
Abstract
Background
Percutaneous Inferior Venacava (IVC) filter retrieval can be challenging when the filter is grossly angulated, embedded in the wall or penetrates through the IVC. When conventional filter removal technique fails, the use of advanced retrieval techniques often improves the chances of percutaneous filter retrieval. These techniques, however, are associated with a high rate of complications.
Methods
We report a case of 26-year-old female who had IVC filter placed on postpartum day 4. Attempted percutaneous filter retrieval 3 weeks later with loop snare technique and endobronchial forceps assisted filter removal technique resulted in gross filter deformity, malposition, and IVC perforation.
Result
Open IVC filter removal was performed with midline laparotomy and cavotomy with lateral venorrhapy. The deformed filter along with adherent thrombus was completely removed. The patient had an uneventful recovery with no immediate or long-term complications.
Conclusion
Use of advanced endovascular IVC filter retrieval techniques could result in serious complications like filter fracture, migration and IVC perforation. Since excessive tilt of the filter at the time of placement often results in difficult retrieval, it is important to ensure proper deployment of the filter with minimal tilt. If encountered with excessively tilted or embedded filter, one should refrain from excessive manipulation of the filter and consider open filter removal.
Introduction
When conventional percutaneous filter removal technique fails, advanced techniques can be utilized to improve the chances of retrieval. These techniques, however, are associated with high rates of complications like Inferior Venacava (IVC) perforation, IVC thrombosis and filter fracture. 