
Abstract
Background
Popliteal artery aneurysms (PAA) were traditionally treated by open repair (OR). Endovascular repair (ER) has become a new treatment strategy. The aim of this systemic review and meta-analysis was to evaluate and compare the current outcomes of OR and ER in the emergency treatment of PAA.
Methods
A systematic literature search of the PubMed/Medline database was carried out. Outcomes were 30-day mortality, morbidity, major amputation rate (30 days), major amputation rate (1 year), 1-year primary patency rate, 1-year secondary patency rate and 1-year survival. Additionally, we included clinical data of patients with popliteal aneurysms treated between 2009 and 2021 at the Martin-Luther University Halle-Wittenberg.
Results
We identified two cohort studies from 2014 and 2015 with a total of 199 patients that underwent emergent surgery (39 ER and 160 OR). We also included 26 patients from our institution. For emergency treatment, 30-day major amputation rates (18% vs 3%, Odds Ratio 5.82, 95% CI [1.75; 19.30], p = .004), 30-day mortality rates (10% vs 1%, Odds Ratio 5.57, 95% CI [1.01; 30.58], p = .05), 1-year major amputation rates (15% vs 6% Odds Ratio 3.61, 95% CI [1.18; 11.09], p = .02), 1-year loss of primary patency (54% vs 23%, Odds Ratio 3.19, 95% CI [0.91; 11.20], p = .07), and 1-year loss of secondary patency (44% vs 12%, Odds Ratio 6.91, 95% CI [3.01; 15.83], p < .05) were higher in the ER group when compared to the OR group.
Conclusion
Endovascular repair represents an alternative approach for the emergency treatment of PAA. Limited evidence from the available non-randomized studies shows unfavorable outcomes for patients undergoing ER. However, the results are prone to selection bias, and only randomized trials comparing ER to OR might reveal whether a subgroup of patients would benefit from ER as primary treatment of PAA in an emergency setting.
Background
Since 1994 endovascular repair has been used as an alternative to the gold standard of open repair (OR) for the treatment of popliteal artery aneurysms (PAA). 1 When symptomatic, PAA should undergo repair regardless of its size. Risk factors associated with growth of popliteal aneurysms are a diameter of 20 mm or more, the presence of a luminal thrombus, and atrial fibrillation. 2
There is no unique approach to OR. It is not clear which approach has the better outcomes: vein or prosthetic graft, posterior or medial approach. 3 Endovascular repair (ER) represents an attractive alternative approach due to its lower access morbidity and length of hospital stay. 4
Several meta-analyses have been performed to evaluate the outcomes of OR and ER in the treatment of PAA.5,6 Moreover, studies reporting on the use of fibrinolysis in the acute treatment of PAA have been published. 7 Recent guidelines from the Society of Vascular Surgery recommend a stratification of thrombotic or embolic complications of PAA depending on the severity of ischemia at presentation to decide if a thrombolysis or pharmacomechanical intervention should be performed. 8 Only one randomized controlled trial exists comparing OR with ER for elective asymptomatic PAA. 9 Registries such as those in Germany 10 or the Swedvasc 11 and Vascunet collaboration 12 represent a unique approach, making it possible to analyze the modern treatment of PAA. Recently, a meta-analysis also addressed the natural history of popliteal artery aneurysms. 13 However, no meta-analyses on the emergency treatment of PAA comparing OR with ER has been published. With the advances in endovascular repair in recent years, an analysis of the current outcomes of OR and ER in the treatment of popliteal aneurysms in an emergency setting is important. The aim of this meta-analysis was to summarize and compare the available evidence on outcomes of patients undergoing OR or ER for the emergency treatment of popliteal aneurysms. We also present and include into the analyses our single center experience on the treatment of PAA, reporting on 26 patients.
Methods
The literature search and data analysis were conducted in accordance with the MOOSE guidelines. 14 The study has been registered in the PROSPERO database. 15
Search strategy
The PubMed/Medline database was searched for this study through its respective online search engine. The search was performed on studies published between database inception and a defined search date. The last search date was on 24.05.2021. The PICO (population, intervention, control, outcome) framework was used to develop the literature search strategy. A protocol was established according to the evidence-based PICO model to answer the following research question: “In Patients undergoing emergency treatment for popliteal aneurysms, what is the effect of endovascular repair on mortality, morbidity, limb salvage and other outcomes compared with open repair?” The following search strategy was used: (“Popliteal” [Mesh] OR Poplit*[tw]) AND (“Aneurysms” [Mesh] OR Aneurys*[tw]) AND (“Surgical Procedures, Operative” [Mesh] OR Operat*[tw] OR Surg*[tw] OR Excision*[tw] OR Dissection*[tw] OR resect*[tw] OR removal*[tw] OR ectomy [tw]) AND (“endovascular” [Mesh] OR endovasc*[tw]). Furthermore, the reference lists of the included studies were manually searched to find relevant articles. Abstracts and full-text reviews were evaluated independently in an unblinded standardized manner by two authors (AR and JP) to assess eligibility for inclusion or exclusion. Disagreements between reviewers were resolved by consensus; if no agreement could be reached, a third reviewer (JU) decided whether to include the respective study. If abstracts of unpublished studies were detected, contact with the authors was sought. In addition, data for all patients treated for popliteal aneurysms at our center from 2009 to 2021 were analyzed.
