
Abstract
Objectives
Limited knowledge exists regarding access site complication rates between trans-axillary and trans-brachial approaches with sheath sizes ≥6Fr. We retrospectively reviewed our institution experience with access site complications for percutaneous trans-axillary and trans-brachial arterial interventions using sheath sizes ranging from 6Fr to 10Fr.
Methods
We examined 67 endovascular interventions performed over 18 months, restricted to sheath sizes of 6Fr to 10Fr. Procedures utilizing trans-brachial (41 cases) and trans-axillary (26 cases) approaches under sonographic guidance were included. Cases involving hemodialysis accesses and those requiring surgical cut-down were excluded. The primary outcome measure was the occurrence of major access site complications (SIR grade-II/III) within 30 days, with data collected on hemostasis method, sheath size, and complications. Statistical analysis involved ANCOVA and Fisher’s exact tests, with significance set at p < .05.
Results
Successful percutaneous arterial access was achieved in all cases using either approach (trans-axillary or trans-brachial). Closure devices were employed in all axillary punctures and in 71% of brachial punctures. Major access site complications occurred in 7 out of 41 cases (17%) in the trans-brachial group and in 4 out of 26 cases (15%) in the trans-axillary group. However, there was no statistically significant difference in complication rates between the two groups, regardless of access site or sheath size.
Conclusion
Trans-axillary access serves as a safe and effective upper limb access method for percutaneous endovascular procedures requiring sheath size of 7Fr or larger when compared to trans-brachial approach.
Keywords
Introduction
Several endovascular interventions require intermediate to large-bore-sheath device delivery, which necessitate a vessel diameter of at least 5 mm. When the common femoral artery or target vessel angulation is unfavorable, the axillary or the brachial artery can provide an important upper limb alternative access site.1–12
The axillary artery was the first upper extremity artery to be used for angiography nearly 40 years ago, given its comparable caliber to femoral artery and lack of significant calcification. It fell out of favor as compared to transfemoral access, 7 primarily due to inadequate hemostasis resulting in hematoma, sometimes with local mass effect on critical regional structures such as the brachial plexus.3,4,7
The brachial artery is an alternative upper extremity access site; however, it is primarily limited by relative small caliber compared to femoral or axillary arteries, and its increased incidence of complications when ≥6Fr access sheath is used even when rescued by closure devices.5–7,13 Therefore, the axillary artery is once again being considered as a potential location for routine intermediate to large-bore access when the femoral approach is unfavorable.2,8–12,14–16 Advancements in closure devices and easy accessibility to ultrasound guidance offer a great opportunity for this vessel to become an alternative vascular access site in the modern era; however, limited knowledge exist regarding comparison of access site complication of trans-axillary and trans-brachial artery interventions when ≥6Fr access sheath is used especially when closure devices are utilized.2,9–12
The purpose of the present study, therefore, is to retrospectively review our institution’s experience with percutaneous trans-axillary and trans-brachial access site complications when using access sheaths larger than 5Fr (6Fr to 10Fr). As such, establishing which artery is less prone to these complications may help to guide decision-making and risk reduction in future treatments, when requiring access sheath sizes 6Fr to 10Fr.
Materials and methods
Patients
This retrospective study was approved by the institutional research ethics board. All patients who underwent percutaneous axillary artery or brachial artery access for endovascular interventions at our institution, between January 1, 2020, and July 1, 2021, were recruited for the study. Indications were primarily for critical limb ischemia (CLI), claudication, visceral stenting, endovascular aneurysm repair (EVAR) revisions, and embolization. During the data collection period, access site was chosen based on target vessel in the individual case and operator preference. We excluded cases where sheath sizes <6Fr or >10Fr were used; cases related to arteriovenous fistulae or grafts for hemodialysis; and cases requiring vascular access through surgical cut-down approach.
Techniques
Access
Endovascular interventions are typically performed under moderate sedation with intravenous fentanyl and midazolam (Sandoz, Boucherville, Quebec, Canada) administered by a registered nurse and titrated to effect. The skin overlying the puncture site is cleaned with chlorhexidine or povidone solution and draped in typical sterile fashion. The subcutaneous tissues overlying the puncture site are infiltrated with 1% lidocaine (Alveda Pharmaceuticals, Toronto, Ontario, Canada). All patients received intravenous or intraarterial heparin.