1 We report a case where percutaneous filter retrieval attempt utilizing advanced technique resulted in gross malposition of the filter with IVC perforation and thrombosis. The deformed filter along with thrombus was successfully removed by midline laparotomy and cavotomy. The patient consented to the publication of anonymized case details and images.
Case report
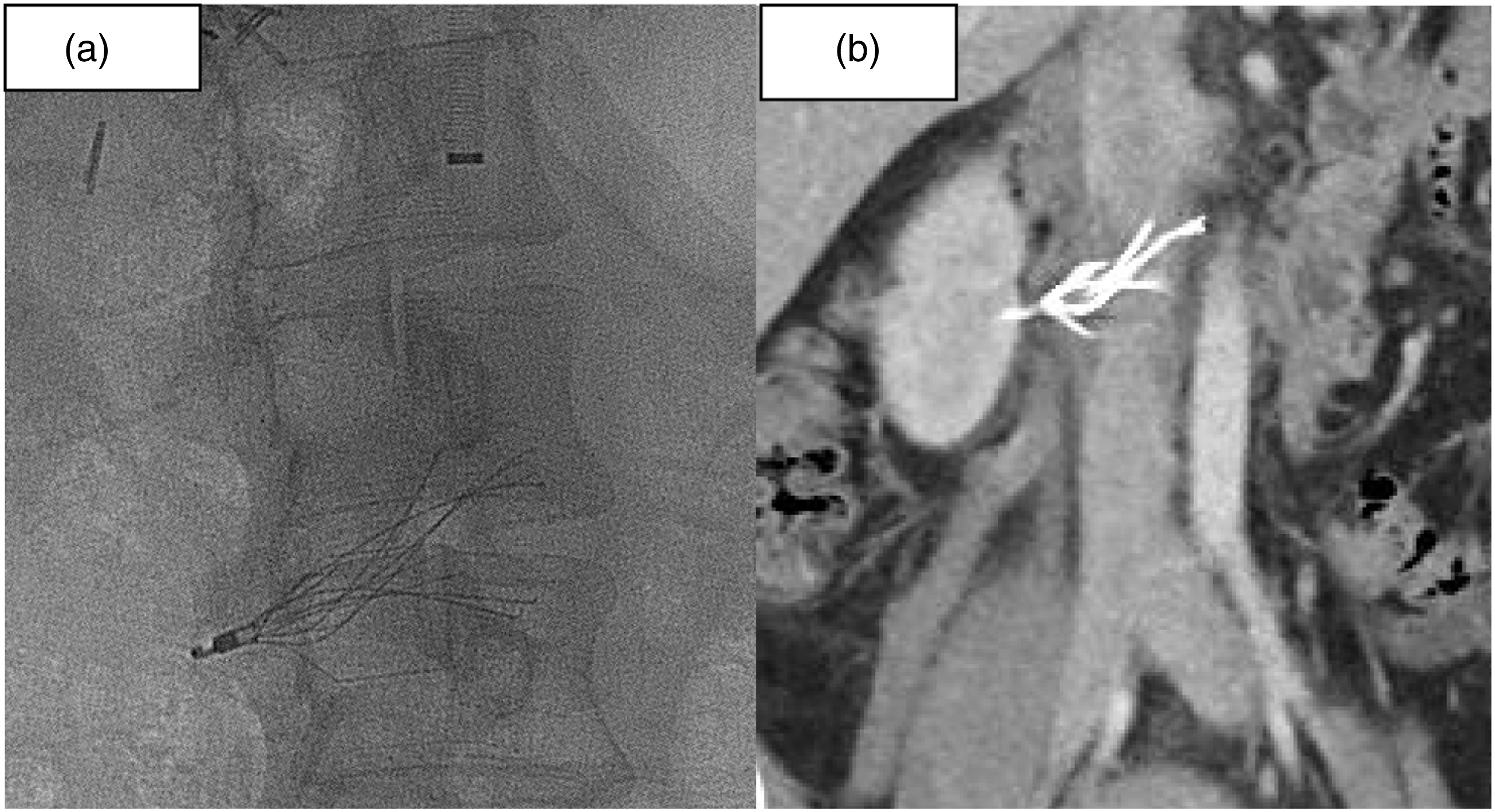
A 26 years old female had an IVC filter placed on postpartum day 4, due to contraindication for anticoagulation after diagnosis of deep vein thrombosis. Denali IVC filter (Bard Peripheral Vascular, Inc., Tempe, Arizona) was implanted at the time without any incident. (Figure 1(a)). She presented approximately 3 weeks later for percutaneous filter removal. At the time, percutaneous IVC filter removal was attempted through right Jugular vein access. Due to significant tilt of the filter, conventional snare capture technique was unsuccessful. (Figure 1(b)). Advanced filter retrieval maneuver was carried out utilizing loop snare technique and endobronchial forceps assisted filter removal technique. Persistent intervention resulted in further tilting of the filter and the snare got entangled within the filter struts. At this point femoral venous access was obtained and the snare was released by catheter deflection. By this time, the filter had become significantly deformed and was lying transverse in the IVC (Figure 2(a)). Procedure was aborted and vascular surgery was consulted for further management. Upon reviewing the venography, we felt that this filter would not be suitable for percutaneous removal as the retrieval hook was completely outside of IVC. CT venography was performed which demonstrated significant IVC perforation, filter