Inclusion and exclusion criteria
Articles in English, German, Spanish, Portuguese, and Italian language were considered. Studies reporting on outcomes for endovascular and open surgery both for elective and emergent treatment of popliteal aneurysms (as defined in the single studies) were included. Studies with an irrelevant abstract or title were excluded, and so were reviews, case reports, case series with less than five patients, comments, and letters. Details of the study selection process are summarized in a flowchart Figure 1. Flowchart with the number of studies identified, screened, assessed and finally included in the meta-analysis.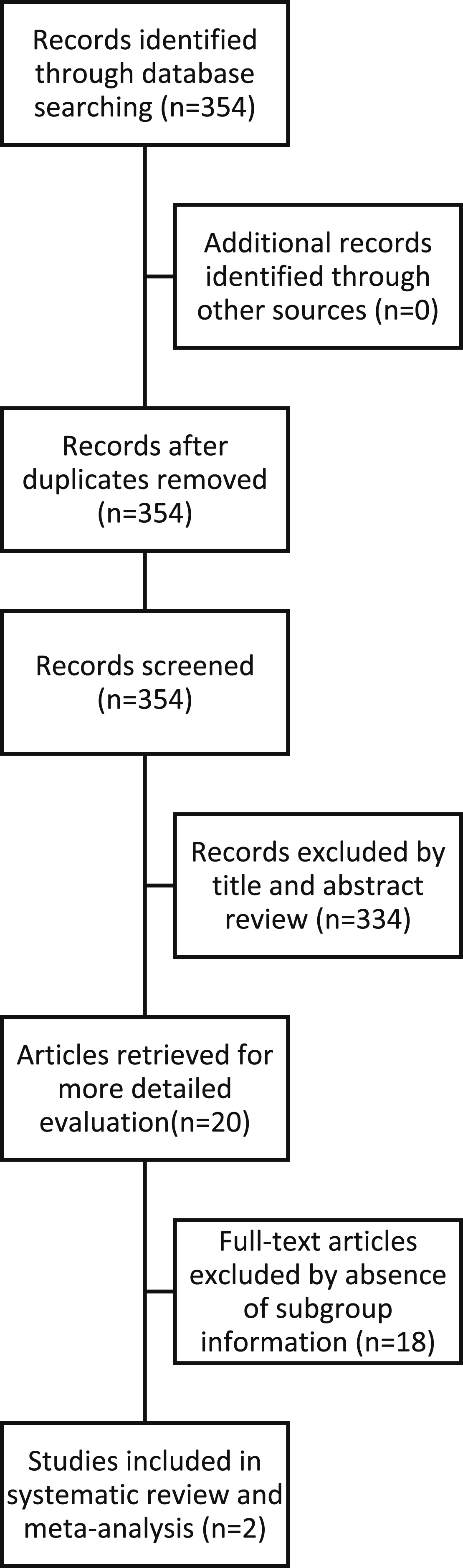
From our institutional patient collective, patients were included if they underwent endovascular (stent graft, thrombolysis) or open (vein or prosthetic graft bypass) treatment for the diagnosis of a popliteal aneurysm (focal dilation of the popliteal artery by >50%). PAA diagnosis was performed by Doppler ultrasound or computed tomography. Emergency treatment was defined as immediate treatment (within 6 hours of diagnosis) for acute limb ischemia or aneurysm rupture.