Percutaneous access was then obtained according to a modified Seldinger technique. Ultrasound guidance was performed using high frequency linear probes. Brachial artery access was done typically following published approach. 17 Briefly, the distal arm is examined with ultrasound to identify the lower brachial artery just proximal to the antecubital fossa at an area where the vessel is more superficial and can be compressed against the humerus. Following local anesthetic (5–10 mL of 1% lidocaine), a single-wall puncture needle is used to access the artery under ultrasound guidance followed by placement of appropriately sized sheath.
Axillary artery access is obtained following published approach.
18
Briefly, the anterior chest wall is sonographically examined near the intersection of the pectoral muscles and the anterior deltoid. A suitable location for puncture is chosen within the deltopectoral groove, taking care to avoid the brachial plexus when possible. Typically, the junction of the second and third segment, where the axillary artery is more superficial as it moves lateral to the pectoralis minor muscle is chosen as the optimal location (Figure 1). Percutaneous access technique of axillary artery. (a) Axial CT with arm by side. Arrow indicates direction of puncture, arrowhead points to the pectoralis minor muscle. Occasionally, the access traverses the pectoralis minor. (b) Coronal reconstruction. White line showing the location of access and arrowhead points to first rib. On fluoroscopy, the access is usually located just lateral to the first rib.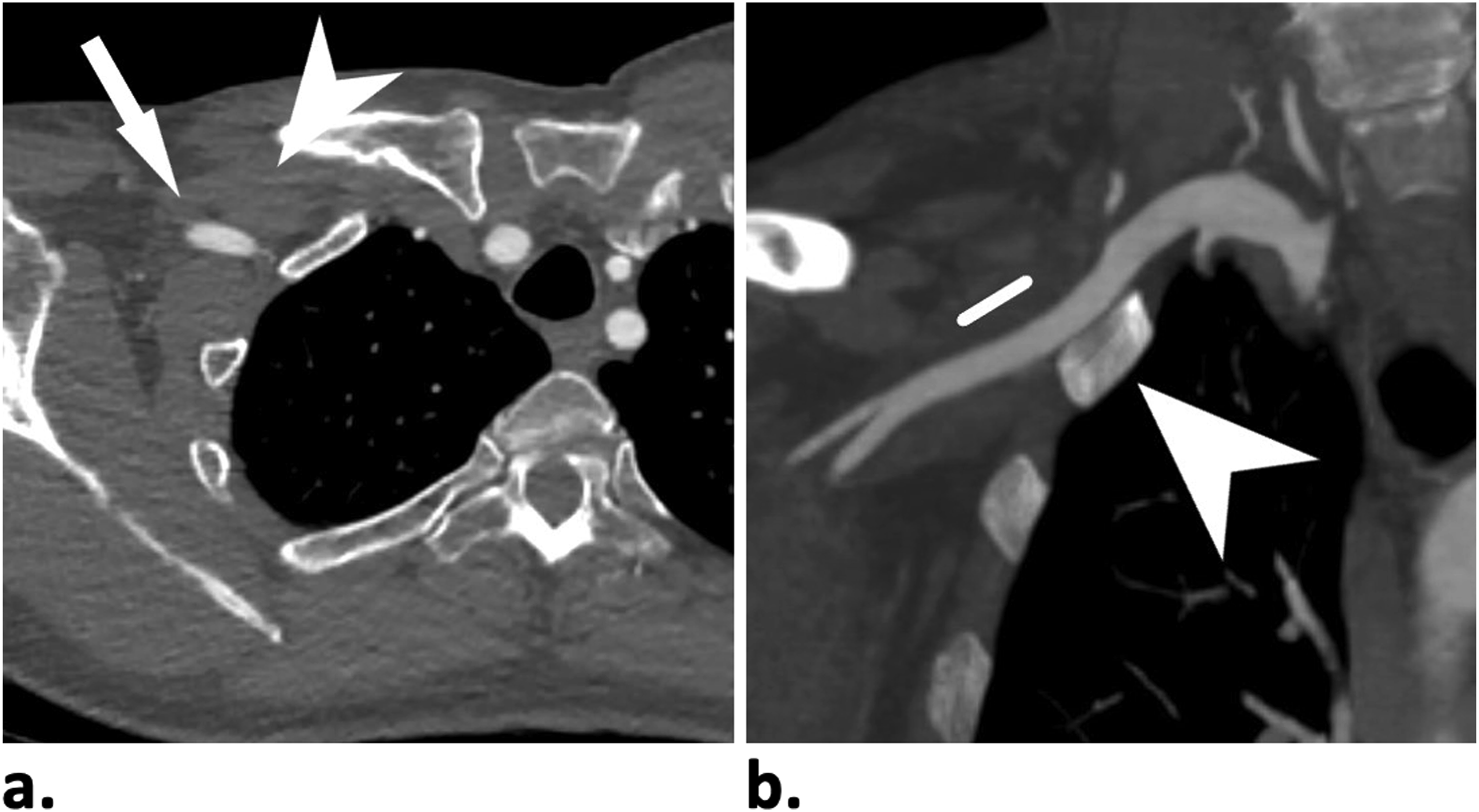
Closure
