
Abstract
Background
Endovenous interventions and minimally invasive procedures are effective in the management of varicose veins. However, they can cause postoperative discomfort.
Objective
To evaluate the clinical efficacy of sodium aescinate (SA) in improving edema, pain, vein-specific symptoms, and quality of life in patients following endovenous laser ablation (EVLA) for varicose veins.
Methods
In this single-center randomized controlled trial (RCT), patients were allocated into two groups: in Group A, 60 mg SA was administered twice daily for 20 days, and in Group B (control), no venoactive drug was prescribed. The Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification system for chronic venous disorders was used to assess the varicose veins. The circumferences of the calf and ankle were recorded for evaluating edema. The 10-point Visual Analog Scale (VAS), Venous Clinical Severity Score (VCSS), and Aberdeen Varicose Veins Questionnaire (AVVQ) were used to measure the pain intensity, overall varicose vein severity, and patient’s quality of life, respectively.
Results
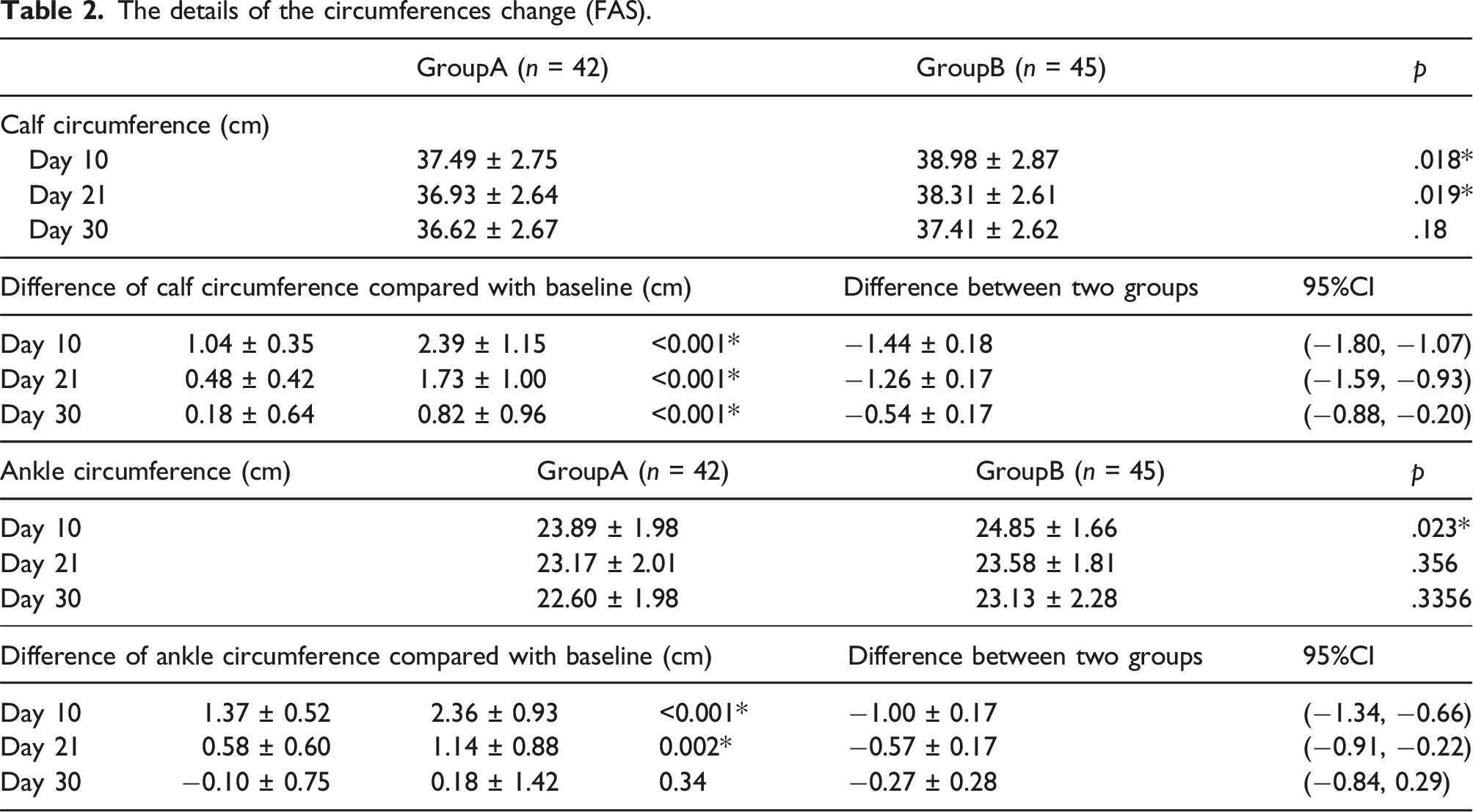
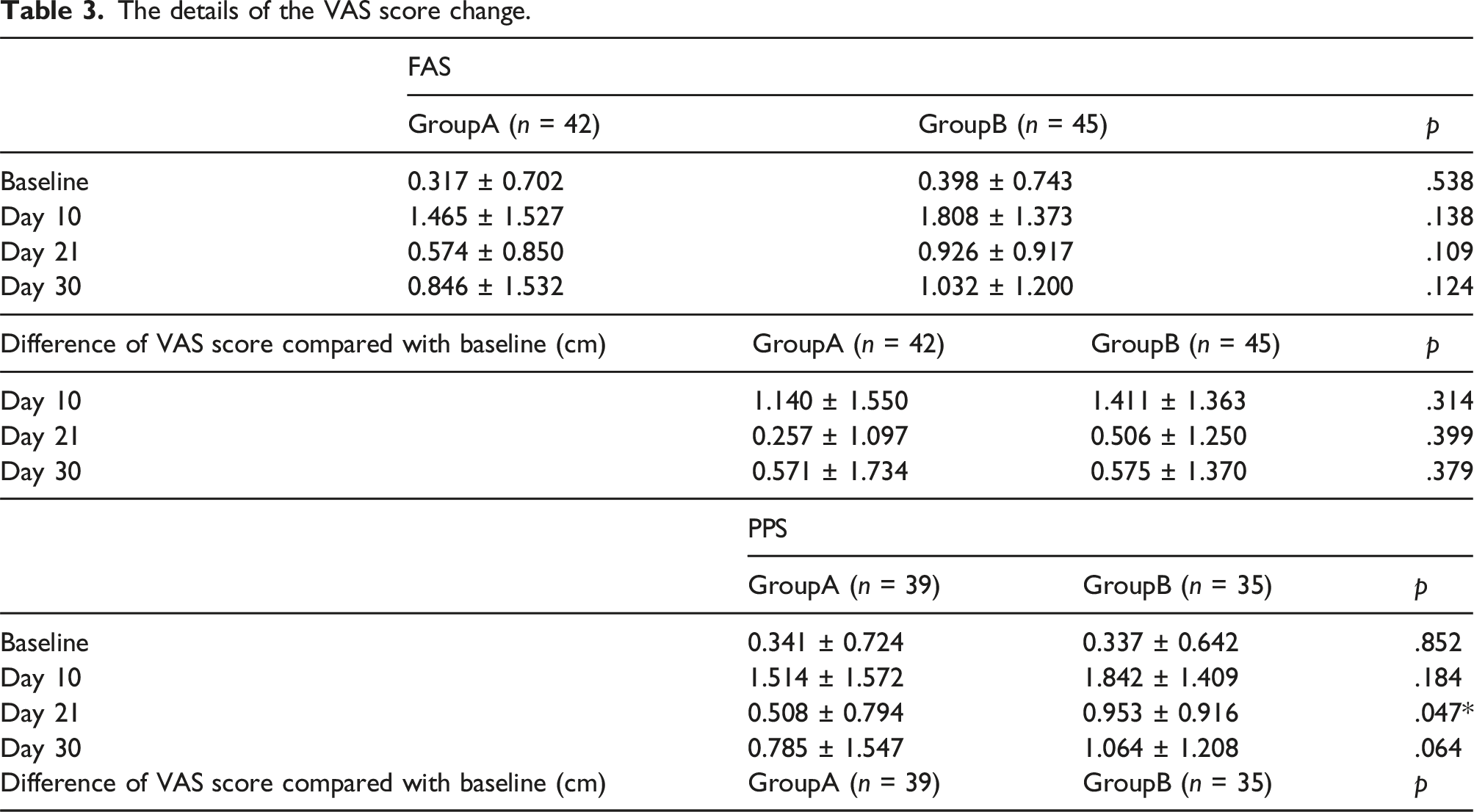
The study included 87 patients (mean age, 59.9 ± 10.7 years; 54 men) with CEAP class C2–C5 varicose veins who underwent EVLA and phlebectomy or foam sclerotherapy. The calf circumference recovered quicker in Group A than in Group B by days 10, 21, and 30 (difference from baseline was 1.04 ± 0.35 vs 2.39 ± 1.15 [p < .001], 0.48 ± 0.42 vs1.73 ± 1.00 [p < .001], and 0.18 ± 0.64 vs 0.82 ± 0.96 [p < .001], respectively). The ankle circumference recovered quicker in Group A than in Group B by days 10 and 21 (the difference from baseline was 1.37 ± 0.52 vs 2.36 ± 0.93 [p < .001] and 0.58 ± 0.60 vs 1.14 ± 0.88 [p = .002], respectively). Pain relief was achieved quicker in Group A than in Group B (0.257 ± 1.097 [p = .0863] vs 0.506 ± 1.250 [p = .0168] by day 21). There were no significant differences in the VCSS and AVVQ scores between both groups. There were no drug-related adverse effects.