Data collection
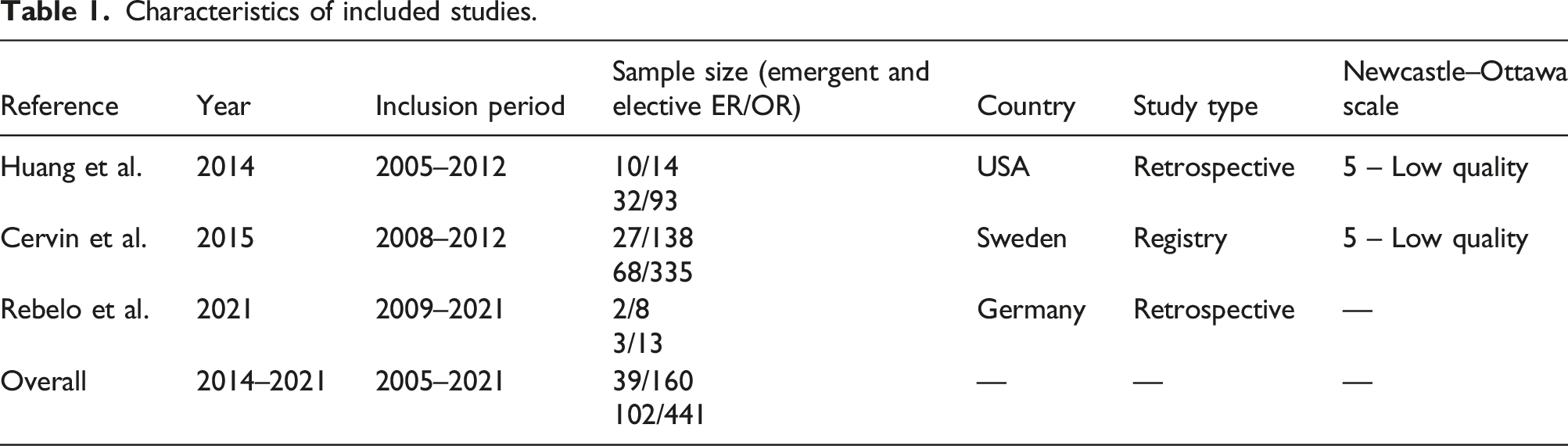
Studies were analyzed, and data were extracted separately by two investigators and presented in a tabular fashion. The following descriptive data were documented for each selected study: first author, year of publication, inclusion period, sample size, country where the study was conducted and study type. The following patient and operation characteristics were documented: total number of patients, mean or median age, sex, and comorbidities. The following predefined outcomes were extracted: mortality (30-day), morbidity (any type of complication, surgical and medical), major amputation rates (30 day and 1-year), 1-year primary patency rate, 1-year secondary patency rate, and 1-year survival. Each outcome was documented for ER and OR in both an elective and emergent setting. Risk of bias was assessed using the Newcastle-Ottawa Scale. 16
The clinical data of consecutive patients with PAA treated at the University Hospital Halle (Saale), Germany, between 1 January 2009, and 31 March 2021, were retrospectively reviewed. Patients were asked to return at 1, 3, and 6 months and 1 year after intervention for physical examination, ankle-brachial index measurement, and duplex ultrasound imaging. Patency rates were based on imaging studies. Follow-up information and patient vital status was obtained from the medical records