deformity and large amount of thrombus within and around the filter but no active extravasation. (Figure 2(b)). At this point, a decision was made to proceed with open laparotomy and removal of filter. Final angiographic picture after implantation of the filter (Figure 1(a)) shows significant right tilt. IVC venography prior to retrieval attempt (Figure 1(b)) shows persistent tilt of the filter. Note that the hook of the filter (arrow) is completely outside of the lumen. Grossly deformed filter as seen on fluoroscopy (Figure 2(a)). CT venography (Figure 2(b)) shows significant portion of the filter outside of IVC.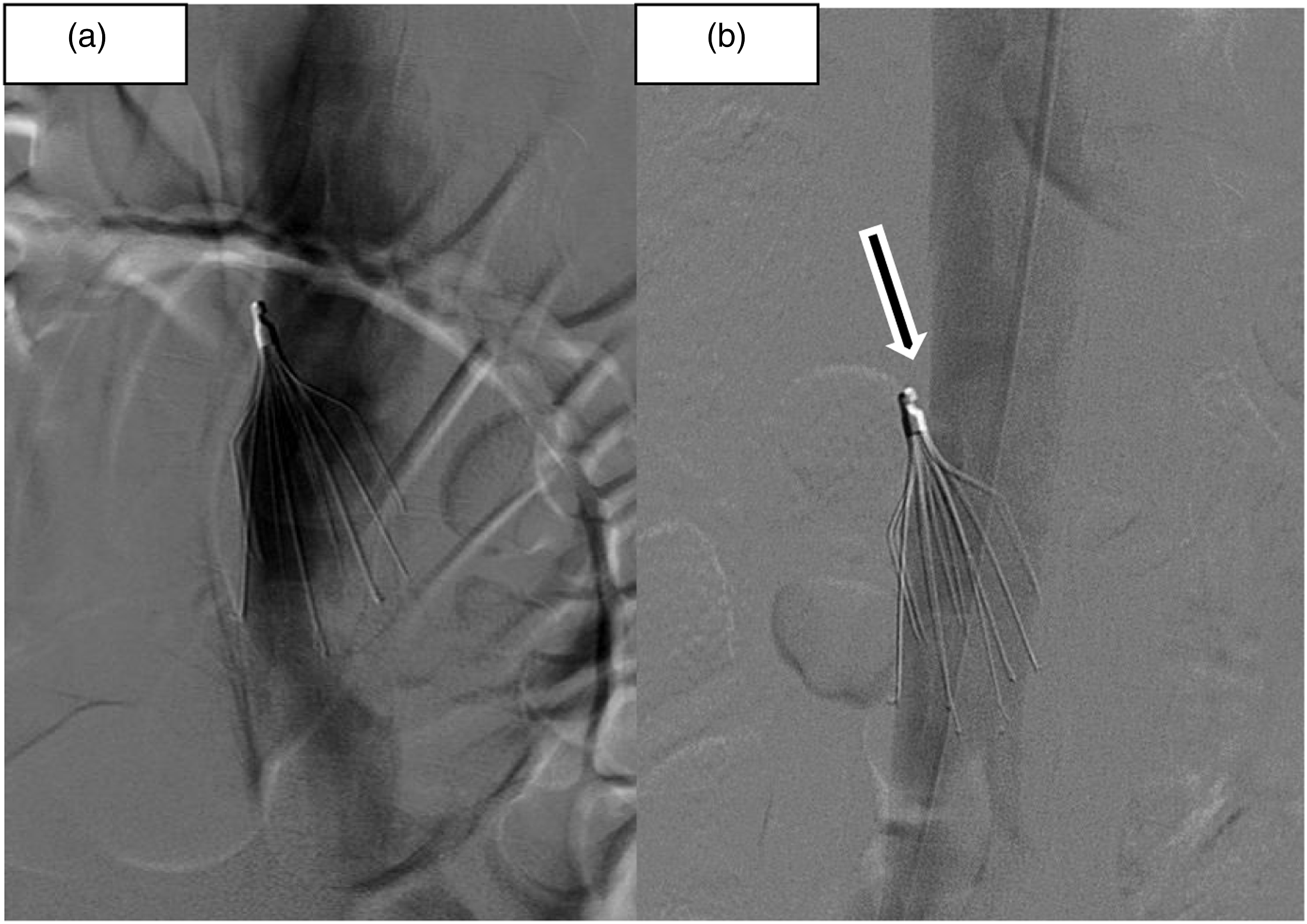
After obtaining informed consent, open removal of IVC filter was performed under general anesthesia. Midline laparotomy and extended Kocher’s maneuver were carried out to expose the Infrarenal IVC. Circumferential control of the IVC above and below the filter was obtained. Filter struts penetrating the retroperitoneum were divided flush to the wall of IVC utilizing wire cutter. A longitudinal cavotomy was performed. Filter was grasped at its collar from within IVC lumen and pulled back into the lumen. Filter was finally removed through the cavotomy after freeing all the struts from the IVC wall. This segment of the IVC contained a large amount of thrombus as visualized on CT scan. The thrombus was completely removed under direct visualization. Inferior Venacava was subsequently closed with lateral venorrhaphy utilizing 3/0 polypropylene suture. Hemostasis was secured and the abdomen was closed. The postoperative period was uneventful, and the patient was discharged on postoperative day 5. The patient does not have any complaints related to surgery in a 4-year follow-up period.