Conclusions
SA, in combination with compression therapy, can relieve edema and alleviate pain in patients following EVLA for varicose veins.
Introduction
Varicose veins (VV) are a prevalent medical condition that significantly impacts a patient’s quality of life (QoL), particularly in its advanced stages. Over the past two decades, endovenous procedures have become popular as a minimally invasive alternative to traditional surgery, saphenofemoral ligation and stripping (SFL/S), for VV. 1 Endovenous laser ablation (EVLA) is reportedly effective and widely used for the treatment of VV.
Although severe postoperative complications are relatively rare following EVLA, it can cause several uncomfortable side effects, including edema, pain, hematoma, and a burning sensation. According to Zhang et al., the probability of edema developing after EVLA is 62%–67%. 2 In another study, edema developed in 40.0% and 65.5% of the patients in the EVLA and radiofrequency ablation (RFA) groups, respectively. 3 Despite its effectiveness, improving postoperative discomfort and promoting early and rapid recovery of patients are key issues related to EVLA.
Elastic compression stockings (ECSs) are highly recommended for patients following surgery for VV to reduce pain and improve physical function. Venoactive drugs can also facilitate the recovery process for primary VV. Additionally, according to recent systematic reviews, venoactive drugs can reduce VV symptoms such as edema. However, studies on the effect of venoactive drugs, such as sodium aescinate (SA), on patient recovery following EVLA are scarce. Therefore, we aimed to evaluate the clinical efficacy of venoactive therapy in reducing post-EVLA edema, pain, and symptoms and improving the patient’s QoL.
Patients and methods
Patients and study design
This was a single-center randomized controlled trial (RCT). Patients who underwent EVLA at the Vascular Surgery Department in our hospital between 1 March 2021 and 30 September 2021 were enrolled in this study. Duplex ultrasound was conducted in the upright position to map sources of venous reflux and reverse flow of >0.5 s at the saphenofemoral junction (SFJ) was considered pathological.
4
The enrolled patients were allocated into two groups with a 1:1 allocation ratio. In Group A, 60 mg SA was administered twice daily for 20 days after EVLA procedure. In Group B (control), no venoactive drug was prescribed. All patients wore a thigh high ECS (Class II, ankle pressure of 23–32 mmHg) with an open toe distally during the daytime (removed only at the time of measurements).
