
Abstract
Introduction
One of the most important problems for patients undergoing hemodialysis due to chronic renal failure is the need for a long-lasting vascular access. The patency of vascular access is affected by many factors. Factors related to surgery are also among these factors. No-touch techniques theoretically and practically prevent endothelial damage due to minimal contact on vascular structures. It is a well-known fact that surgeries performed with these methods also increase long-term survival.
Methods
Patients who underwent distal radiocephalic arteriovenous fistula (AVF) surgery for the first time between 2017 and 2021 were included in our study. The groups, whose cephalic veins were inflated conventionally and not inflated, were compared in a prospective randomized manner.
Results
There was a significant difference between both groups in terms of failure and patency rates, which is one of the study endpoints (p = 0.012). The fact that the patency period is long, and the failure rate is low stands out as the superiority of the fully no-touch technique in AVF surgery. On the other hand, no significant difference was observed in terms of failure to maturation and fistula maturation time.
Conclusions
Fully no-touch technique in AVF surgery should be considered primarily in suitable patients due to its long patency time and low failure rate.
Introduction
CRF is one of the most important public health problems today. Every year, millions of people need hemodialysis due to kidney failure. 1 Although the patency of AVFs varies from person to person, many factors that affect this patency interact with each other in a complex way. 2 Each of the factors, such as preoperative preparations, surgical techniques, adjuvant treatments and follow-up protocols, can have very effective results on AVF patency. The vascular accesses required for hemodialysis are limited. Therefore, the AVFs created must both allow for effective hemodialysis and must be durable for a long time. Almost every vascular surgeon tends to inflate the vein grafts used for fistula, both out of necessity and habit, when creating an AVF. This study prospectively and randomly investigated whether there was a difference between the inflating or non-inflating of the cephalic vein in distal radiocephalic AVFs created for the first time in terms of maturation time, patency time, and failure to mature of the fistula.
Methods
The study was started after the decision of the ethics committee of Sivas Cumhuriyet University. Our study included 57 patients who underwent distal end-to-side radiocephalic arteriovenous fistula operation for the first time between November 2017 and March 2021 in the department of cardiovascular surgery at Sivas Cumhuriyet University. Written informed consent forms were obtained from all patients. In line with the predetermined randomization criteria, the cephalic veins of 28 patients were not inflated, while the cephalic veins of 29 patients were inflated by the same surgeon using the same technique. In the cephalic vein inflated group, two patients were excluded from the study because of early death, and one patient was excluded because of early renal transplantation. The study was completed with a total of 54 patients, including 28 patients in the group whose cephalic veins were not inflated, and 26 patients in the group whose cephalic veins were inflated. The study endpoints were evaluated as failure to mature, failure, patency, and exitus. All the patients consulted the adult nephrology department and were undergoing hemodialysis via a catheter. They had started hemodialysis on their last admission and had AVF requirements for permanent vascular access.
Patient selection
All the patients were older than 18 years and those with positive Allen’s test were included in the study. The nondominant arms of the patients were preferred for the operation. Patients who had been treated with the radial artery grafting due to aortocoronary bypass were also not included in the study. Patients with radial artery or cephalic vein diameter 1 mm or less in intraoperative measurements were excluded from the study. The researchers performed conventional surgery for this patient group and continued the procedure by inflating the cephalic vein. Patients with diameter over 1 mm (mm) but had calcification in the radial artery were included in the study. After the intraoperative evaluation, a researcher opened one of the predetermined envelopes, and the researchers decided whether to inflate the cephalic vein.