and mailing questionnaires. The above-mentioned patient and operation characteristics and outcomes were extracted. Patients were divided in four groups by the type and urgency of the intervention: ER or OR and elective or emergency.
Statistical analysis
The Review Manager (RevMan) software, version 5.3 (Cochrane Collaboration, Oxford, UK) was used. If a given outcome was present in all studies, a meta-analysis was performed, firstly on emergency versus elective therapy, with both groups comprising ER as well as OR, and a subsequent subgroup analysis of ER and OR. Secondly, ER and OR were compared in an emergency setting. The magnitude of the effect estimate was visualized by forest plots. An odds ratio was calculated for binary data and the weighted mean difference for continuous data. The 95% confidence interval (CI), heterogeneity, and statistical significance was reported for each outcome. The X2 test was used for the evaluation of statistical significance. p < .05 was statistically significant. Descriptive statistics from our patient collective are reported as number (percentage) or mean (standard deviation).
Results
Characteristics of included studies.
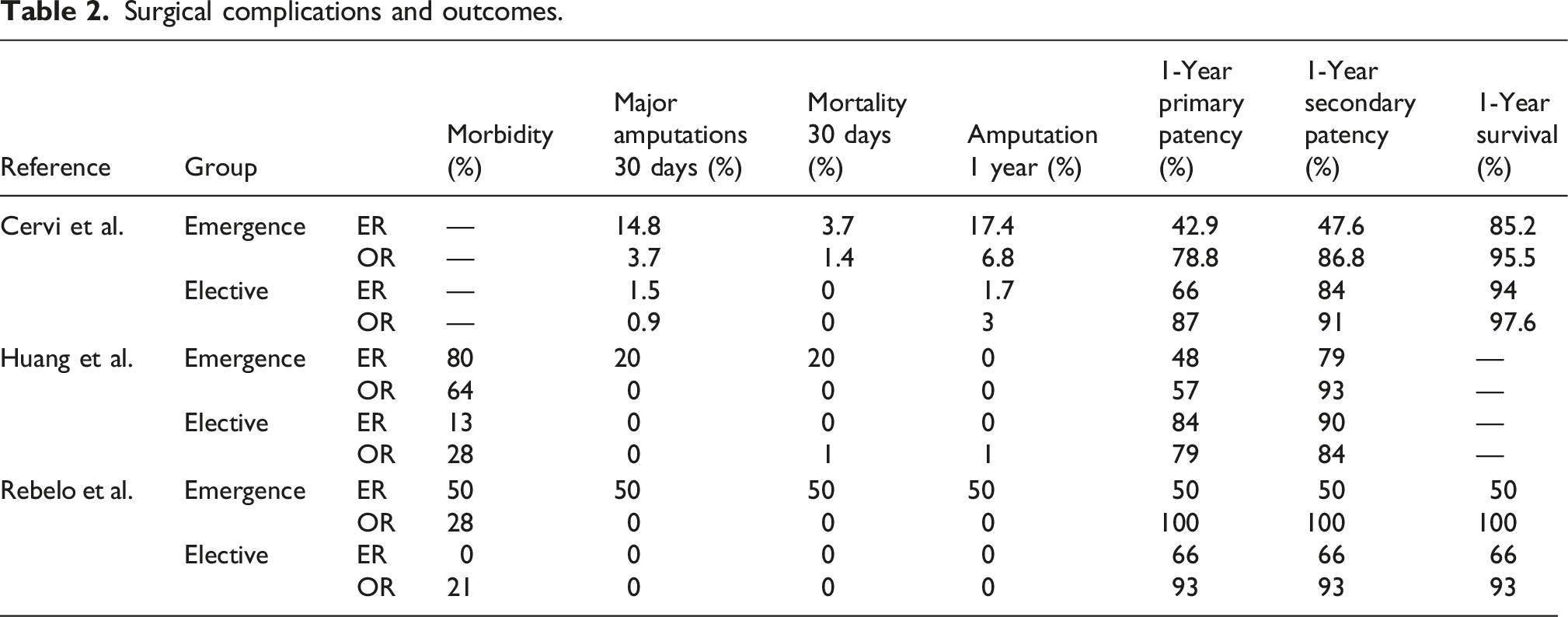
Surgical complications and outcomes.
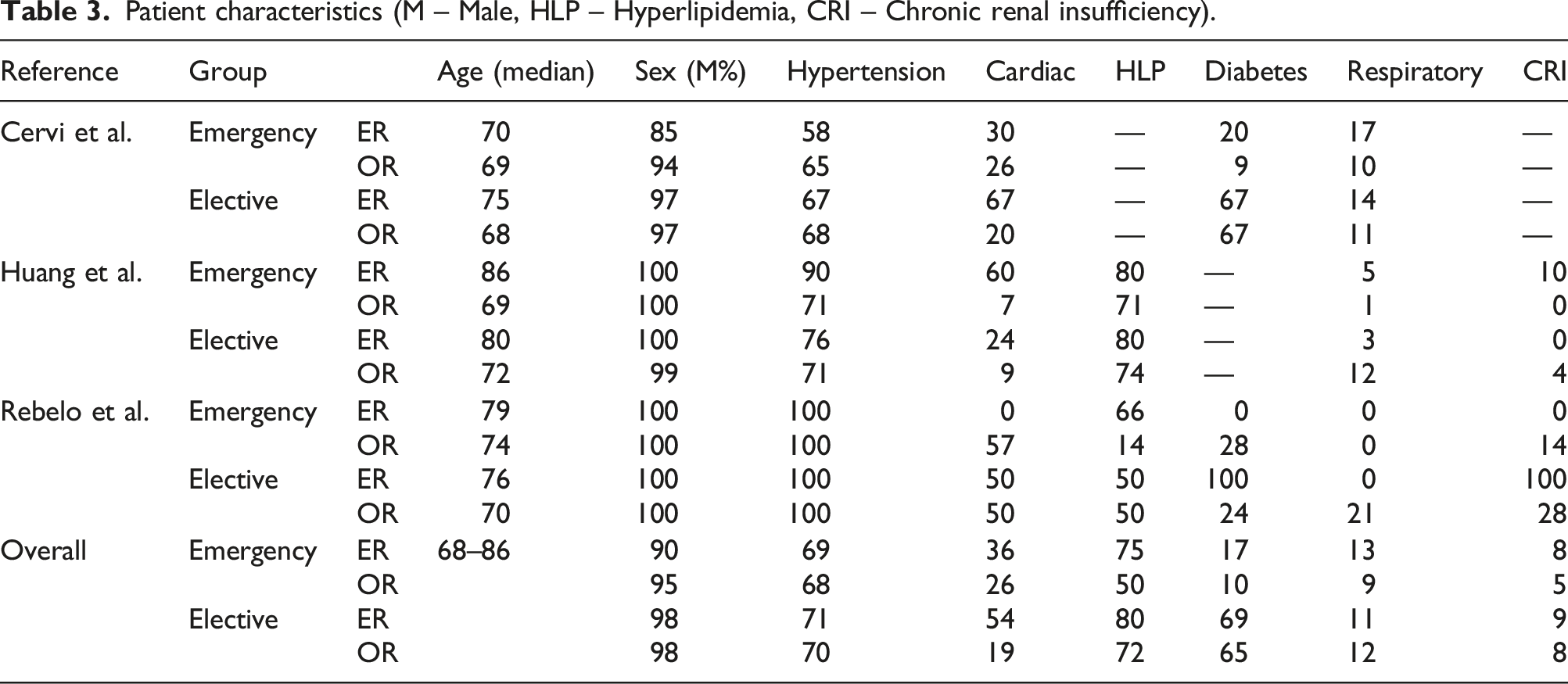
Patient characteristics (M – Male, HLP – Hyperlipidemia, CRI – Chronic renal insufficiency).