Discussion
Successful percutaneous retrieval of retrievable filters by conventional technique is somewhere between 70 and 90%.1,2 The major determinants of whether the filter can be successfully removed by percutaneous technique remains the duration since implantation and the alignment of filter in relation to IVC. In general, longer dwell time poses the risk of difficulty at percutaneous retrieval. With increasing dwell time, parts of the filter become embedded within the wall of IVC. Occasionally the filter struts may perforate through the IVC into the retroperitoneum. Once the top retrieval hook gets embedded within the wall of the IVC, the filter can no longer be removed by conventional endovascular techniques.3,4
If the filter removal is unsuccessful by conventional technique, advanced endovascular techniques can be utilized to increase the chances of percutaneous retrieval. Advanced filter retrieval techniques like loop snare technique, use of endobronchial forceps and balloon repositioning technique etc. significantly increase the chance of filter retrieval.
5
These techniques, however, are associated with increased incidence of complications. Commonly encountered complications include IVC perforation, retroperitoneal hemorrhage, filter fracture and IVC thrombosis. (Figures 3 and 4). Intraoperative picture showing filter hook (White arrow) and ends of filter struts (black arrows) outside of IVC. Appearance of the filter after removal. Note grossly deformed filter tines.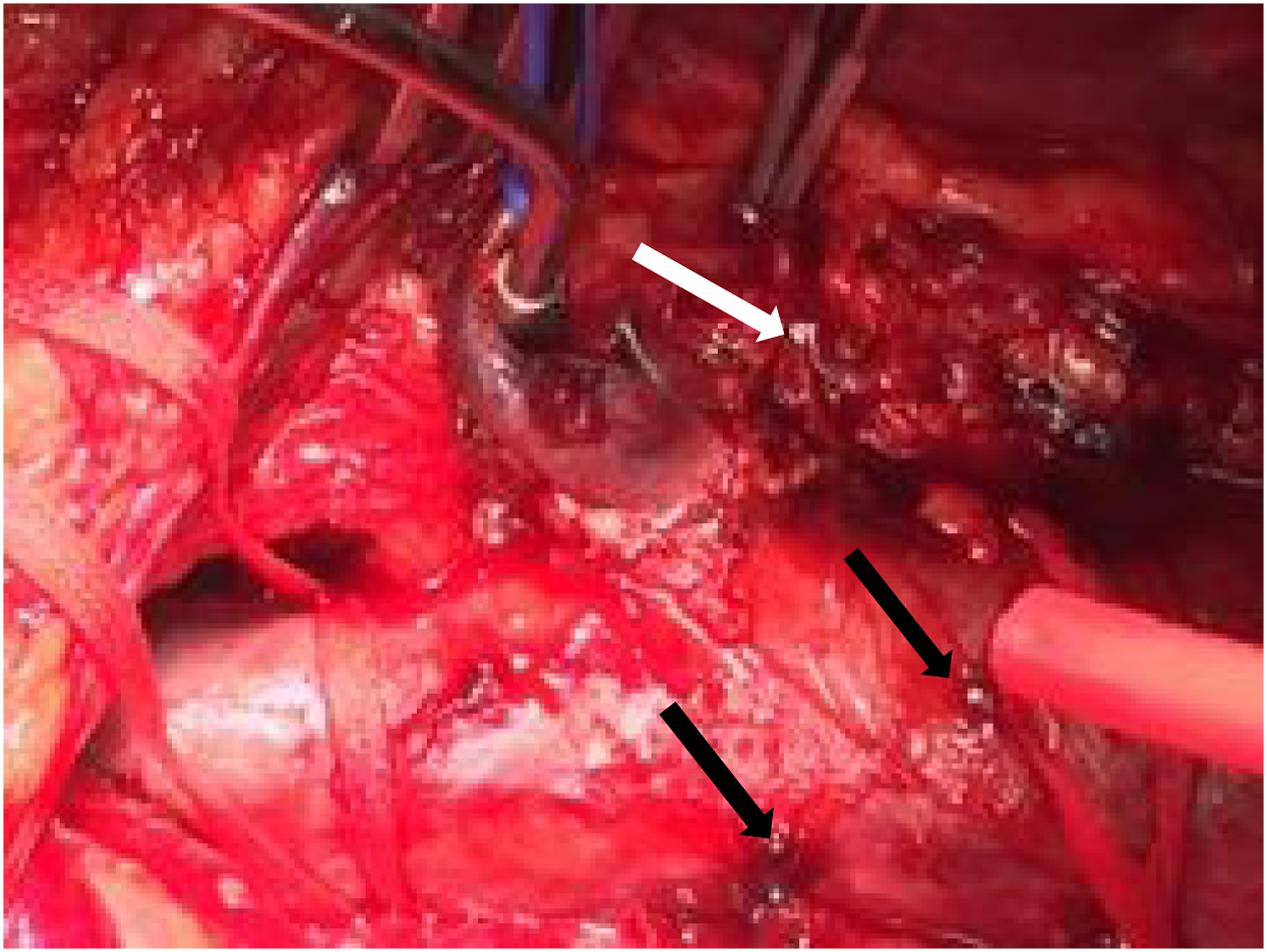

Al-Hakim et al. et al. 1 reported that the rate of complications associated with filter retrievals that required advanced technique was significantly higher than seen with routine technique (5.3% vs 0.4%; p < .05). Excessive manipulation and forceful traction could easily lead to IVC perforation, filter fragmentation or filter malposition. One of the difficulties with these procedures is the understanding of how much force is too much. Every interventionalist has their own threshold of how much force they are willing to exert depending upon their level of competence and experience. It cannot be overemphasized that only experienced endovascular interventionalist should be performing these procedures. Also, one must ensure that there is adequate backup available, and the facility is well equipped to deal with these complications.
Open retrieval of IVC filter is generally reserved for symptomatic patients with filter related complications when percutaneous attempt is unsuccessful or not feasible. Charlton-Ouw et al. 6 recently reported a case series of seven open IVC filter removal. Of the 7 cases, only one patient required open removal due to complication from percutaneous retrieval attempt.
