
Abstract

Keywords
Dear Editor,
Recently, Mouawad NJ commented on the adequacy of the isolated profunda femoris revascularization in critical limb ischemia. Isolated profundaplasty refers to restoration of unimpaired inflow to the stem of the profunda femoris artery (PFA) and this branches with endovascular techniques having further evolved our treatment options.1,2 Yet, the clinical results of this procedure remain diverse, with most authors reserving its role in claudicants but not in cases of tissue loss, while its treatment role in cases with rest pain remains dubious and controversial.3–5
The selection of the revascularization of the PFA and its prognostic value could be enhanced by implementing the forgotten and underappreciated tool of the profunda-popliteal collateral index (PPCI) which evaluates the competence of the profunda collateral index (Figure 1). The PPCI is expressed as the difference between the above- and below-knee systolic pressure divided by the above-knee pressure.
6
It is indicated that a PPCI value of 0.3 is a good predictor for the adequacy of collateral pathways from the PFA to the crural arteries.
7
The high values of PPCI ≥0.45 correspond to poor collaterization and are associated with profundaplasty failure.
6
Collateral network between the profunda femoris artery and the popliteal artery (magnetic resonance angiography).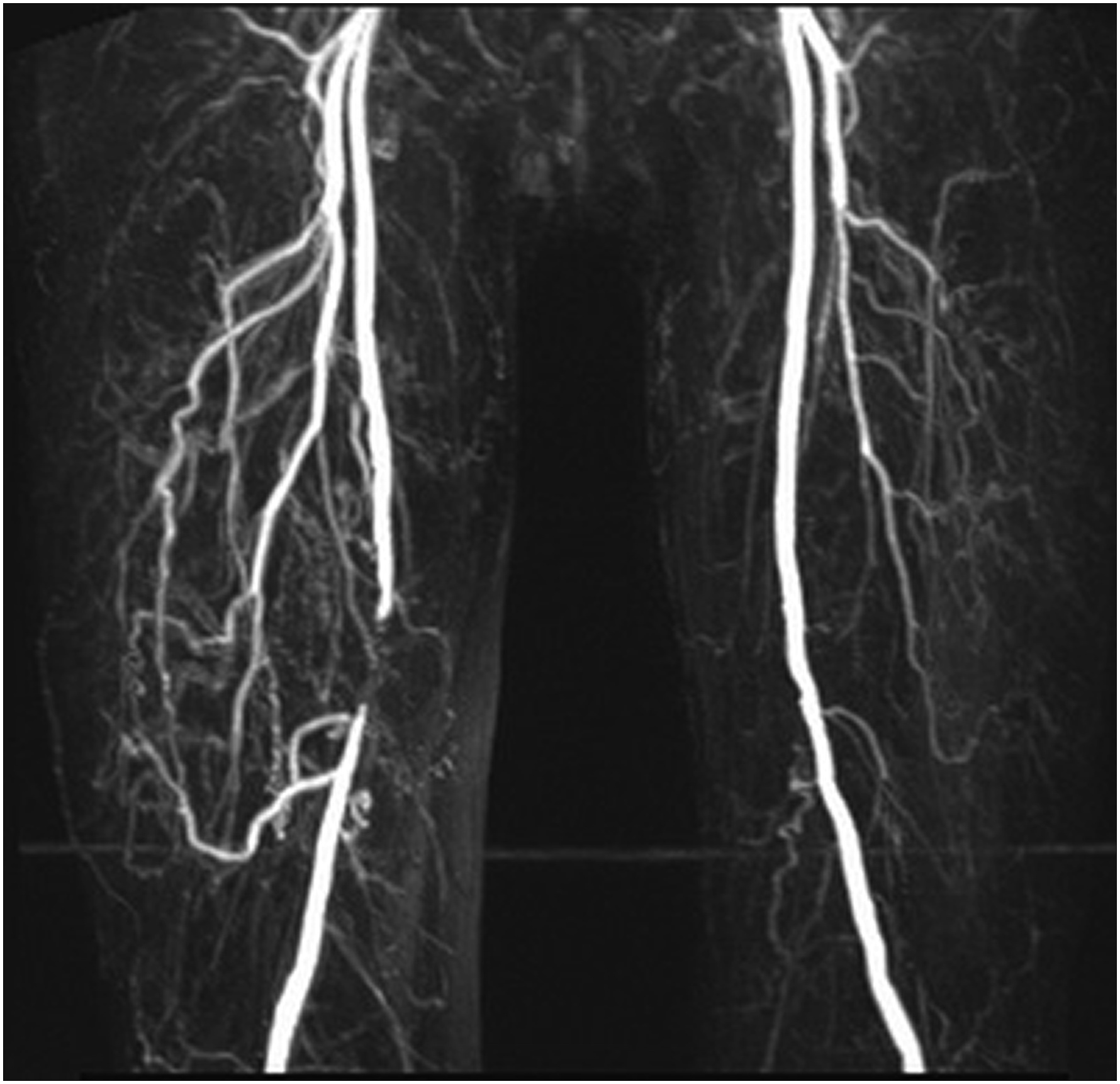
Anatomical cadeveric studies have classified six types of collateral network between the PFA and the popliteal or crural vessels. 8 Admittedly, only 19% of the PFA collaterals ended in the popliteal artery while one-third of them in the distal adductor canal. 8 Therefore, the adequacy of the PFA collaterals perfused via profundoplasty varies markedly; yet, these could be evaluated by a thorough angiography.
