
Abstract
Background
Emergency computed tomography angiography (CTA) is the most important imaging modality to visualize arterial occlusions in patients with acute lower limb ischaemia (ALI). Extravascular incidental findings (EVIFs) have received less attention.
Purpose
The aims of this study were to evaluate the incidence of EVIFs of immediate clinical relevance in patients with ALI undergoing CTA and evaluate the association between EVIFs and emergency revascularization and amputation-free survival at 1 year.
Methods
Retrospective cohort study. Emergency CTA in patients with ALI between 2015 and 2018 were independently scrutinized by two senior radiologists. EVIFs were classified into immediate (category I), potential (category II) or no clinical relevance (category III). Multi-variable binary logistic regression analysis was expressed in Odds ratios (OR) with 95% confidence intervals (CI).
Results
The intra-class correlation (ICC) coefficient for EVIF category I between the raters was 0.94 (95% CI 0.92–0.96). Among 118 patients with ALI, 78 patients underwent emergency revascularization. Forty-six EVIFs (34 patients) were category I, of which 63% were found in the chest, including pleural effusion (n = 12), pneumonia (n = 8) and cardiac thrombus (n = 4). Ascites (n = 4) and cancer disease (n = 4) were other category I findings. Category I EVIFs were associated with reduced rate of emergency revascularization (OR 0.26, 95% CI 0.10–0.66) and increased rate of combined major amputation/mortality at 1 year (OR 2.9, 95% CI 1.1–8.2) in adjusted analysis.
Conclusion
It is important to evaluate EVIFs in emergency CTA in patients with ALI since these findings are both common and associated with reduced emergency revascularization and amputation-free survival at 1 year.
Keywords
Introduction
Acute limb ischaemia (ALI) is distinguished by a sudden decrease of arterial blood flow, threatening the survival of the limb.1,2 The Rutherford ALI classification is a system to grade the severity of ischaemia, where type IIb involves motor deficit, and where the limb is immediately threatened. 1 Patients with ALI need to be immediately identified and transferred to hospitals with access to vascular surgeons. 2 Emergency computed tomography angiography (CTA) has become the most important imaging modality around the clock to diagnose the localizations and extent of occlusive arterial disease in the lower extremities. 3 Performance of CTA has recently been reported to be associated with a higher amputation-free survival in revascularized patients with ALI and motor deficit in a propensity score adjusted analysis in a cohort of 260 patients. 4 Therefore, CTA has emerged as a tool to provide guidance in selecting the most appropriate candidates for revascularization and choice of technique, endovascular, open vascular or hybrid vascular surgery. 4
The role of extravascular incidental clinical findings (EVIFs) on CTA of the abdomen and lower extremities in the management of patients with ALI is limited. 5 The aims of the present study were to evaluate the incidence of EVIFs of immediate clinical relevance in patients with ALI undergoing CTA and evaluate the association between EVIFs and emergency revascularization and amputation-free survival at 1 year.
Materials and methods
Study design and population
The study complies with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement for cohort studies (Supplementary Table 1). Retrospective cohort study. Data derives from a tertiary referral vascular center. All CTA of the lower extremities between 1 January 2015 and 31 December 2018 in the SECTRA Radiology Information System (RIS) were retrieved. In all, 1284 examinations in 1087 patients were reviewed, resulting in 118 patients with confirmed ALI according to definition. 6 Reports of the CT angiographies were performed by radiologists in 71 (60.2%) and vascular surgeons in 47 (39.8%) of the CT-examinations. Patients were followed from the day on admission up to 1 year regarding major amputation or death. Survival was checked in the Swedish Population registry based on the patient´s personal identity number.