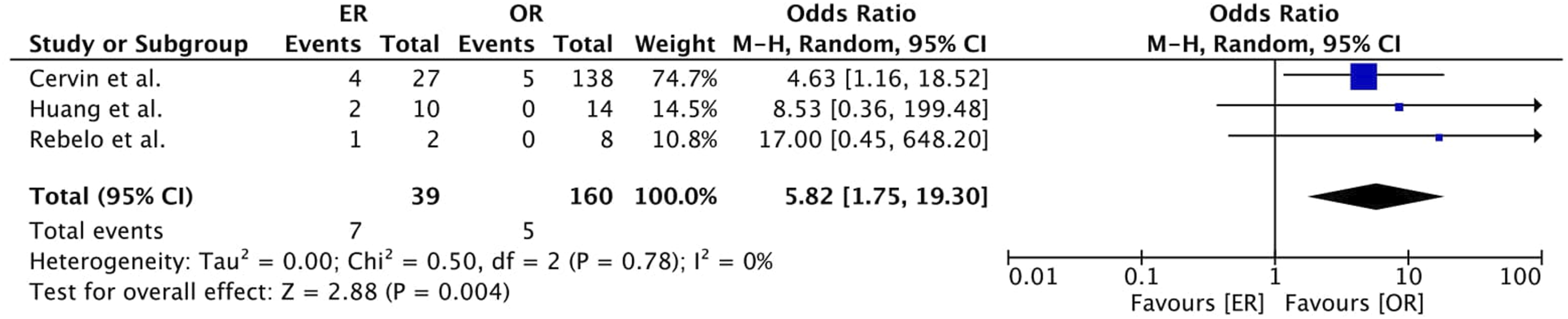
Concerning major amputation (30-day), our meta-analysis showed lower rates for the elective group (4% vs 0.7%, Odds Ratio 5.00, 95% CI [1.10; 22.72], p = .04), also in the ER subgroup analysis (18% vs 1% Odds Ratio 12.1, 95% CI [2.35; 62.18], p = .003) but not for the OR subgroup analysis (0.6% vs 0.7%, Odds Ratio 0.81, 95% CI [0.08; 7.83], p = .85) (Figure 2). Major amputation (30 days) rates in emergency treatment were higher in the ER group when compared to the OR group (18% vs 3%, Odds Ratio 5.82, 95% CI [1.75; 19.30], p = .004). (Figure 3). Forest plot of pooled odds ratio with 95% CI for emergency