Interestingly, one would anticipate the clinical success of isolated profundaplasty to depend greatly on tibial perfusion, yet the tibial gradient index (i.e. below-knee pressure-ankle pressure/below-knee pressure) expressing the adequacy of the tibial outflow network did not correspond to the operative results, according to Boren et al., 6 preserving a unique significance for PPCI as a predictive tool and underling that it is the adequacy of the profunda-popliteal collateral network that mostly determines the success of isolated profundaplasty.
The postoperative evaluation of distal Doppler signals (dorsalis pedis or posterior tibial artery) to evaluate the ankle-brachial index comprises common practice for vascular surgeons (Figure 2(a)); yet, in our experience, the early postoperative detection of postoperative Doppler signal at the lateral aspect of the thigh close to the knee is suggested as an encouraging test for hemodynamic and clinical improvement for the limb, empirically related to adequacy of the collaterals for recession of rest pain and no further deterioration of any ischemic toe lesions but not for wound healing, the latter demanding an optimal level of distal perfusion. The location of interest for these bridging branches extending distally to the second perforating branch of PFA is detected laterally above the knee in the groove between the biceps femoris and the vastus lateralis muscle (Figure 2(b)). Some hand-held Doppler devices can even record and assess the flow waveform (Figure 2(c)). In such cases, we believe that one could assess immediately postoperatively whether the profundaplasty could be promising and sufficient or an additional revascularization procedure would be inevitable. (a) Examination of the dorsalis pedis artery with a hand-held Doppler device. (b) Detection of Doppler signal in the lateral thigh in the groove between the biceps femoris and the vastus lateralis muscle. (c) Recording of flow waveform in the collateral network between the profunda femoris artery and the popliteal artery.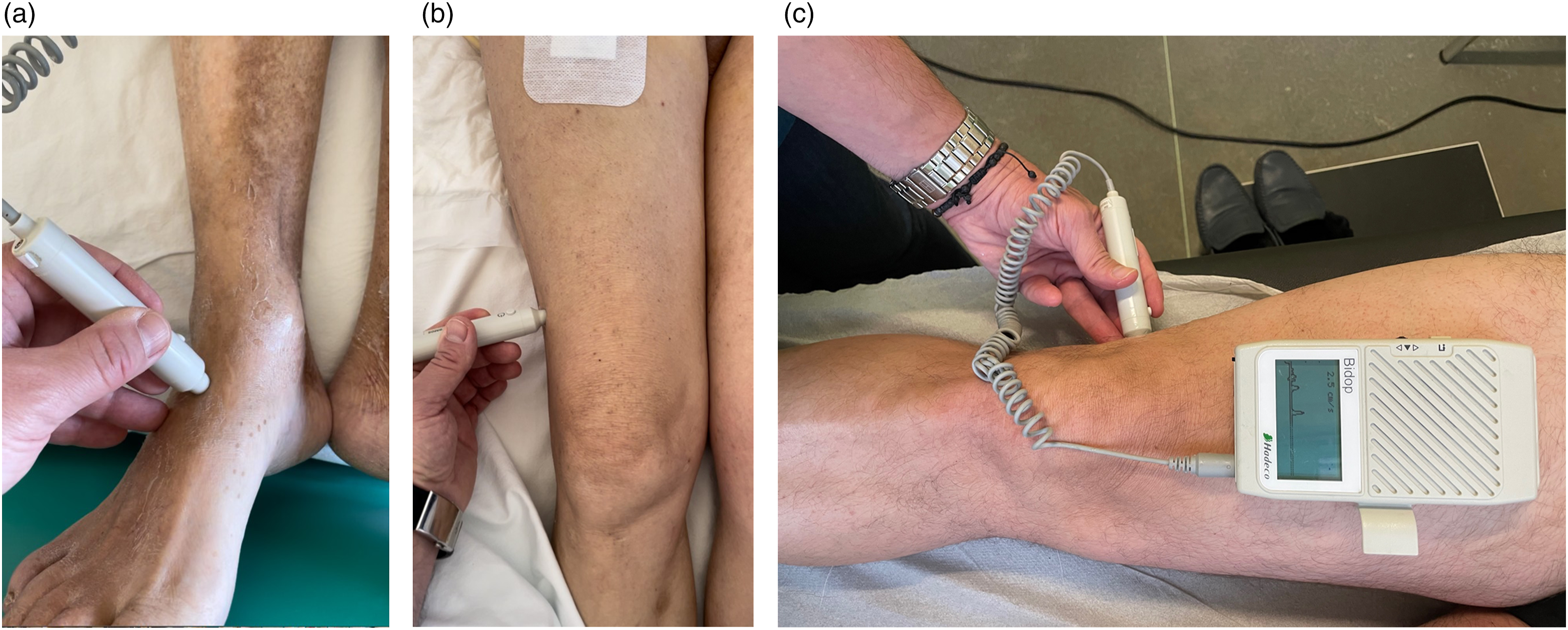
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.