A range of techniques for obtaining hemostasis of the arteriotomy exist. These range from simply applying manual compression to the artery and allowing for clot formation, to an array of devices designed to obtain hemostasis immediately after deployment, namely, 6Fr and 8Fr AngioSeal (St Jude Medical, Inc. Exton, Pennsylvannia) and Perclose ProGlide SMC (Abbott). These devices were used either individually or in combination, following standard techniques. The use of these devices depended on patient factors such as body habitus, coagulation status, and operator preference. Double AngioSeal technique is predominantly utilized for trans-axillary approach. In this technique, two wires are placed into the axillary artery and sequential AngioSeals are deployed. Often, the second AngioSeal is not needed, so the second wire is removed. If there is a continuous bleeding, however, the second AngioSeal is then deployed. In the rare cases where there is concern about AngioSeal failure (>8Fr sheath access or deep axillary artery), a safety occlusion balloon is placed in the axillary artery via common femoral access during the AngioSeal deployment (Figure 2). Axillary artery closure technique. (a) Closure of 8Fr access left axillary artery with occlusion balloon assistant. Arrow showing the access site just lateral to first rib. Arrowhead showing placement of sheath in the subclavian artery via common femoral access. (b) Arrowhead indicates balloon occlusion of subclavian artery proximal to axillary access during AngioSeal deployment. (c) Completion angiogram demonstration normal axillary artery post AngioSeal.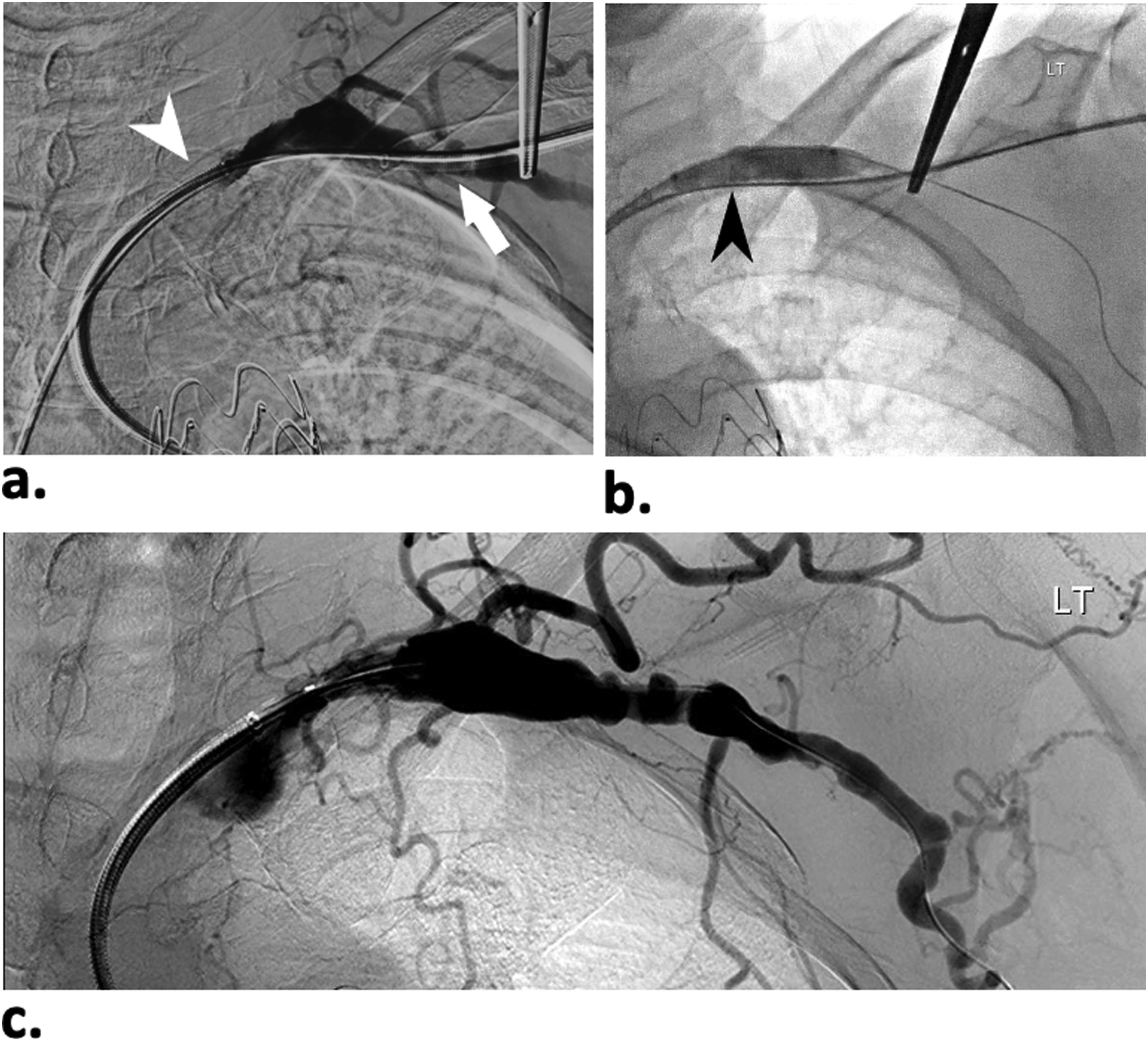
Outcome measures
Complications were the primary outcome measure and were assessed by retrospective review of the relevant electronic patient record for a period of up to 30 days following intervention in all patients, including discharge summaries, clinic notes, and imaging studies on the institutional Radiology Information System. Complications were recorded and classified into simple versus clinically relevant complications based on their clinical significance and modified SIR criteria. 19 Briefly, SIR grade-I, or uncomplicated hematoma, is considered simple complications. Similarly, simple access site dissections with zero consequences are also considered simple complications since these are typically ignored clinically. On the other hand, complicated hematomas and/or dissections (including associated with pseudoaneurysm and/or active extravasation) and other access site complications requiring treatment, are collectively termed “clinically relevant complications” and typically constituted SIR grade II and III. The comparison of access site complications in the current study was based primarily on occurrence of clinically relevant complications. Sheath size, and method of hemostasis were recorded. Patient demographic information such as age and sex were recorded.
Microsoft Excel was used for data collection. The Pearson Chi-Square and Fisher Exact tests, and one-way-ANOVA with adjustment for covariates (ANCOVA) using general linear model were performed to assess for statistical significance (p-value <.05 is considered statistically significant), with Levene’s test used to assess for equality of error variances. All statistical analysis performed using SPSS, version 28.0 (IMB Corp, Armonk, New York).
Results
A total of 67 vascular interventions, 41 (61%) via percutaneous brachial artery access and 26 (39%) via percutaneous axillary artery access met the inclusion criteria and were included in the analysis. There were no significant differences in age, sex, and indication for procedure between patients in the two groups. The average age was 73 years, with 62% of patients being male.