5
Patients were included after obtaining a signed informed consent form. The study was approved by the local ethics committee and institutional review board (SH9H-2020-C40-1, date of approval: 2020.11.2) and registered in the Chinese Clinical Trial Registry [No: ChiCTR2000041029]. (Figure 1). Flow diagram.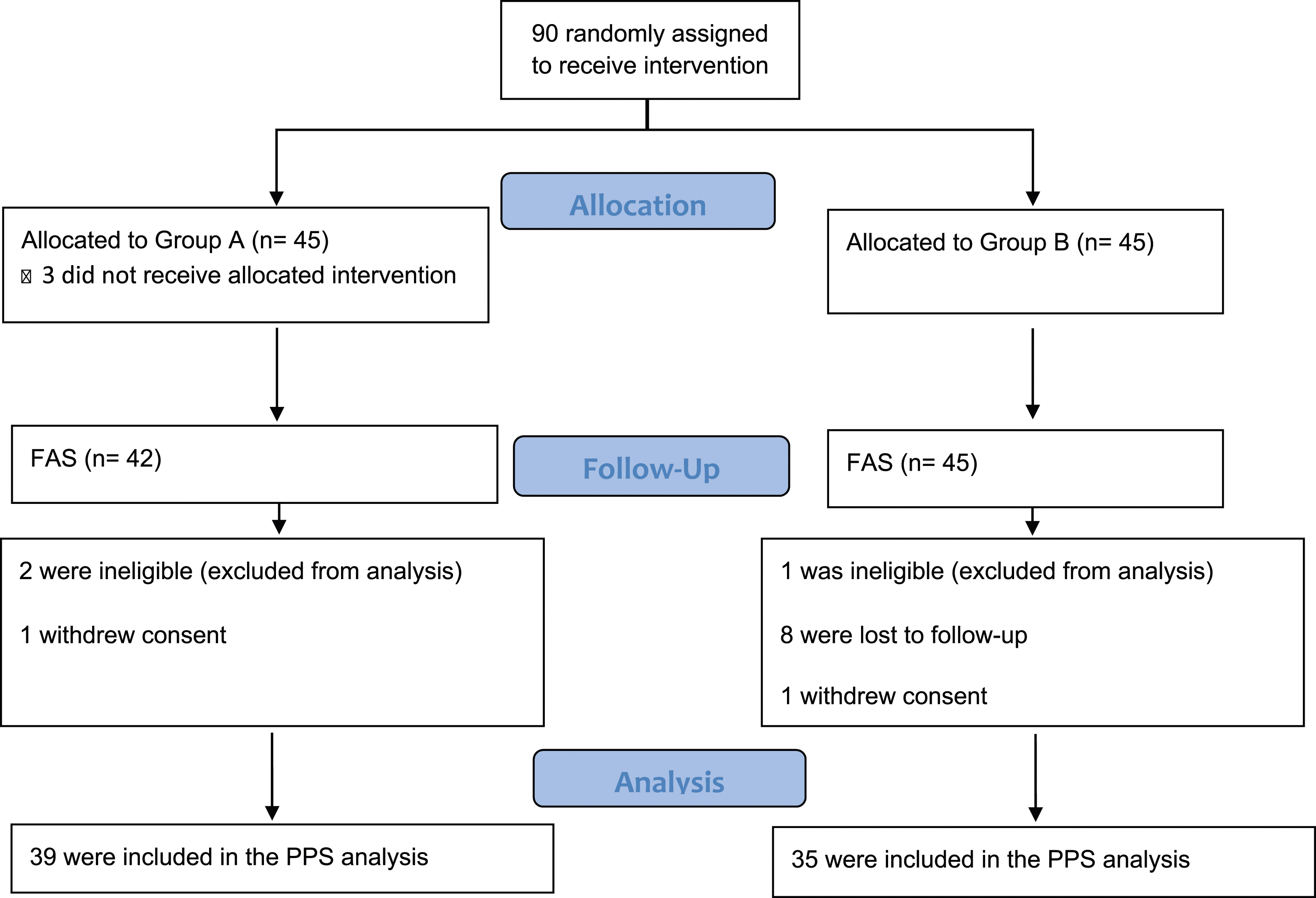
Inclusion and exclusion criteria
The inclusion criteria were as follows: age >18 years, Clinical-Etiology-Anatomy-Pathophysiology (CEAP) class C2–C5 for chronic venous disorders, and no contraindication to surgery. The exclusion criteria were as follows: previous VV surgery, treatment of both lower limbs in the same sitting, recent use (within 1 month) of antiedema medications (venoactive medications or diuretics), edema caused by other reasons (cardiogenic, hepatic, renal or lymphatic conditions); stenosis/occlusion of deep veins, known allergy or intolerance to SA, patient refusal to participate in the study, inability to wear ECSs, prior use of ECS or an elastic bandage, and arterial disease (with ankle-brachial index <0.9).
