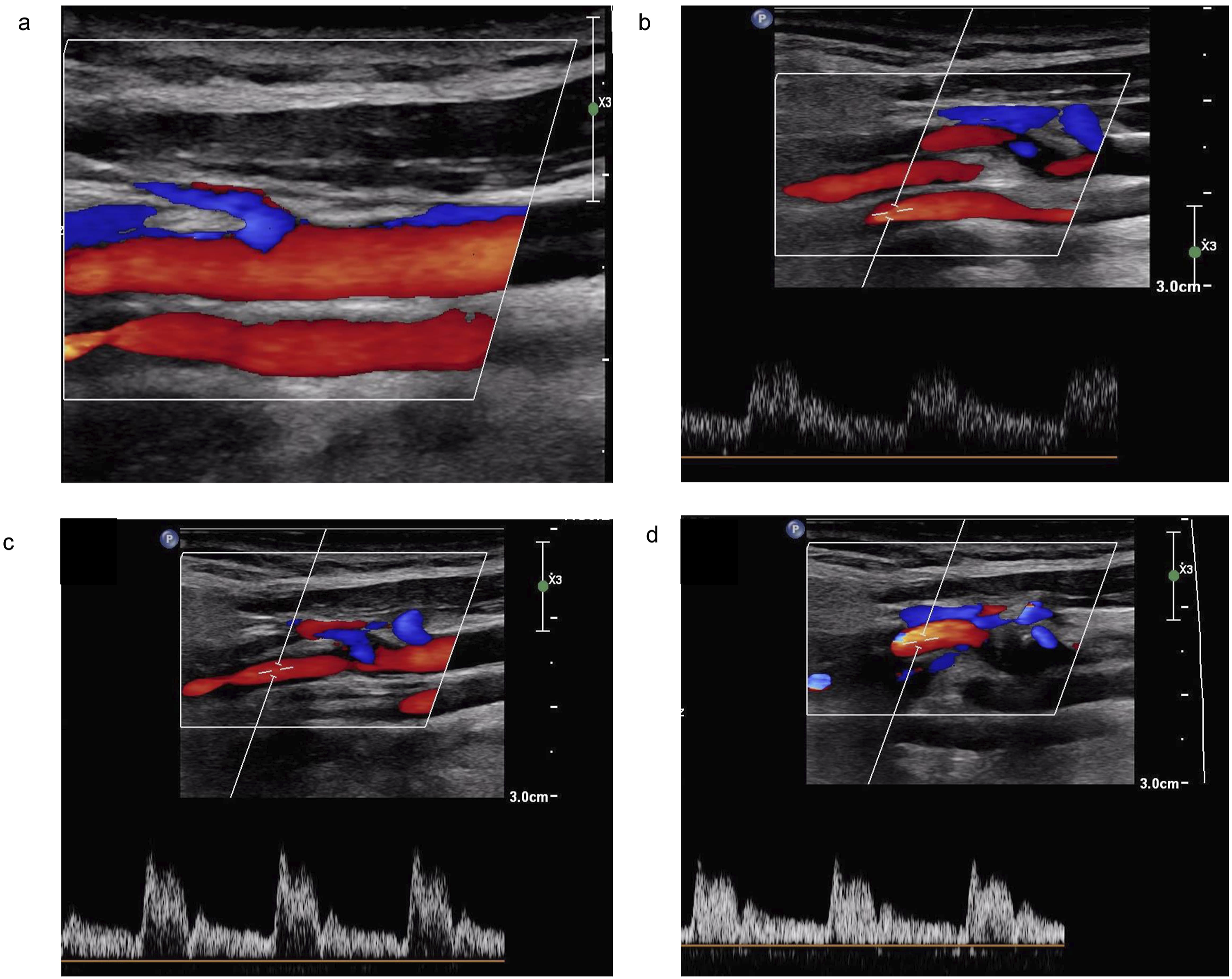
Case report 2
A 52-year-old woman without previous cardiovascular events was evaluated at our hospital as part of a screening. The patient was asymptomatic. During the visit, she underwent a DUS of the carotid arteries. On the left side, left ICA and left ECA originated from the left CCA. On the right side, we observed two vessels originating from the right CCA, both with monophasic low-resistance flow, suggesting the presence of two ICA (Figure 3(a)–(c)). Tilting the probe, a third vessel with a triphasic high-resistance flow was seen, deposing for the ECA (Figure 3(d)). On a transverse projection, we found three arterial vessels, one close to the