versus elective surgery regarding Major Amputation (30 Days) with subgroup analysis for ER and OR. Forest plot of pooled odds ratio with 95% CI for ER versus OR in emergency surgery regarding Major Amputation (30 Days).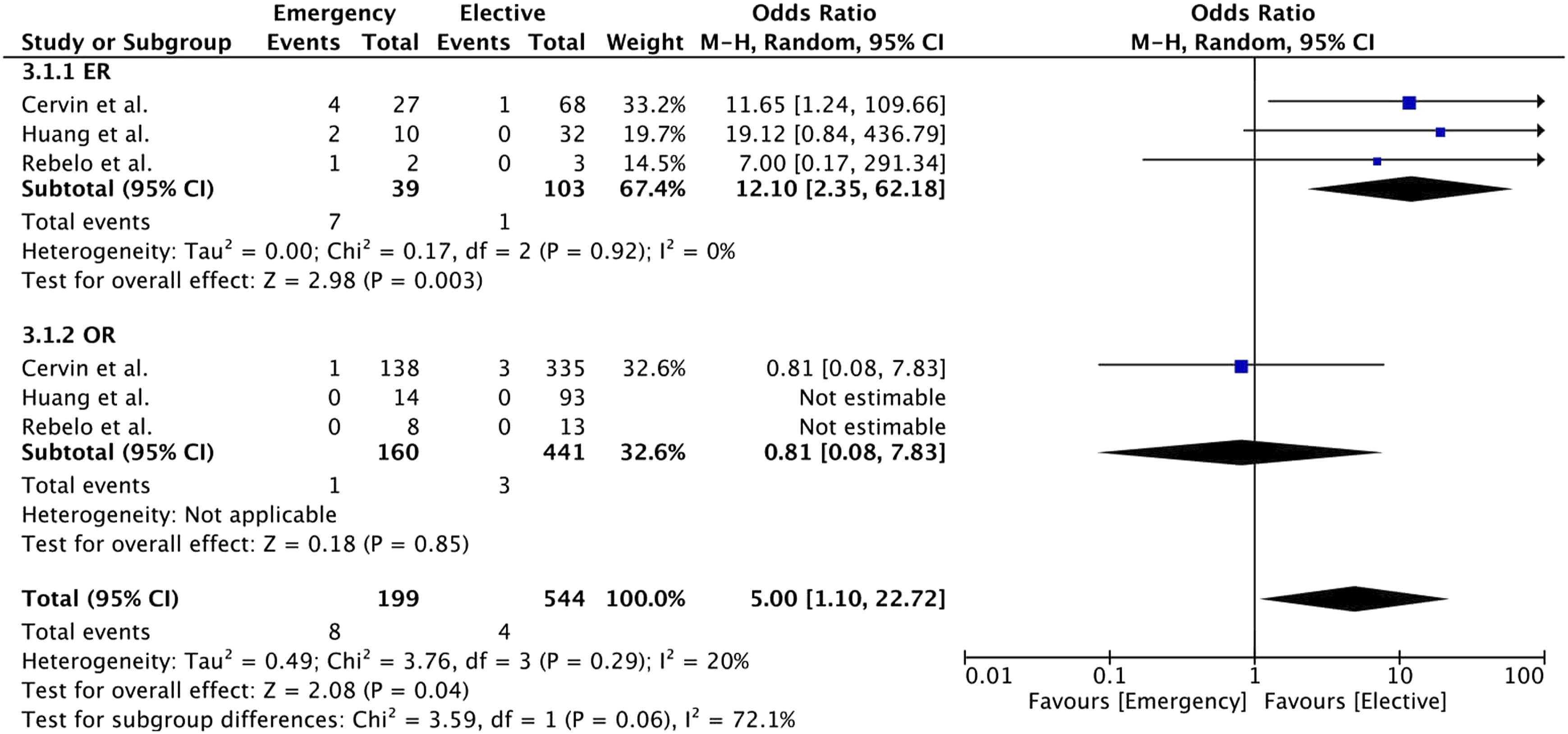
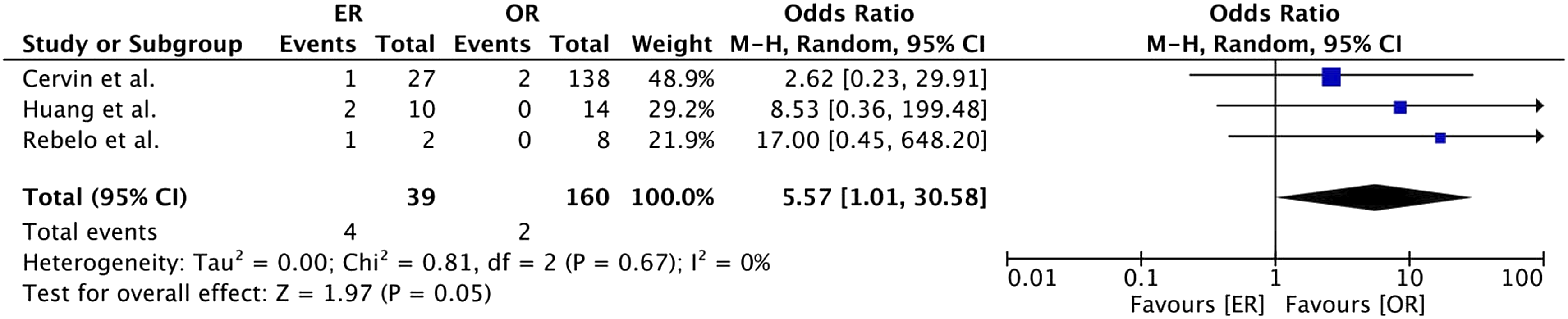
In the included studies, mortality (30-day) was higher in the emergency group than in the elective group (3% vs 0.2%, Odds Ratio 7.95, 95% CI [1.86; 34.06], p = .005, ER subgroup 10% vs 0% Odds Ratio 10.62, 95% CI [1.55; 72.80], p = .002), OR subgroup 1% vs 0.2%, Odds Ratio 5.41 95% CI [0.59; 49.87], p = .14) (Figure 4). Our analysis demonstrated