Interventions - EVLA procedure
Patients underwent EVLA and high ligation of the great saphenous vein (GSV) according to a standardized protocol.5,6 Following regional anesthesia, the proximal GSV was dissected and ligated at the SFJ. Using the Seldinger technique, the distal GSV was punctured at the ankle level, through which a guidewire and catheter were passed proximally to the SFJ. A 980-nm diode laser was used to deliver approximately 80 J/cm of energy, while the fiber and catheter were withdrawn simultaneously at a speed of 1–3 mm/s. The laser was continuously applied with the same power (12 W). Incompetence of anterior accessory veins and small saphenous veins were treated in the same procedures. Additional sclerotherapy or phlebectomies were performed at the discretion of the vascular surgeons. Prophylactic medications for deep vein thrombosis and wound infection were not prescribed. Patients were encouraged to resume their daily activities and return to work as soon as possible.
Follow-up and endpoints
All the patients were dynamically followed-up; visual examination, limb photography, and ultrasound examination were performed. The follow-up visits were scheduled on days 10 ± 5, 21 ± 3, and 30 ± 5 after surgery.
The primary endpoint was the degree of edema relief on day 21 ± 3, which was the change in calf circumference. The other endpoints were as follows: changes in ankle circumference by days 10, 21, and 30; venous clinical severity score (VCSS); pain visual analog scale (VAS], ranging from 0 to 10; and patient’s QoL, determined using the Aberdeen Varicose Vein Questionnaire (AVVQ).
Sample size and randomization
Based on the literature review and previous experience, the sample size was calculated assuming a mean change of 1.2 cm in calf circumference with a standard deviation of 1.8 cm. The type-1 error of the study was set at 0.05, and the power was set at 80%. The sample size was calculated to be 36 patients for each study group. To compensate for dropouts, 20% more patients were required. Thus, at least 45 patients needed to be included in each group. Finally, after obtaining informed consent, 90 patients who met the inclusion conditions in the screening period were randomly assigned to Group A or B in a ratio of 1:1. A random table was generated in SAS (SAS Institute Inc.,Cary,NC,USA.Version 9.4) using the block randomization method.