CTA technique
Run-off CTA scanning was done from hemidiaphragms to the forefoot. Seventy-nine patients were scanned with Siemens Somatom Definition Flash (Siemens Healthineers, Erlangen, Germany) and 39 patients were scanned with Canon Aquilion One (Canon Medical Systems, Ōtawara, Tochigi, Japan). The following acquisition parameters were used for Siemens Somatom Definition Flash: Dual Energy (DE) 80/Sn140 kVp tube voltage, 210/81 mAs reference tube current-time product with tube current modulation CareDose4D; rotation time 0.33 s; collimation with 128 × 0.6; pitch of 0.85. The acquisition parameters for Canon Aquilion One were: 100 kVp tube voltage, tube current modulation with Sure Exposure 3D (SD 12.5, 600 mA max/50 mA); rotation time 0.5 s; collimation 0.5 × 80; pitch of 0.813. Iohexol 90 mL 350 mg I/ml (Omnipaque 350 mg I/ml, GE Healthcare Limited Little Chalfont, England) followed by 50 mL saline flush at flow rate 5 mL/s were injected via an 18 G intravenous cannula placed in an antecubital vein. Arterial phase images were obtained 5 s after bolus detection in the suprarenal aorta (threshold 120 HU for Siemens Somatom Definition Flash and threshold 180 HU for Canon Aquilion One). The scanning was done in two series; first from the level of right atrium to middle of femur and secondly from hips to forefoot. All the images were reconstructed with 1 mm and 3 mm thickness in axial plane. A reconstruction with coronal and axial plane with 2 mm thickness were also done.
Classification of incidental findings
All CTA studies were independently re-evaluated by two radiologists (one interventional radiologist and one general radiologists with 14 and 20 years of clinical experience, respectively). The extravascular incidental findings (EVIFs) were classified into immediate clinical relevance (category I), potential clinical relevance (category II), or no clinical relevance (category III).
5
Category I findings needed immediate further investigation or therapy due to suspicion of malignancy, inflammatory disease or cause of acute limb ischaemia like cardiac thrombus in a patient with embolic ALI (Figure 1). Category II findings implicated need for further investigation after treatment for ALI. Category III findings included benign changes or age-related processes. Examples and classification of EVIFs by category are presented in Supplementary Table 2. The classification of the clinical relevance of EVIFs was verified using medical history and/or patient records. Extra-vascular incidental findings Category 1. Thrombus in the left ventricle.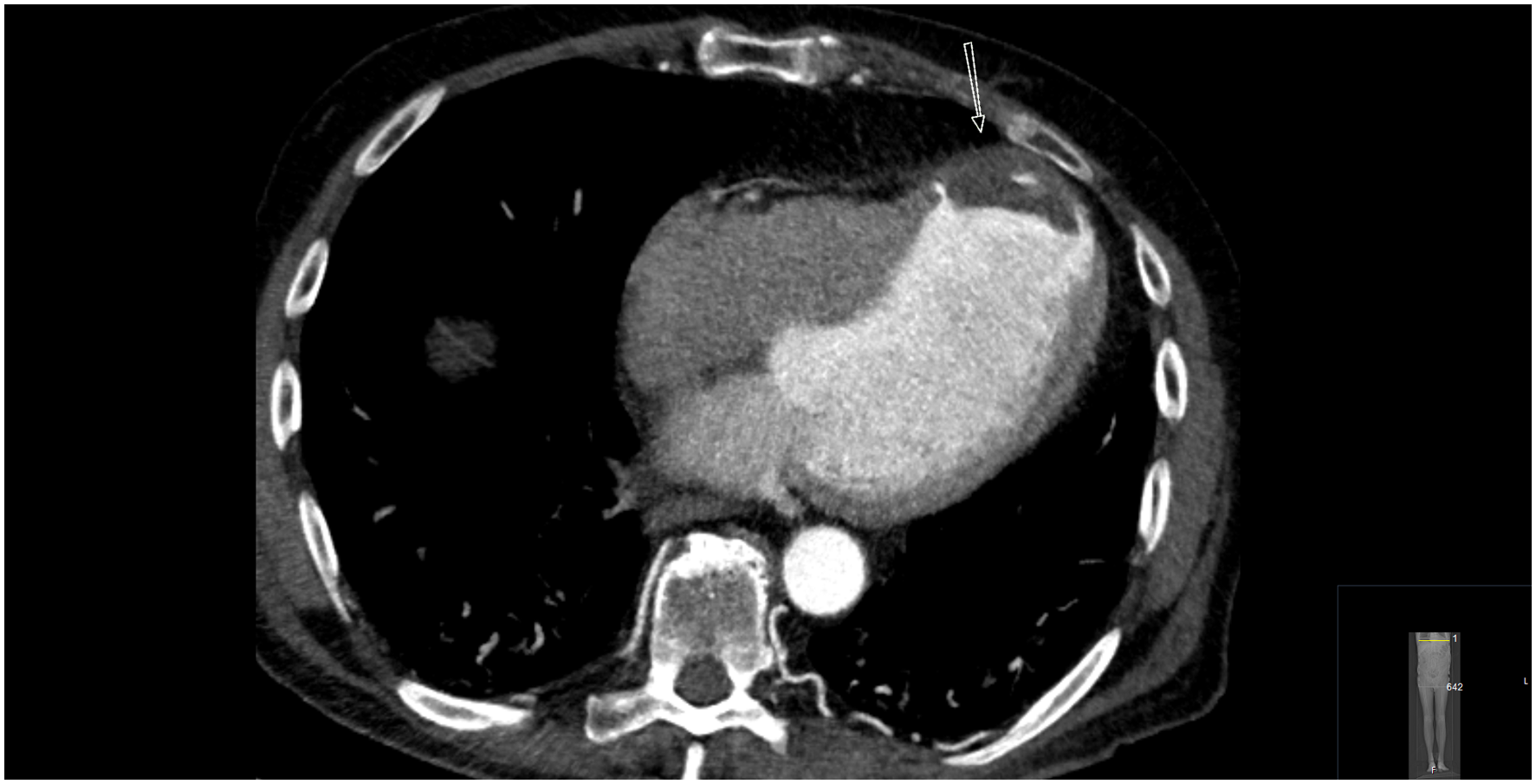