Operation technique
All patients were operated under local anesthesia after the operation conditions were met. After preparation of the cephalic vein and radial artery, 2500 units of heparin were administered. After heparin was administered and the appropriate activated clotting time (ACT) value (>200) was reached, end-to-side radiocephalic arteriovenous fistula was performed in all patients with 7.0 or 8.0 prolene. In both groups, all branches of the cephalic vein included in the surgical field were tied with silk sutures. In both groups, the size of the anastomosis was decided according to the diameter of the cephalic vein and dissection was performed. In the group in which the cephalic vein was inflated, dilatation was achieved by placing an appropriate branule inside the cephalic vein and applying pressure to the proximal part of the cephalic vein by injecting saline through a 5 mL (ml) syringe. All surgical procedures were performed by the same surgeon. Cephalic vein and radial artery measurements were obtained by measuring with a tape in the surgical field. The measurement areas were determined as the top of the anastomosis areas. When performing intraoperative measurement, the presence of vasospasm in the radial artery or cephalic vein was not considered. Although the vasospasm response varies due to individual differences, no antispasmodic treatment was applied because all patients underwent the same procedure. Obtaining a trill after the operation was considered a successful fistula.
Postoperative follow-up
If the patients had not been receiving acetylsalicylic acid (ASA) 100 mg treatment, the researchers added it to the treatment in the postoperative period. The researchers recommended continuing their current treatment for patients who were taking antiplatelet therapy (ASA, clopidogrel, etc.) for any reason. All patients were called to the cardiovascular surgery outpatient clinic on the 14th postoperative day for control examinations. The data of the fistulas of the patients were confirmed with the information received from the people in charge of the dialysis unit. The decision of the patients to undergo hemodialysis through the AVF was determined based on the condition of the surgical wound and whether the cephalic vein was technically suitable for needle entry. AVF flow measurement was not applied to any of the patients. In both groups, two patients were not followed up for a long period due to AVF failure to mature.
Statistical analysis
In the study, continuous variables were expressed as mean ± SD and categorical variables as frequency and percentage. SPSS 24 package statistical program (StataCorp LP, College Station, TX, USA) was used for descriptive statistics. Mann–Whitney U tests were used for pairwise comparisons and Kruskal–Wallis tests were used for more than two comparisons in nonparametric groups. A p-value of <0.05 was considered statistically significant.
Results
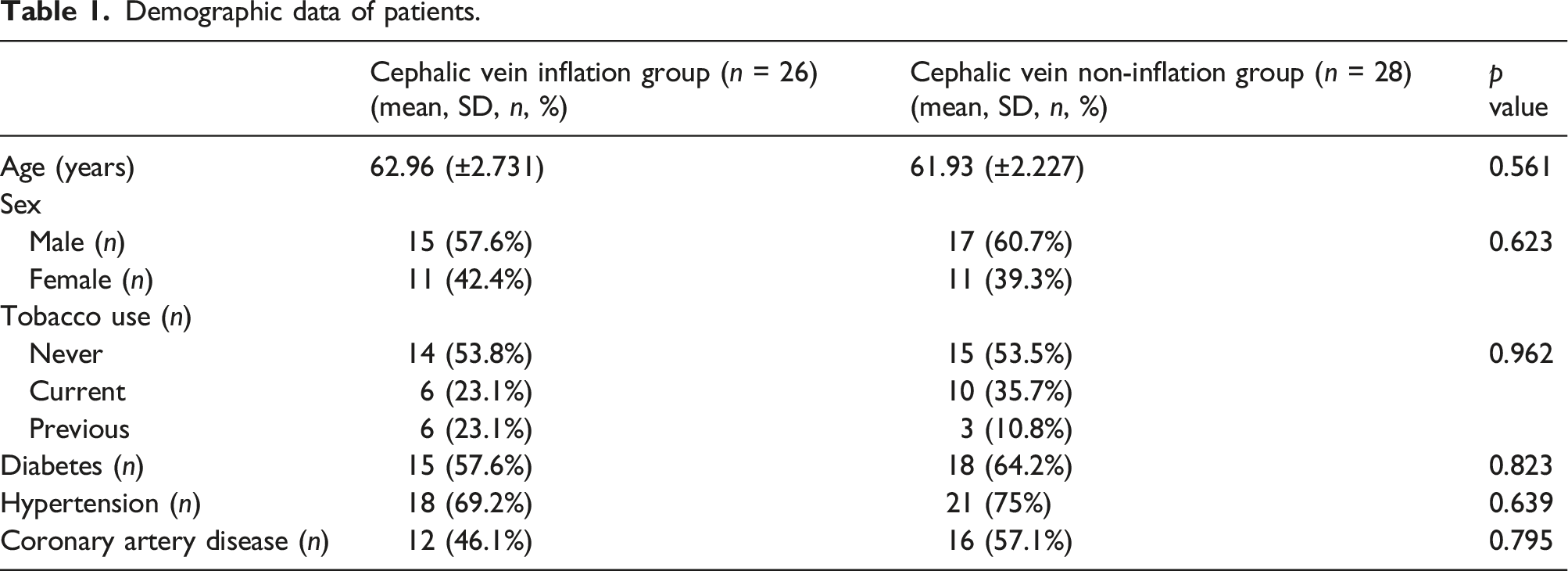
Demographic data of patients.