Statistical analysis
Normally distributed data are presented as means with standard deviations, non-normally distributed data as medians with interquartile ranges, and categorical data as proportions. Both the primary and secondary investigations were analyzed using the full analysis set (FAS) and Per protocol set (PPS), and patients in the group were compared. If patients were lost to follow-up, the last available measurement prior to withdrawal was included in the analysis (last observation carried forward). To compare the patient demographics and clinical characteristics, the Fisher exact test was used for categorical variables, and the Student t test was used for continuous variables. All statistical analyses were performed using SPSS (version 21.0; SPSS Inc., Chicago, IL, USA). A p-value of <0.05 was considered significant.
Results
Patients’ clinical and demographic characteristics
Baseline patient demographics and clinical characteristics.
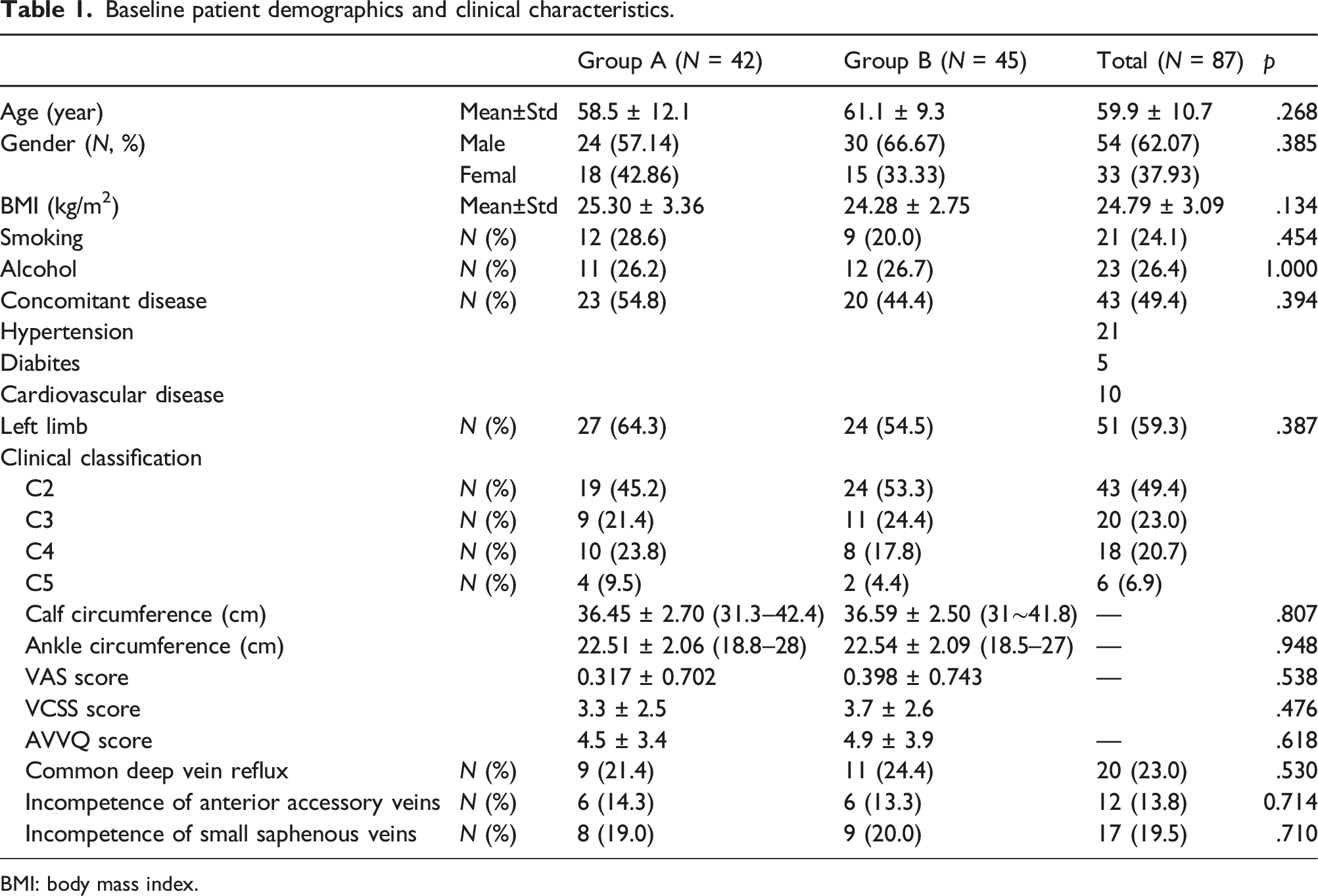
BMI: body mass index.
Treatment outcomes
The details of the circumferences change (FAS).
The details of the VAS score change.
The incidence of adverse events was 16.7% (n = 7) in Group A and 11.1% (n = 5) in Group B. There were no severe adverse events. Gastrointestinal discomfort was reported by five patients, and two of them stopped taking the medications. Cardiac discomfort was reported by two patients in Group A. Skin reactions developed in four patients in Group B, and one patient experienced hypersensitivity in Group B. There was no statistically significant difference in the incidence of adverse events between the two groups (p = .255). ECS was used at least 6 days a week by 65 patients (74.7%), 4–5 days a week by 13 patients (14.9%), and <4 days a week by nine patients (10.3%). There was no statistically significant difference in ECS use between the two groups (p = .530).
Discussion
Herein, we aimed to assess the efficacy of adjuvant treatment with SA for patients experiencing venous insufficiency following an endovenous ablation procedure. The results indicated that SA can alleviate postoperative edema and pain with good tolerance, making it suitable for short-term postoperative use. However, there were no significant differences in the VCSS and AVVQ scores between the two treatment groups.