higher mortality rates in the ER group compared to the OR group for emergency surgery (10% vs 1%, Odds Ratio 5.57, 95% CI [1.01; 30.58], p = .05) (Figure 5). Forest plot of pooled odds ratio with 95% CI for emergency versus elective surgery regarding Mortality with subgroup analysis for ER and OR. Forest plot of pooled odds ratio with 95% CI for ER versus OR in emergency surgery regarding Mortality.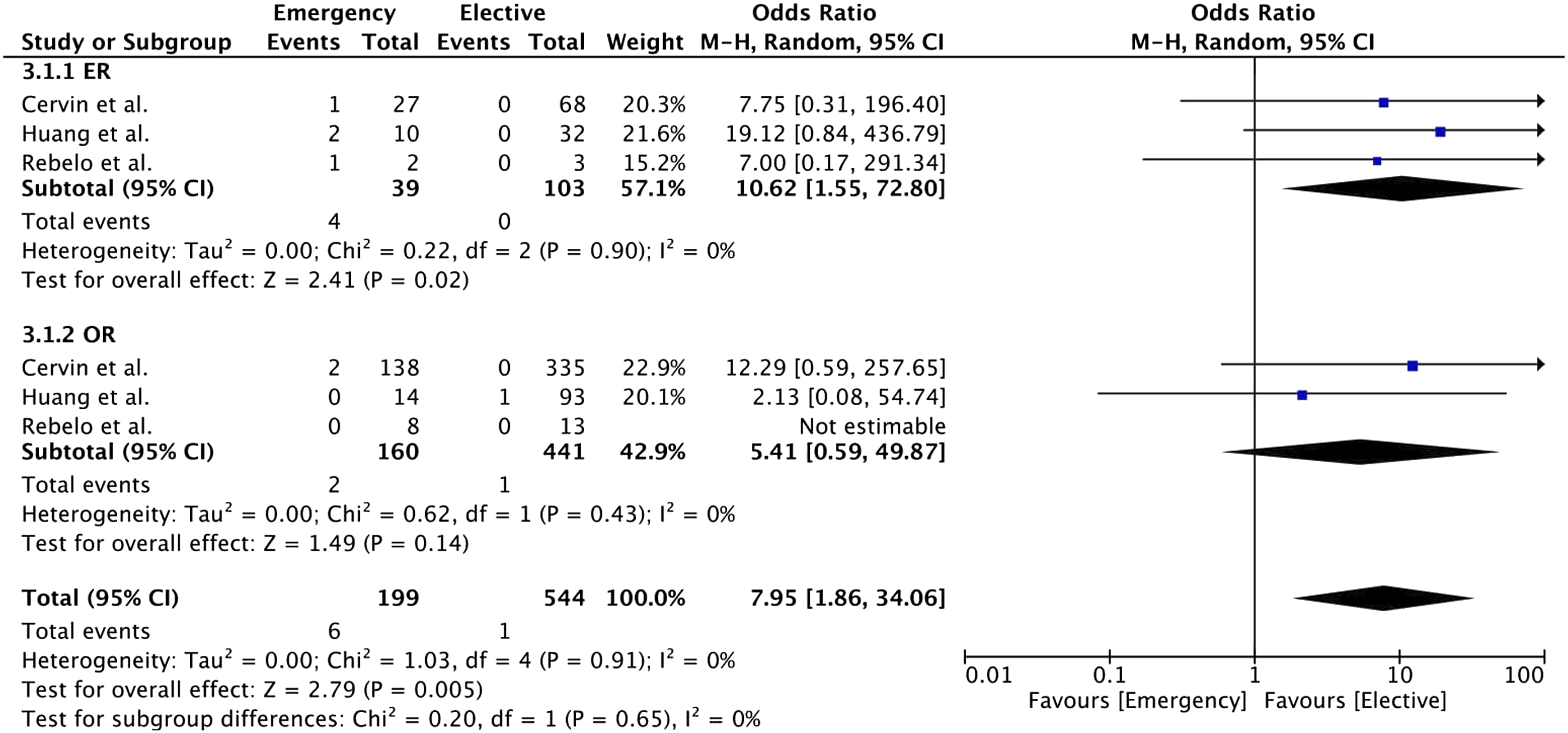
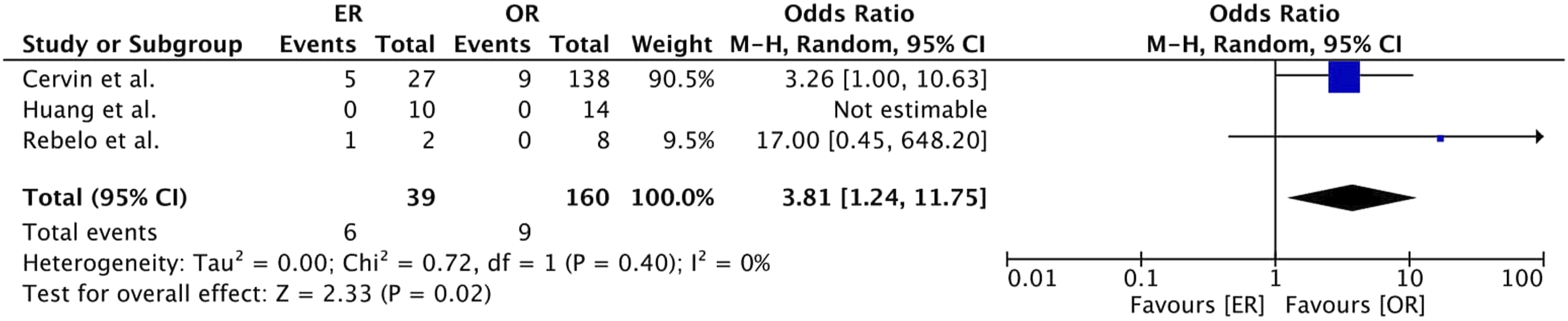
Regarding 1-year amputation rates in both the ER (15% vs 1%, Odds Ratio 12.46, 95% CI [1.87; 82.88], p = .009) and OR (6% vs 2%, Odds Ratio 2.26, 95% CI [0.93; 