The vast majority (98%) of the procedures were therapeutic, with 80% involving the brachial artery and 62% the axillary artery. Among these therapeutic procedures, 73% were solely therapeutic, involving interventions such as embolization (3%) and EVAR revisions (70%), predominantly targeting renal visceral and aortoiliac areas. The remaining 25% of procedures were diagnostic with angioplasty, performed for conditions such as critical limb ischemia (22%) and claudication (3%). Only one diagnostic procedure was performed on an asymptomatic patient (2%).
30-days follow-up was completed for all cases. Simple, self-limited hematomas, which are minor access site complications occurred in 11% (12% trans-brachial and 8% trans-axillary cases). Minor access site dissections, which are self-limited, occurred in 3% (0% trans-brachial and 8% trans-axillary cases). Complicated hematomas (including pseudoaneurysm and/or active extravasation) and other access site complications requiring further treatment/interventions—clinically relevant complications—occurred in 16% of patients (17% of brachial artery cases n = 7, and 15% of axillary artery cases n = 4). Importantly, there was no statistically significant difference in occurrence of these clinically relevant complications in the two groups: F (1, 65) = 0.358, p = .552; while not violating Levene’s test, p = .243.
Patients’ characteristic and variables used in this study to compare between the two access techniques.
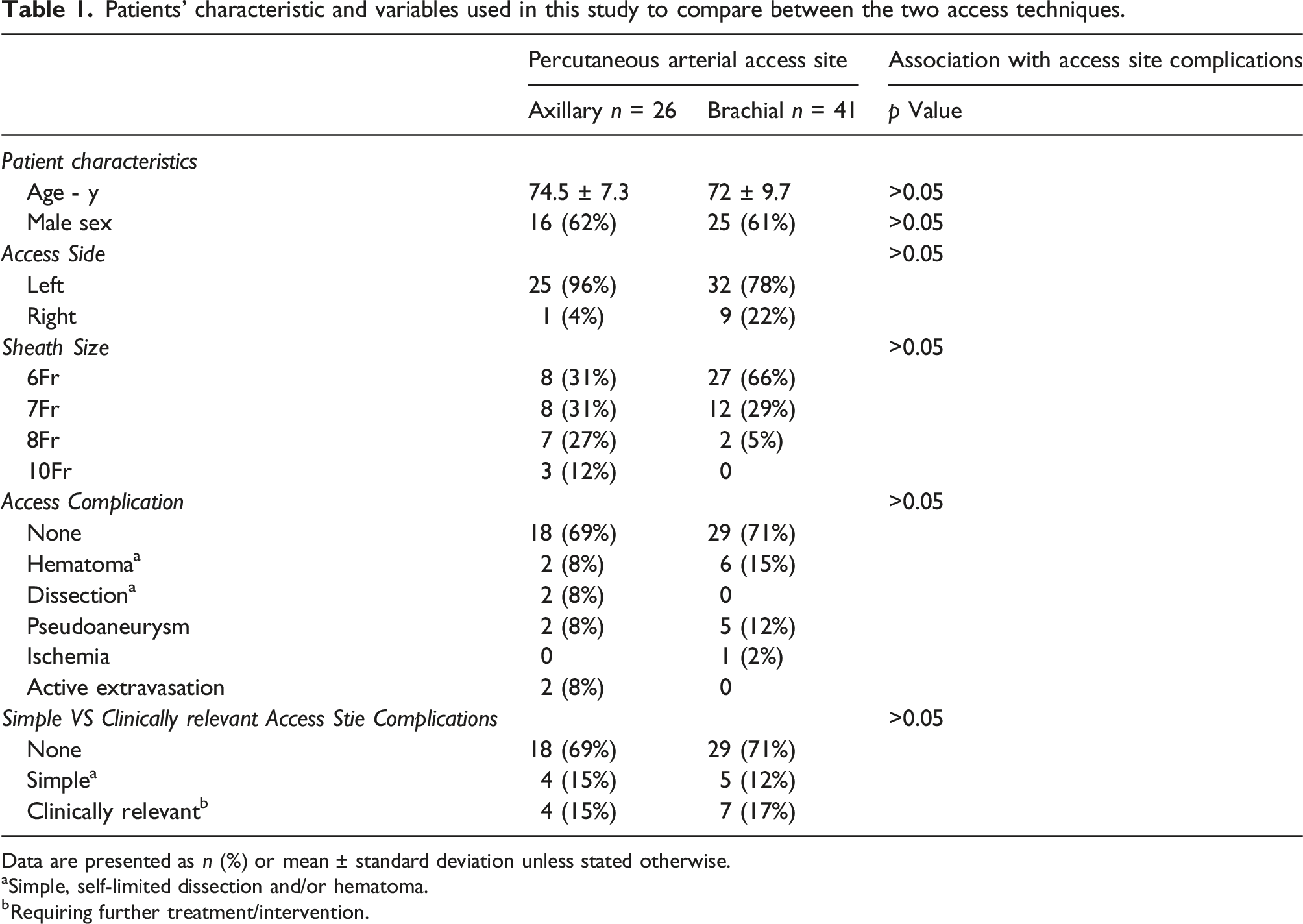
Data are presented as n (%) or mean ± standard deviation unless stated otherwise.