Classification of native artery occlusion
The nature of native artery occlusion, embolic or thrombotic was determined by appearance of occlusion and extent of atherosclerotic wall lesions at CTA. 3 Embolic occlusion appears often as an oval-shaped clot surrounded by contrast in a non-calcified arterial segment, whereas thrombotic occlusion usually appears as a clot superimposed on a heavily calcified occlusive lesion. 3 Presence of synchronous embolism, atrial fibrillation, previous embolism and no or inadequate anticoagulation therapy at onset of ALI suggested embolism. 7
Definitions
ALI is defined as a symptom duration of less than 2 weeks. 6 The Rutherford classification is defined as resting pain (I), sensory loss (IIa), motor deficit (IIb) or irreversible damage with paralysis (III). 1 Major amputation was defined as amputation above the ankle. Ischaemic heart disease was defined as previous myocardial infarction, angina, coronary artery bypass grafting or percutaneous transluminal coronary angioplasty. Cerebrovascular disease included history of cerebral infarction, haemorrhage or transient ischaemic attack. Diabetes mellitus included dietary, oral or insulin treatment. Charlson Comorbidity Index (CCI) was calculated according to www.mdcalc.com/calc/3917/charlson-comorbidity-index. A CCI ≥5 is interpreted as severe comorbidity.
Ethics
This study has ethical clearance from the Swedish Ethical Review Authority (Dnr §2020–00764).
Statistical methods
The statistical analyses were carried out in Statistical Package for the Social Sciences (SPSS) Statistics version 26 (IBM, Armonk, NY, USA). Pearson’s chi-square test or Fisher’s exact test were used to analyse differences in frequencies between groups. Continuous variables were presented as a median together with interquartile range (IQR). Baseline factors associated (p < .1) with revascularization, combined major amputation/mortality or mortality at 1 year in the uni-variable analysis were entered the multi-variable binary logistic regression analysis and expressed in Odds ratios (OR) with 95% confidence intervals (CI). The inter-rater reliability between the first and second rater of EVIF category I was evaluated with intra-class correlation (ICC) with 95% CI and a value > 0.7 was regarded as satisfactory. 8 The level of statistical significance was p < .05.
Results
Patient characteristics
Patient and limb characteristics.