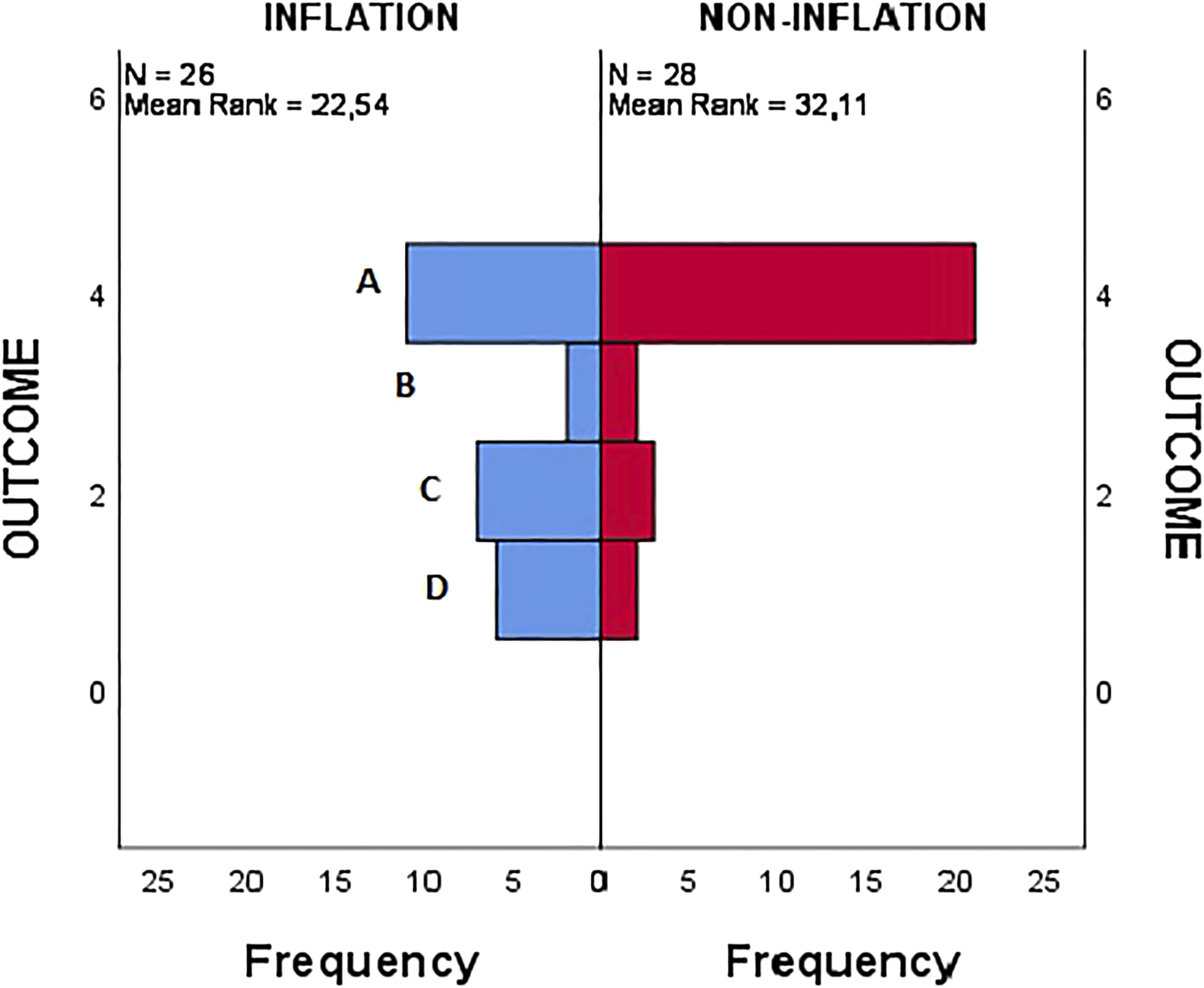
Results in terms of study endpoints. (A: Patency, B: Failure to mature, C: Failure, D: Death in follow-up).