other (Figure 3(e)). Since it was clear that there was a duplication of the right ICA, we decided to defer to further investigations. The patient was sent home with conservative treatment. Representative DUS images of ICA duplication: 3 a/b/c: two vessels originating from the right CCA, both with monophasic low-resistance flow, suggesting the presence of two ICA; 3d: a third vessel with a triphasic high-resistance flow was suggestive of the ECA; 3e: transverse projection were we saw three vessels (two ICA and one ECA), one close to the other.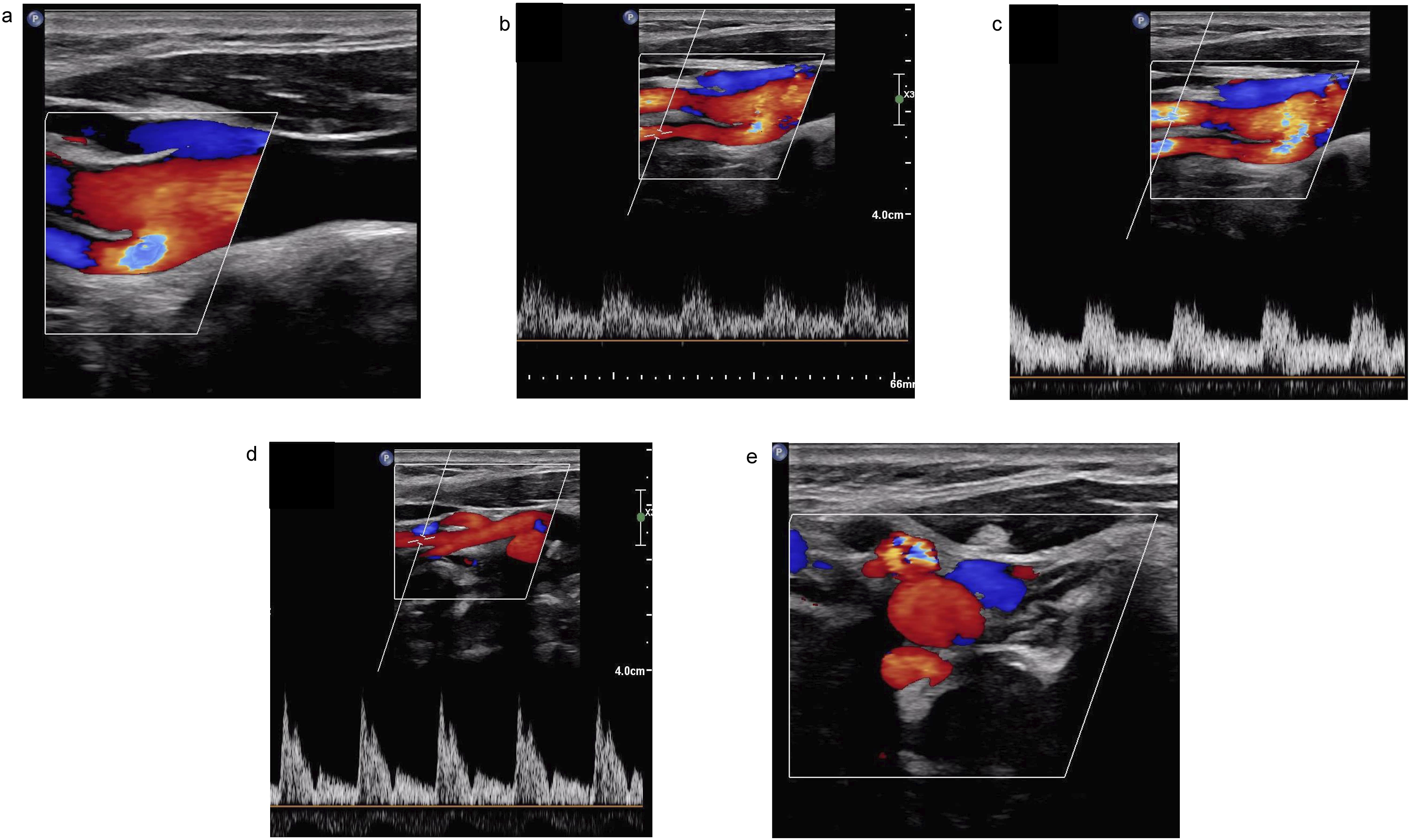
Discussion and literature review