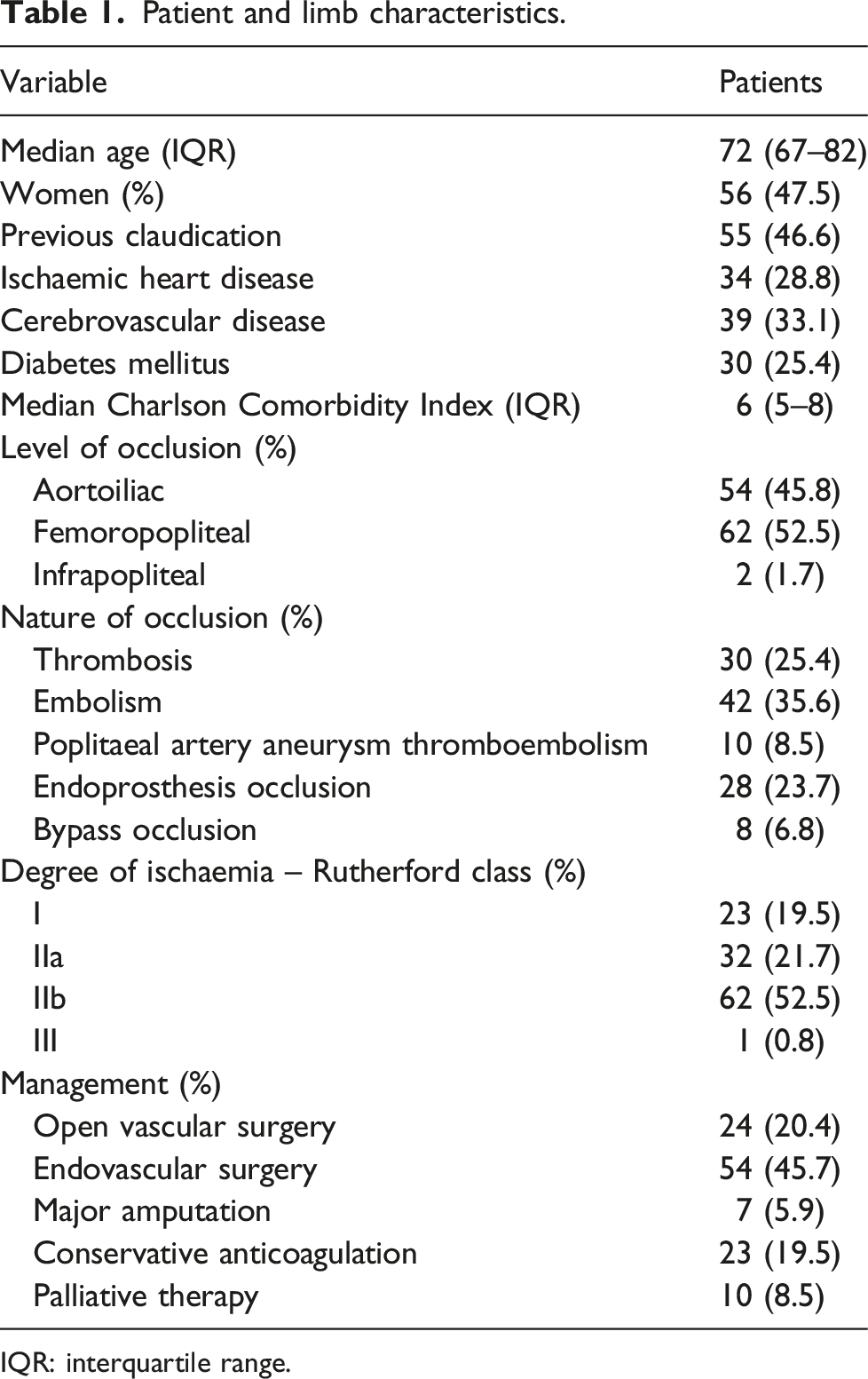
IQR: interquartile range.
Extravascular incidental findings
In total, 331 EVIFs were found in the 118 patients with ALI. Three patients had no EVIFs. There were 46 EVIFs of immediate clinical relevance (Category I) in 34 (29%) patients. Twenty-four patients had one Category I finding, eight patients had two Category II findings and two patients had three Category I findings. There were 128 EVIFs of potential clinical relevance (Category II) in 65 (55%) patients and 157 EVIFs of no clinical relevance (Category III) in 36 (31%) patients.
Category I extravascular incidental findings
Category I extravascular incidental findings in 118 patients.