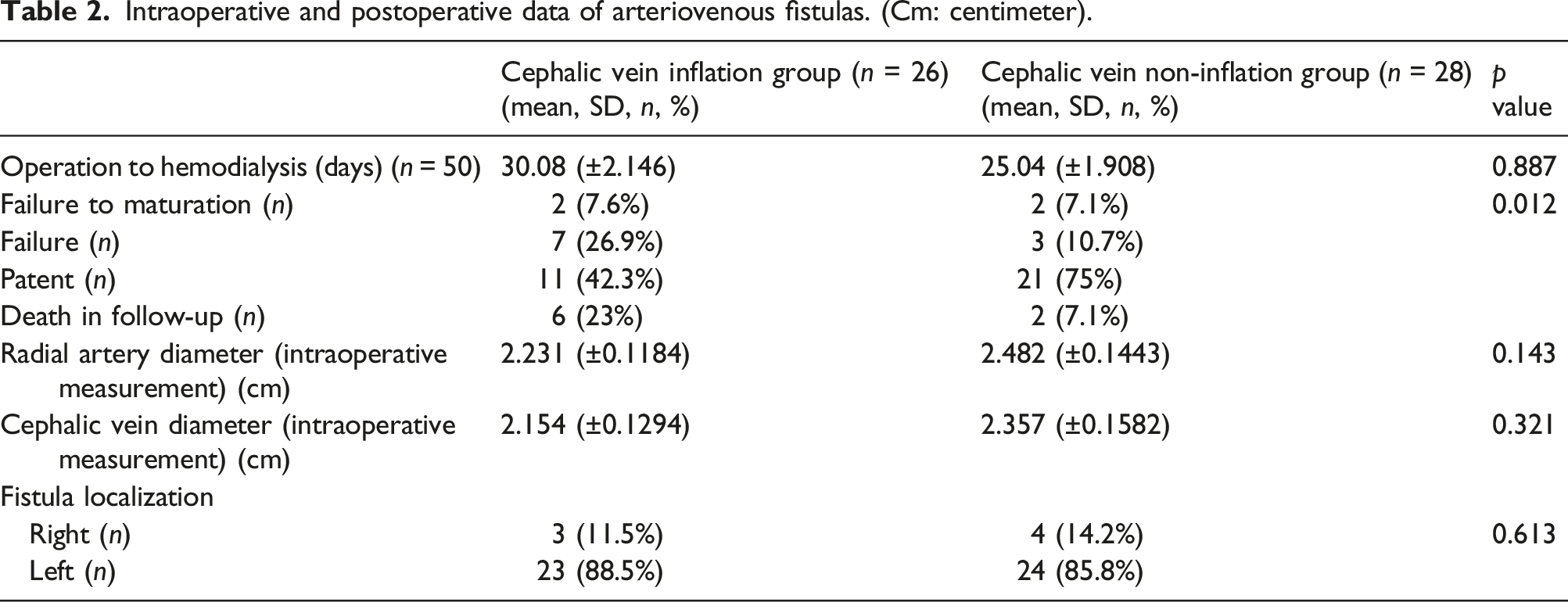
Intraoperative and postoperative data of arteriovenous fistulas. (Cm: centimeter).