A literature search was performed on Pubmed on February 2nd, 2024, with the words “internal carotid artery origin” and “duplication of internal carotid artery.” As shown through the Prisma Flow Diagram
2
(Figure 4), a total of 2428 papers were found through database searching and 7 papers were identified through other sources. After duplicates were removed, we screened a total of 2424 papers of whom 2331 were removed by title. Full-text articles assessed for eligibility were 93, of which 7 were excluded after reading the text, 2 articles were not retrieved and 1 article was not in English. We found 83 articles reporting cases about anatomical variation of the origin of the ICA or about duplication of the ICA. Although it was not possible to identify all the articles (two articles were not found), the remaining ones cover a time period ranging from 1977 to 2023. Prisma Flow Diagram of our systematic review. The total number of articles included in the review and the total number of excluded articles are described.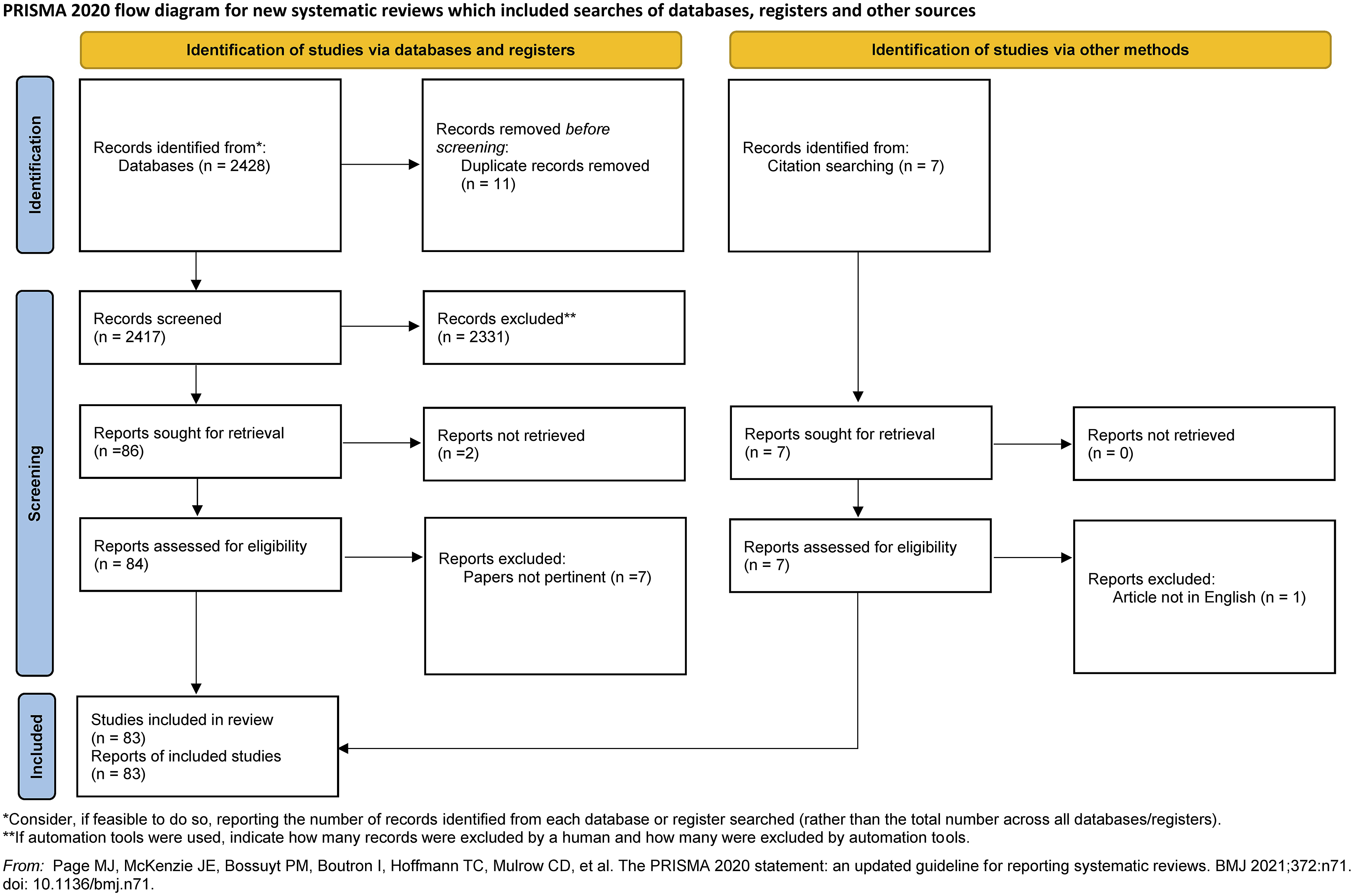
A total of 238 patients with anatomical variant of origin of ICA were identified in the literature. Patients were basically equally distributed by sex, being female patients 50.4% (male = 38.2%, unknown =11.4%). The patient’s age ranged from few months to 92 years.
Overall description of selected papers based on anatomical variant.
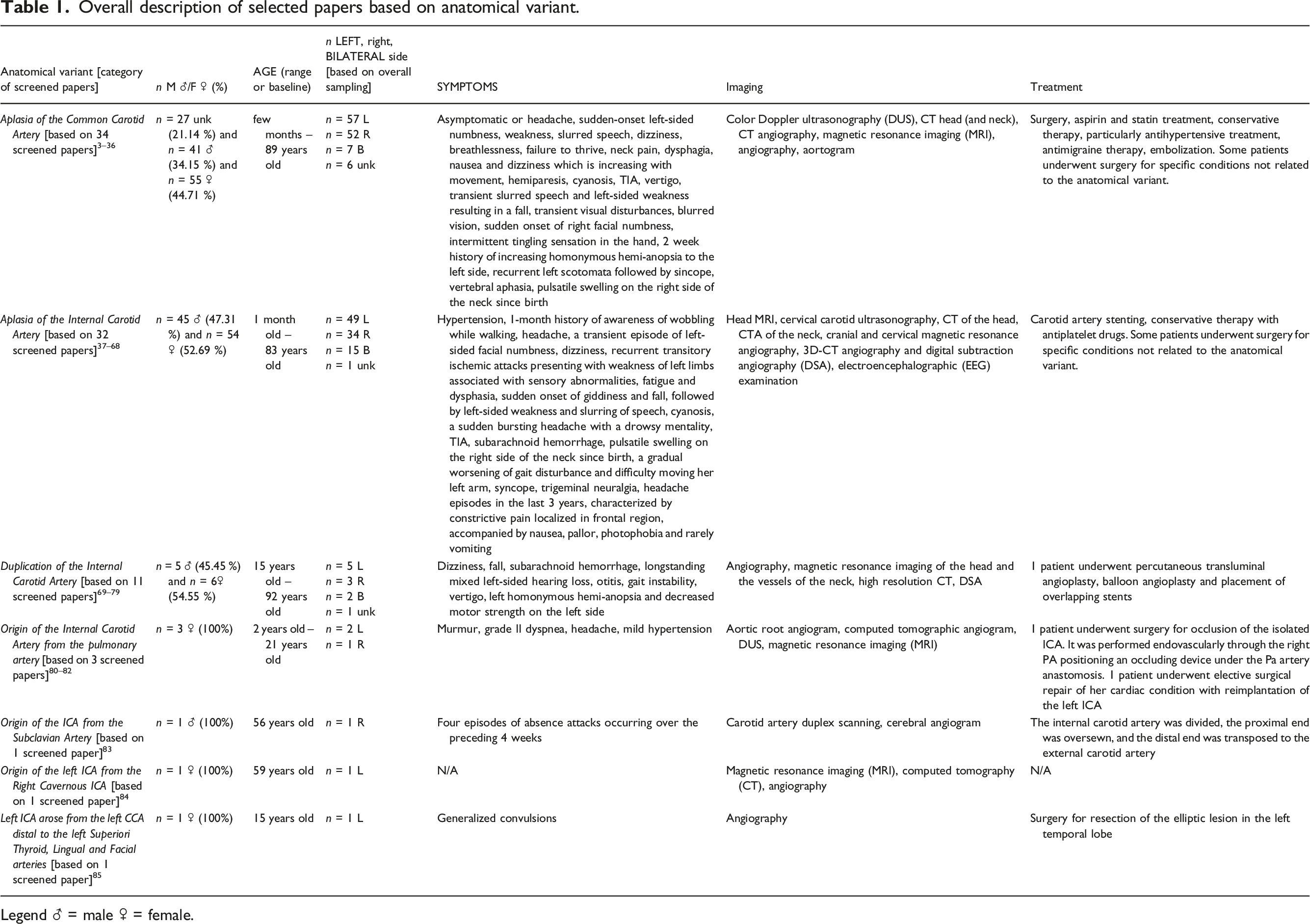
Legend ♂ = male ♀ = female.