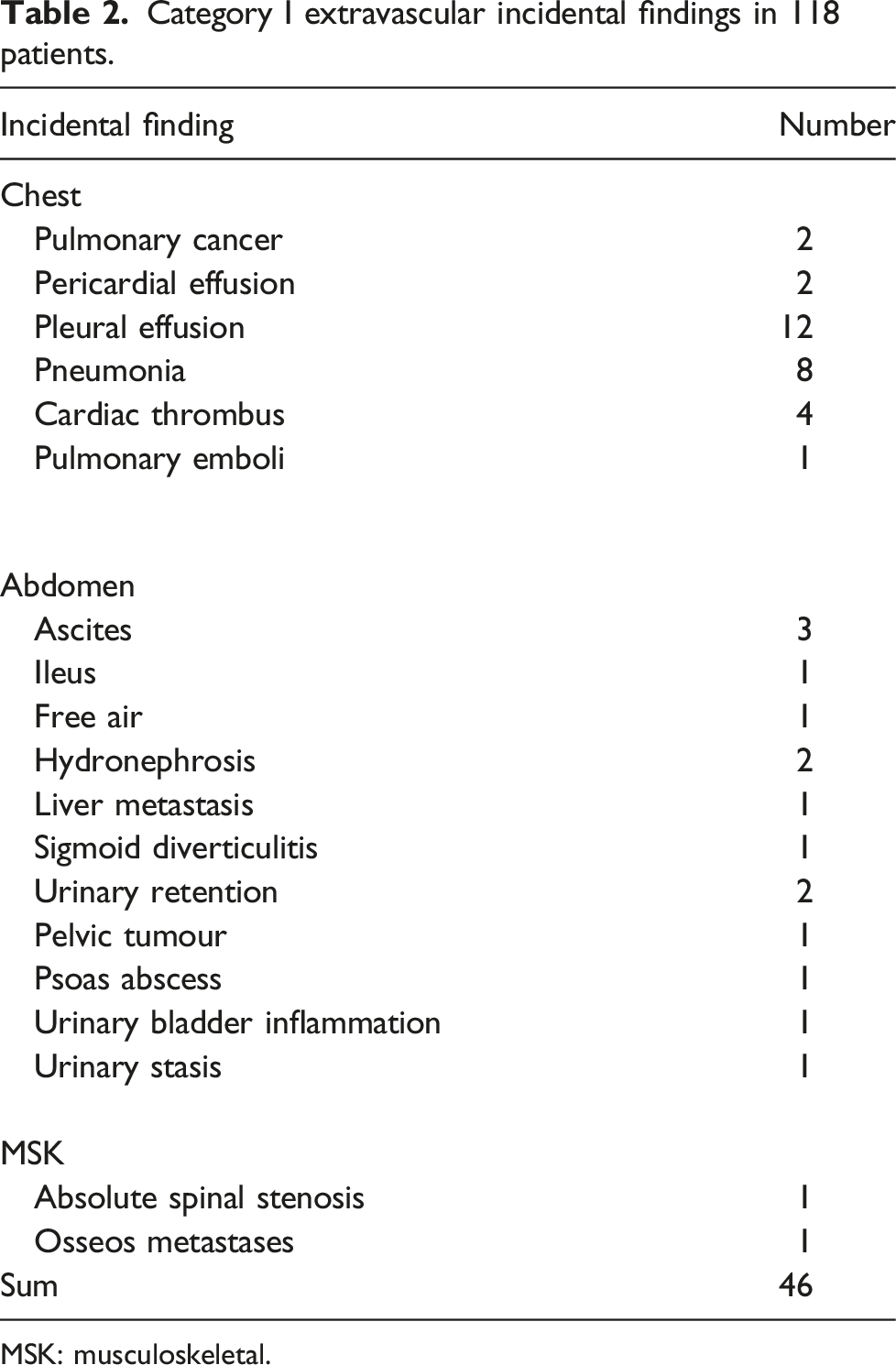
MSK: musculoskeletal.
Factors associated with emergency revascularization in patients with ALI
Factors associated with emergency revascularization in patients with acute lower limb ischaemia evaluated by computed tomography angiography.