aSimple, self-limited dissection and/or hematoma.
bRequiring further treatment/intervention.
In the trans-axillary group, a pseudoaneurysm occurred in n = 2 (7.7%) patients, both of which required surgical repair after two unsuccessful attempts at percutaneous thrombin injection (SIR Grade-III). Active extravasation developed in n = 2 (7.7%) of patients; the first of which was complicated by a large pseudoaneurysm that failed thrombin injection (1000 units) and balloon occlusion of outflow and therefore had to be repaired surgically; the second case of active extravasation was associated with a rapidly expanding anterior chest wall hematoma from a small perforating branch supplying the pectoralis major, confirmed by CT angiography. The patient was brought back to the angiography suite and coil embolization was performed. The patient was then admitted for monitoring overnight with no further issues arising. All the patients who required surgical repair made a full recovery (Table 1).
All procedures were performed percutaneously under ultrasound guidance, with 100% success with catheterizing the relevant artery. Micro-puncture was performed in vast majority of cases (94%). 7
Sheath sizes included for analysis were 6Fr to 10Fr. In 67% of the trans-brachial arterial cases, the largest access sheath used was 6Fr, followed by 7Fr (29%), then 8Fr (5%). Larger than 8Fr sheath size for brachial artery access was not performed. On the other hand, 6Fr sheath size was largest in only 31% of the trans-axillary cases with the remaining 69% of cases utilized 7Fr, 8Fr or 10Fr sizes (Table 1). Clinically relevant access site complications (SIR grade-II and III) for trans-brachial approach occurred less frequently with 6Fr sheath (7%) when compared to >6Fr sheath sizes (36%); however, this increase was not statistically significant when accounting for covariates; ANCOVA p = .554, Levene’s p = .747. There was no significant association between sheath size and occurrence of access site complication for trans-axillary approach too. Access site complications increased with increased fluoroscopy time (>30 min) but were not statistically significant; Pearson Chi-Square p-values = 0.104.
Vascular access site hemostasis techniques.