In most cases, the anomaly is discovered occasionally. Clinical symptoms, in fact, are aspecific (i.e., dizziness, vertigo, hearing loss, gait instability, etc.). They often are not related to the anomaly and vary among patients but sometimes they are the reason for the primary examination. Drazin and Coll, for example, reported a case of a 41-year-old female who performed a Computed Tomography Angiography (CTA) for sudden headache, revealing the presence of a ruptured anterior communicating artery aneurysm, along with the agenesis of the CCA. 26
Diagnosis is usually confirmed through a multimodality imaging approach, including duplex sonography of extracranial carotid arteries, magnetic resonance imaging (MRI) and computed tomographic angiography. In most cases, treatment was conservative, with pharmacological therapy aimed at the symptoms.
When the vascular anomaly is diagnosed occasionally, usually no medical treatment nor surveillance is needed in the long-term, neither there is the need to perform any other diagnostic assessment to investigate about possible concomitant cardiovascular abnormalities.
On the other side, when the associated pathology requires surgical treatment, dealing with the concomitant abnormal origin of the ICA can be challenging in some cases. Idhrees and Coll 78 reported a case of a 21-year-old female who presented with grade II dyspnea due to the presence of an intracranial arteriovenous malformation with retrograde filling of a left ICA draining into the left pulmonary artery in tetralogy of Fallot. The patient underwent elective surgical repair of her cardiac condition with reimplantation of the left ICA to the left external carotid artery, which arose directly from the aortic arch, and was disconnected from the left pulmonary artery.
The patients reported in our case were both asymptomatic and did not require any surgical treatment, since the anomaly of origin of the ICA was discovered in both cases with a DUS that was performed for cardiovascular screening. In one case, DUS was enough for the diagnosis of anatomical variant of origin of ICA, but in the other case we decided to perform a CTA for a better understanding of the ultrasonographic finding. Interestingly both variants in our cases were found on the right side, even though according to the literature most variants are more frequent on the left side (Table 1).
From the surgical point of view, it is important to bear in mind the existence of such anatomical variant, especially when treatment is required and involves that vessel. Failure to recognize these variations may lead to incorrect diagnostic conclusions but also to possible intraoperative complications that may threaten cerebral vascularization.
Conclusions
Anatomical variations of origin of carotid arteries are rare. Among them, the most frequently reported in the literature are the aplasia of the common carotid artery, followed by the agenesis of the ICA and the duplication of the ICA. The recognition of such variations can pose a diagnostic challenge but is crucial when the patient needs a surgical treatment that may involve the vessel with the anatomical variant.
Footnotes
Author contributions
LR: data collection, data analysis, writing, critical revision
DM: conceptualization, data analysis, writing, critical revision
KT: data collection, critical revision
MBT: data analysis, critical revision
GC: critical revision
GN: critical revision
LM: critical revision
SC: data collection, writing, critical revision
All the Authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by in part by the Italian Ministry of Health.