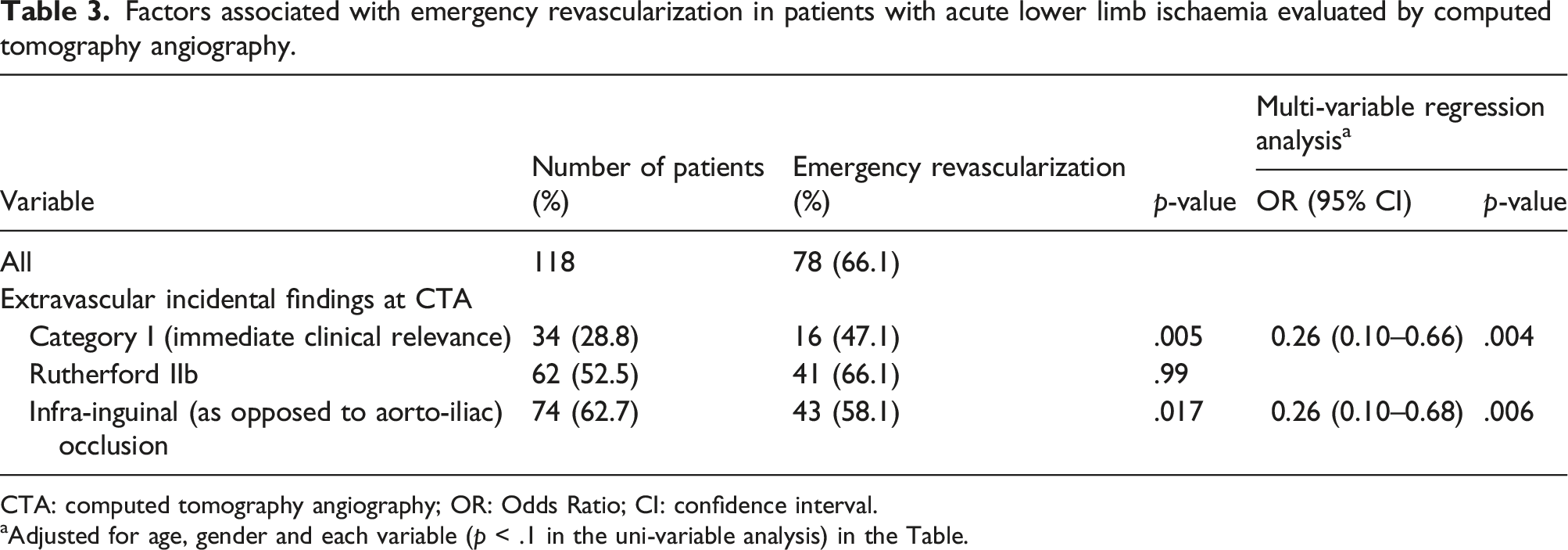
CTA: computed tomography angiography; OR: Odds Ratio; CI: confidence interval.
aAdjusted for age, gender and each variable (p < .1 in the uni-variable analysis) in the Table.
Factors associated with outcome at 1 year in patients with ALI
Factors associated with major amputation/mortality at 1 year in patients with acute lower limb ischaemia evaluated by computed tomography angiography.
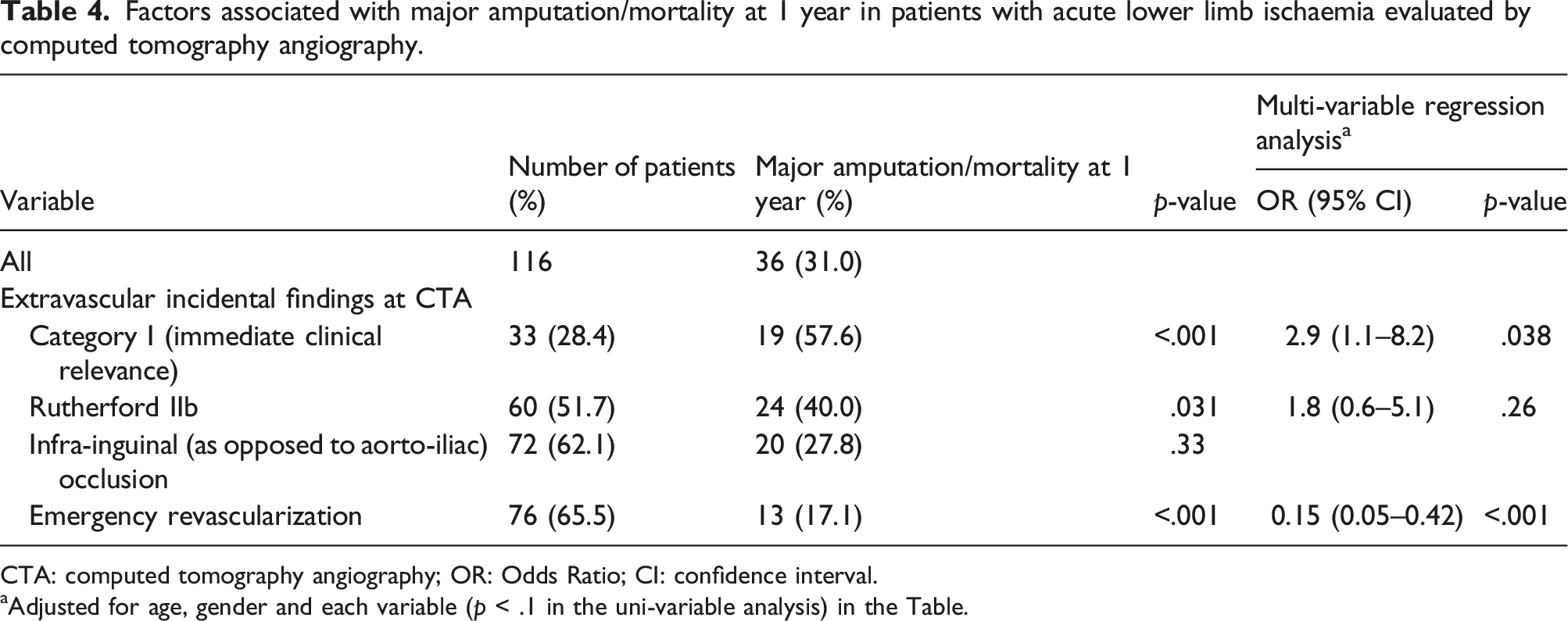
CTA: computed tomography angiography; OR: Odds Ratio; CI: confidence interval.