Currently, endovenous thermal ablation is the most commonly employed treatment method for primary VV. It provides a high level of safety and efficacy, is minimally invasive, can be easily performed, and demonstrates favorable occlusion rates for saphenous vein insufficiency. Although serious complications such as deep vein thrombosis are rare, patients may still experience minor discomforts, including pain, edema, and bruising, that can disrupt their recovery and daily activities. Various methods are available to manage postoperative discomfort. Compression therapy, which is frequently used following invasive treatments for VV, aims to reduce pain, bruising, and edema. However, the outcomes of studies examining compression therapy are contradictory. In one study, 7 the prolonged use of compression therapy effectively alleviated postoperative pain and reduced the time taken off from work after endovenous thermal ablation. Present study’s findings suggested that compression stockings potentially enhance the recovery of patients who have undergone endovenous thermal ablation for VV. However, several recent RCTs8–10 have demonstrated that patients undergoing endovenous thermal treatment do not experience any benefits from the use of compression stockings. Moreover, several patients encountered discomfort and difficulties while wearing the compression stockings. The evidence regarding the use of compression stockings is highly heterogeneous. The efficacy of ECSs significantly depends on patient compliance, which directly impacts the potential benefits of this non-invasive therapy.11,12
Escin is the active component of Aesculus hippocastanum (the horse chestnut), which was itself used as a traditional medicine for centuries.13–16 Escin is known for its anti-inflammatory and anti-edematous effects. It works by reducing vascular permeability in inflamed tissues, thereby inhibiting the formation of edema. Additionally, escin has venotonic effects, primarily demonstrated through in vitro studies on isolated human saphenous veins. 17 Its ability to prevent hypoxia-induced disruption to the normal expression and distribution of platelet endothelial cell-adhesion molecule-1 contributes to its protective effect on blood vessel permeability. 15 SA is sodium aescinate is a derivative of escin. It shares similar therapeutic properties with escin. An RCT involving 240 patients with chronic venous insufficiency demonstrated that horse chestnut seeds were effective in reducing CVD-induced edema and were as effective as compression therapy. 14 However, the evidence regarding SA use is outdated, especially for postoperative use. The latest systematic review, which was published in 2012, included 17 relevant studies on horse chestnut seed extract. 18 These studies demonstrated significant improvements in lower limb pain, edema, itching, and volume after 2 weeks of treatment. 19 In our study, we observed severe edema and pain scores on postoperative day 10, which gradually decreased by day 20 and day 30; these findings are consistent with those of previous studies on EVLA. Patients typically experience postoperative discomfort, which subsequently improves after 2 weeks. Our study findings are consistent with existing evidence regarding the recovery time for pain and edema. SA are well-tolerated when administered orally, with mild gastrointestinal disorders being the most common adverse events reported. Other adverse events are headache, dizziness, flushing, itching, and fatigue. 20 Our findings were consistent with previous data.
There was no significant improvement in the VCSS and AVVQ scores in our study. Although there seemed to be a trend in the difference of VCSS and AVVQ scores compared with baseline, it did not reach statistical significance (Supplemental Tables 2 and 3). Several factors could potentially explain this lack of improvement. First, our study participants may have had a milder condition than those in other studies, which could explain the limited change in VCSS and AVVQ. Second, the sample size was calculated based on edema reduction. As secondary endpoints with multiple variables, the sample size of our study might not have been sufficient to demonstrate differences. Additionally, the follow-up duration in our study was relatively short, which may not have allowed for significant improvement in VCSS and QoL to occur.
The current study had several limitations. A major limitation of this study is that the participants could not be blinded to the intervention. However, the investigator who analyzed the data was blinded to reduce potential biases. Another limitation of the study is that all patients received treatment using a 980-nm bare-tip fiber. Although this approach is reportedly associated with a higher level of discomfort than the use of a radial fiber at a higher wavelength,21,22 it was chosen to reduce the bias of treatment. The fact that almost 50% of the patients presented with C2 chronic venous disease was another limitation of the study. The milder condition explains why the VCSS and AVVQ scores did not improve significantly. Thus, studies involving patients with more serious symptoms and clinical classifications should be conducted. Besides, the demographic distribution of patients in this case is noteworthy because only 33% were female. This gender distribution is atypical for VV, where traditionally a higher proportion of female patients are observed. 23 In China, radiofrequency ablation is also being concurrently conducted. To eliminate the potential impact of treatment modality on postoperative recovery, we excluded individuals who underwent RFA. In our center, there is a tendency for female choose for more minimally invasive method with higher postoperative comfort levels. 24 Cost is another consideration, RFA is associated with higher expenses in China. These may have resulted in a bias in the composition of the study population. Finally, the study only assessed the short-term outcomes. Future studies with larger sample sizes that assess the long-term outcomes are needed for more robust statistical analyses.
Conclusion
In conclusion, SA, in combination with compression therapy, can relieve edema and alleviate pain in patients who have undergone EVLA for VV.
Supplemental Material
Supplemental Material - Clinical efficacy of sodium aescinate administration following endovenous laser ablation for varicose veins
Supplemental Material for Clinical efficacy of sodium aescinate administration following endo-venous laser ablation for varicose veins by Xinrui Yang, Jian Jin, Siyi Huang, Peng Qiu, Ruihua Wang, Kaichuang Ye and Xinwu Lu in Vascular.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by these funding as follows: Shanghai Science and Technology Innovation Action Plan (20Y11909600), Fundamental Research Program of 9th People’s Hospital (JYZZ170) and Shandong Luye Pharmaceutical Co., Ltd.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.