Discussion
It is estimated that 5439 million people will receive renal replacement therapy in 2030.
3
One of the important factors affecting survival in such a large number of patient groups will be the duration of use of the AVF. The related literature on the given subject has reported that a mature fistula requires a blood flow of 500 mL/minute (ml/min
Radiocephalic AVFs are the first choice as a hemodialysis access route. However, it was observed that it had high primary failure and moderate patency rates in 1-year follow-ups. 6 Primary maturation rates vary in distal radiocephalic AVFs. In general, 28%–53% of fistulas in this region never mature and cannot be used.7–10 It is almost impossible to achieve a certain standardization in AVF studies. It is affected by many parameters such as patient-related factors, surgery-related factors, and dialysis-related factors. In the study of Jennings et al., 11 parameters such as vein diameter and arterial diameter were standardized and they concluded that the wrist was the first place of choice for AVF creation. Especially when creating a distal radiocephalic AV fistula, the possibility of fistula failure to maturation should be considered and a surgical site should be preferred accordingly. 12
One of the factors determining the distal radiocephalic AVF patency is the diameters of the radial artery and cephalic vein. The results of Wong et al’s 13 study on the preoperative colored doppler ultrasonography (CDU) measurements, indicated that the diameter of the radial artery and cephalic vein greater than 1.6 mm was associated with low early fistula failure. Female gender, forearm AVF, smaller arterial size, draining vein diameter of 2–3 mm, and protamine use were associated with early AVF thrombosis. 14 On the other hand, Linden et al. 15 demonstrated that venous diameter did not have a direct effect on AVF success, but venous distensibility was directly related. AVF failures are classified as early (1 week–1 month) and late failure (after 1 month). The role of aggressive neointimal hyperplasia in the early failure of AVFs has been demonstrated histopathologically. 16 As a result of exposure of venous structures to arterial pressure, neointimal hyperplasia is triggered. 17 Inflammation appears to be the central to the biology of AVF dysfunction, but important triggers still need to be uncovered. 18 Decreased blood flow in AVFs is a marker of early failure, and if the flow is <350 mL/min, insufficient blood flow surfaces. 19 On the other hand, blood flow <120 mL/min in intraoperative measurements can be considered as an indicator for early AVF failure. 20 It has been reported that one of the ways to prevent early AVF failure is related to the medical treatment given after surgery. Clopidogrel has been shown to reduce early AVF failure. 21 A vast amount of literature on the subject has demonstrated that performing AVF surgery after mapping venous and arterial structures with CDU before surgery increases the lifespan of the fistula and maturation develops earlier.22,23 This can be explained by direct imaging of intact vascular structures and performing surgery away from damaged/sick vascular tissues, and it is a great advantage.
It is known that a good preparation before surgery positively affects fistula maturation and prevents early failure. At the same time, many techniques applied during surgery affect the fistula patency. 24 The cephalic vein was inflated in the no-touch technique described by Hastaoğlu et al. 25 Branule inserted into the cephalic vein and saline given with pressure may cause endothelial damage and cannot be considered as fully no-touch technique. In our study, neither the radial artery nor the cephalic vein was treated, so it can be considered as a fully no-touch technique.
In fact, the patency period of AVFs depends on many factors, as well as the harmony of a multidisciplinary team from the beginning to the end of vascular access. This multidisciplinary team involves; nephrologits, surgeons, radiologists, dialysis nurses, and patients. 26 It is very difficult to conduct controlled studies for AVFs affected by many parameters. However, it is also possible to conduct studies in which some factors are equalized in terms of surgery. As in our study, it is obvious that the fully no-touch technique is open to promising developments in fistula patency rate.
Conclusion
The current study has observed that the patency rate increases, and the failure rate decreases in fully no-touch technique AVFs where the cephalic vein is not inflated. However, our study needs to be supported by multicenter and large population studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.