aAdjusted for age, gender and each variable (p < .1 in the uni-variable analysis) in the Table.
Discussion
The present study showed that EVIFs of immediate clinical relevance was found in almost 1/3 of patients with ALI undergoing CTA. These findings in the study cohort had a great impact on management in terms of lower surgical or endovascular revascularization rate and lower amputation-free survival at 1 year after adjusted analyses. Interestingly, presence of Rutherford IIb at admission was not associated with amputation-free survival at 1 year in the adjusted analysis. Compared to the present study, similar proportion of EVIFs of immediate clinical relevance including cancer has been reported previously, 5 but the associations between EVIFs and surgical revascularization, or between EVIFs and major amputation/mortality at 1 year are novel data.
The most common category I EVIF was pleural effusion. This finding will not only compromise the cardio-pulmonary physiological reserve further among these patients with severe illness, of which some may need to undergo emergency surgery under general anaesthesia, but also be a negative prognostic factor since 1/3 of these patients will have congestive heart failure and 10% will have malignancy. 9 The presence of concomitant pneumonia among these study patients was clinically undetected at the emergency department, and the accurate 10 detection of pneumonia made the clinicians initiate immediate treatment with proper antibiotics. The presence of cardiac thrombus 11 strongly suggested an embolic occlusion as a cause for ALI. This finding is indeed a very strong indicator for careful perioperative anticoagulation and lifelong anticoagulation therapy postoperative to prevent re-embolization. The excess accumulation of intra-peritoneal fluid, ascites, is an important marker for a significant underlying disease. Ascites may be caused by an inflammatory or malignant process within the peritoneal cavity or secondary to cardiac, hepatic and renal decompensation. 12 Knowledge of cancer diagnosis will be of great importance in the decision-making process for clinicians. The prognosis for both limb salvage and life will be inferior to non-cancer patients. 13 If it is decided to perform an emergency revascularization, knowledge of the presence of cancer will direct the surgeon towards open vascular surgery due to fear of hemorrhagic complications during thrombolysis. 14
The retrospective design without a preset defined data base ahead of the study is a limitation. The low sample size increases risk of type II statistical error after multi-variable adjustments. By using only imaging with contrast in the arterial phase, parenchymal assessment and hypo vascular lesions may be missed. The very good inter-rater availability of EVIFs of immediate clinical relevance between the two CTA raters, and evaluation of the consequences of these EVIFs in patients with ALI were major strengths of the study. The high risk of major amputation and mortality at 1 year in patients with ALI implicates that double-reading15,16 of CTA in suspected patients should be conducted to reduce the risk of missing immediate clinically relevant findings. The results of the present study should be externally valid for high-income countries with possibilities to perform CTA around the clock.
In conclusion, EVIFs of immediate clinical relevance are very common in emergency CTA in patients with ALI, and these EVIFs were associated with both reduced emergency revascularization and amputation-free survival at 1 year. Therefore, it is important to evaluate EVIFs in CTA carefully even if clinical focus is on vascular evaluation.
Supplemental Material
Supplemental Material - Extravascular incidental findings in computed tomography angiography are associated with lower amputation-free survival in patients with acute lower limb ischemia
Supplementary Material for Extravascular incidental findings in computed tomography angiography are associated with lower amputation-free survival in patients with acute lower limb ischaemia by Andrea Kulezic, Stefan Acosta, Olle Ekberg, and Leena Lehti in Vascular.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.