In our case, we had a young patient left behind with grossly deformed filter along with IVC perforation and large amount of thrombus. Leaving the filter was not an option because of the high likelihood of long-term complications. Following the unsuccessful percutaneous retrieval, she continued to have continuous back pain which prompted us to proceed with surgery urgently.
Various techniques of open IVC filter removal have been defined in the literature. Though all open retrieval require laparotomy, the major modification in technique is mostly related to the extent of cavotomy and need for caval clamping. Caval clamping and longitudinal cavotomy offer the best accessibility to the filter. Filter removal by first collapsing it and removing it through stab venotomy has been described by Rana et al. 7 Another technique of mini cavotomy has been described where the filter is captured into a sheath via direct access to the hook and the mini cavotomy is closed by tying the preplaced purse string suture. 8 This technique of mini cavotomy has various advantages like decreased blood loss, faster procedure and no need for excessive caval dissection. There is also a decreased risk of caval stenosis compared to the other techniques requiring long cavotomy and repair. Mini cavotomy technique, however, is not suitable for cases where there is large amount of thrombus within the cava which requires direct removal. It is also not suitable when dealing with retained birds nest filter. During extraction of the filter, care should be taken to avoid IVC injury. Sharp hooks at the end of filter tines may lacerate the cava as it is pulled out from within. We did not encounter any injury or bleeding as we had cut the ends of the tines that had penetrated out of IVC. Qato et al. 9 recently reported six cases of open filter removal where four techniques that were used: longitudinal venotomy with primary repair, patch venoplasty, removal of extracaval struts and securing of the IVC filter struts, and snare technique of an extraluminal hook.
Potential causes of filter tilt and their remedy.

Conclusion
Utilization of advanced endovascular filter retrieval technique translates to improved filter retrieval rates; however, complications are more likely after these attempts. Occasionally it could lead to major complications like IVC perforation, filter fracture and IVC thrombosis. Interventionalist should be careful to avoid every one of these adverse outcomes. They should also ensure that there is adequate surgical backup at their institution in case they encounter such problems.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.