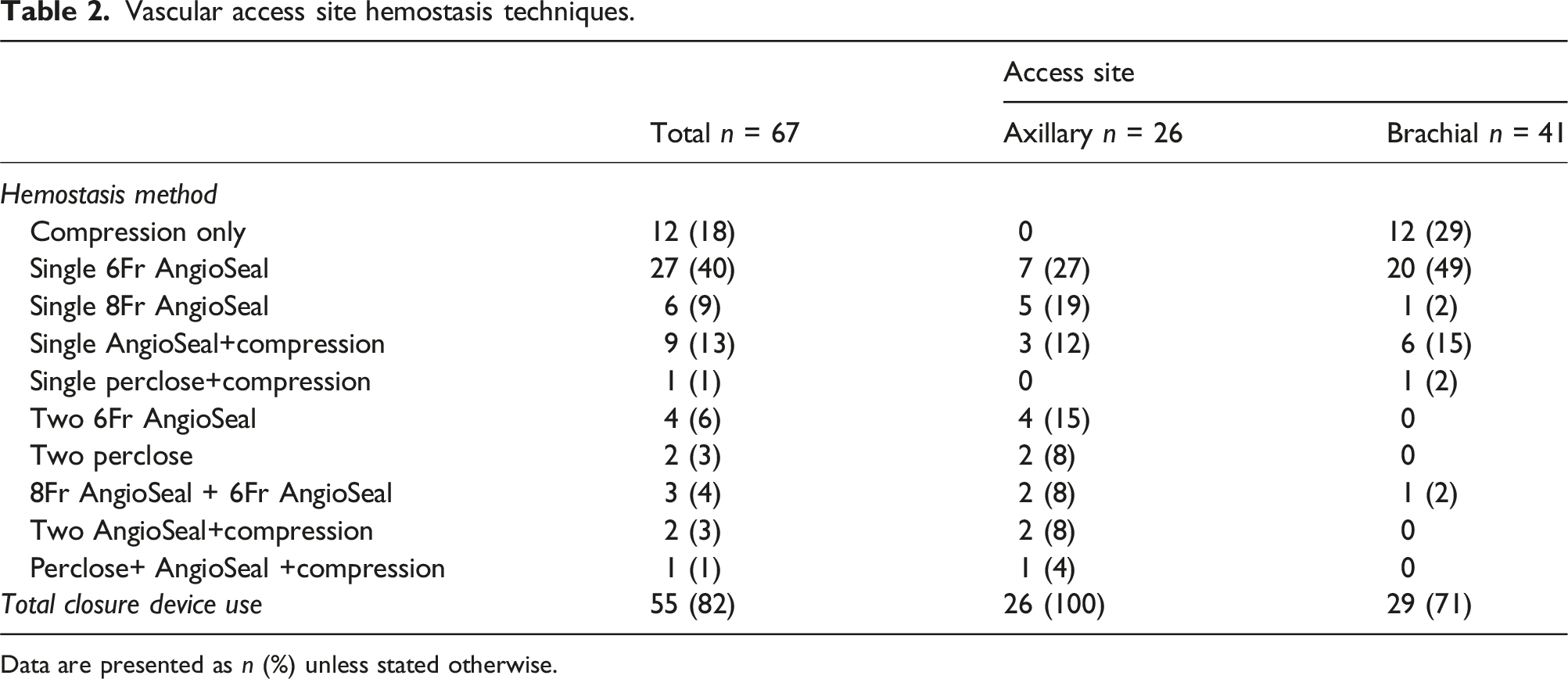
Data are presented as n (%) unless stated otherwise.
The length of vascular procedure was comparable between the two techniques with 42% and 47% of trans-axillary procedures took 10–30 min and >30–60 min, respectively; in comparison 33% and 49% of the trans-brachial procedures took 10–30 min and >30–60 min, respectively. There was no statistically significant difference in procedure length. Side of vascular access was predominantly on the left side, with trans-axillary approach on the left side in 96% of the time versus 78% for the trans-brachial access. Stoke symptoms were not experienced in any of the patients.
Discussion
The trans-axillary approach for upper limb arterial puncture is valuable and should be considered when using a sheath size of seven or greater, while the trans-brachial approach is recommended for sheath sizes of 6F or smaller. This study explores our institution’s experience with axillary artery punctures, using access sheath sizes ranging from 6Fr to 10Fr and employing closure devices. The study findings indicate no significant statistical difference in access site complications between the trans-brachial and trans-axillary approaches when using sheaths sized ≥6Fr to 10Fr. The rate of clinically relevant access site complications was 17% for trans-brachial and 15% for trans-axillary techniques. However, it’s notable that larger sheath sizes were more commonly used in trans-axillary cases, with 69% utilizing ≥7Fr sheaths compared to 34% of brachial cases. The study observed a tendency towards increased access site complications with larger access sheath caliber in the brachial artery, likely due to its smaller size limiting the accommodation of ≥7Fr sheath. Although statistically insignificant due to limited observations, the trend towards higher complication rates with larger sheaths in the brachial artery suggests caution in selecting sheath sizes.
The selection of sheath sizes between 6Fr to 10Fr in this study was based on prior reports indicating that sheath size ≥6Fr predicts access-related complications.2,20–23 The slightly increased preference for the trans-brachial approach over trans-axillary (61% vs 39%) in this study possibly reflects prevailing practices at the time. The axillary artery’s comparability in size to the common femoral artery makes it conducive to larger caliber sheaths, thus representing an underutilized but valuable access site for upper limb percutaneous endovascular procedures requiring sheath sizes 6Fr and larger.2,8,20 Other groups including cardiologists are also increasingly using axillary access for heart support device (Impella); therefore, there is likely to be increased popularity for this access site. 21
Previous research has highlighted significant rates of complications related to upper limb access sites. For instance, Mirza et al. reported access site complications in trans-brachial interventions to approach 32%, while Chesner et al. indicated rates reaching 31%, including both minor and clinically relevant complications. Perclose utilization was associated with estimates as high as 57%, compared to 16% with manual compression according to Meertens et al.22–24 Similarly, trans-axillary interventions, as reported by Kajy et al., demonstrated access site complications at 27%, with clinically relevant complications estimated at 24%. Nijres B.M. et al. estimated the occurrence of clinically relevant access site complications at 19%.25,26 Other studies have estimated complication rates for upper limb access sites to range between 11%–18%.5,6,27–29 Some of these studies encompassed numerous diagnostic cases, typically associated with lower complication risks. Additionally, several studies included smaller-bore access sheaths, while others only considered hematoma as a complication if it caused secondary adverse effects such as neuropathy.5,6,27–30 Notably, none of the access-related complications in our study were linked to neuropathy or brachial plexus injury. Furthermore, no site complications necessitated stent implantation. However, Schafer et al. estimated that complications requiring stent implantation after sheath removal occurred in 11% of cases involving trans-axillary access. 31
The study also discusses the utility of closure devices, with the axillary artery access showing no occlusion complications compared to the brachial access. This is not surprising since axillary artery is much larger therefore able to accommodate closure devices. However, compression of this artery is much more difficult compared to brachial, hence may result in more hematomas/pseudoaneurysm should the closure devices fail. Our general rule is that if access larger than 7Fr is needed, axillary artery is the access of choice. Hematomas with pseudoaneurysms are slightly more common with axillary artery access. In cases involving the brachial artery, hemostasis is achieved through manual compression alone in 29% of cases, while in 69% of cases, a single closure device is used. Perclose is used in only 6% of cases, primarily in trans-axillary procedures. 23 In our study, AngioSeal is the primary closure device, predominantly used in trans-axillary procedures. In trans-brachial artery cases, a single 6Fr AngioSeal is commonly used. The use of closure devices in trans-brachial access does not impact access complication rates. Axillary artery cases typically use vascular closure devices, with either a single or double AngioSeal technique. 8 For trans-axillary hemostasis, two closure devices are commonly used, with no apparent association with access site complications.
Limitations of the study include its single-center, retrospective, nonrandomized design, along with a moderately small sample size, which may limit the power of relevant observations. For instance, access site complications tended to increase with procedure duration, but this trend was not statistically significant. Access site selection depended on individual case characteristics and operator preference, potentially introducing bias into the results. To address these limitations, robust statistical methods such as ANCOVA were employed to adjust for covariates when significant associations were found. Cases involving sheaths larger than 10Fr were excluded to maintain homogeneity between groups, as were cases involving surgical cut down of the brachial artery due to their infrequency. Larger studies are needed to better assess the safety of the trans-axillary technique, particularly when using sheaths larger than 6Fr, compared to more commonly used upper limb arteries such as the trans-brachial and trans-radial approaches.
Conclusion
Axillary access serves as a safe and effective method for procedures requiring a sheath size of 7F or larger. However, utilizing specific access techniques and modified closure methods is crucial for safe hemostasis. Instances of arterial occlusion are uncommon with this approach, even when employing large-bore vascular access, and the need for surgical conversion due to pseudoaneurysm or bleeding complications remains rare. Conversely, accessing the brachial artery is simpler, although it is limited to smaller devices. Despite a similar pseudoaneurysm rate, it carries a higher risk of arterial occlusion. Surgical conversion rates are similar for both techniques. Nevertheless, brachial access tends to result in more occlusion occurrences, while axillary access is more susceptible to bleeding complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.