5.48], p = .07) subgroup, higher rates were reported in the emergency group compared to the elective group (8% vs 2%, Odds Ratio 3.07, 95% CI [1.37; 6.86], p = .006) (Figure 6). In emergency surgery, higher rates were observed in the ER group compared to the OR group (15% vs 6% Odds Ratio 3.81, 95% CI [1.24; 11.75], p = .02) (Figure 7). Forest plot of pooled odds ratio with 95% CI for emergency versus elective surgery regarding Amputation Rate (1 Year) with subgroup analysis for ER and OR. Forest plot of pooled odds ratio with 95% CI for ER versus OR in emergency surgery regarding Amputation Rate (1 Year).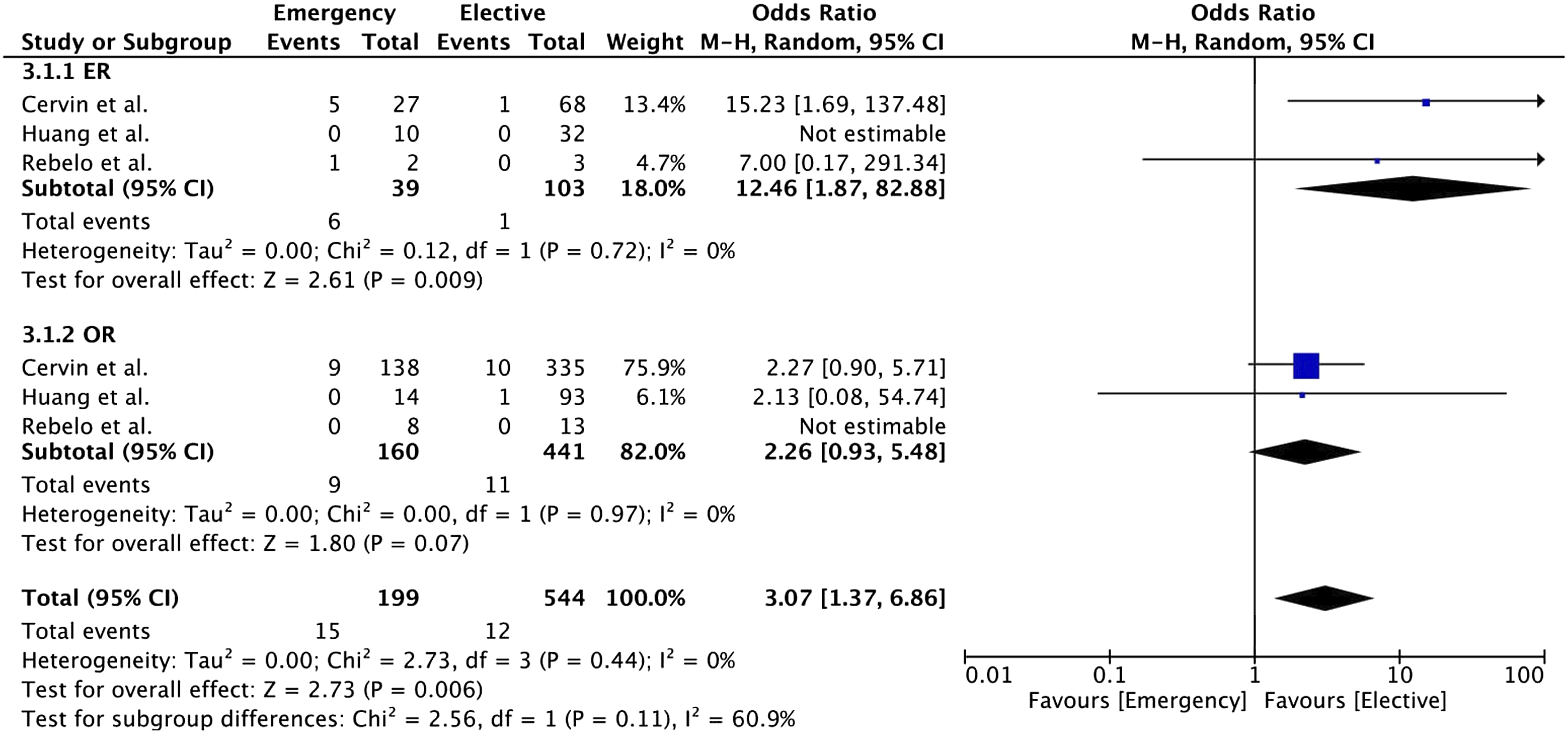
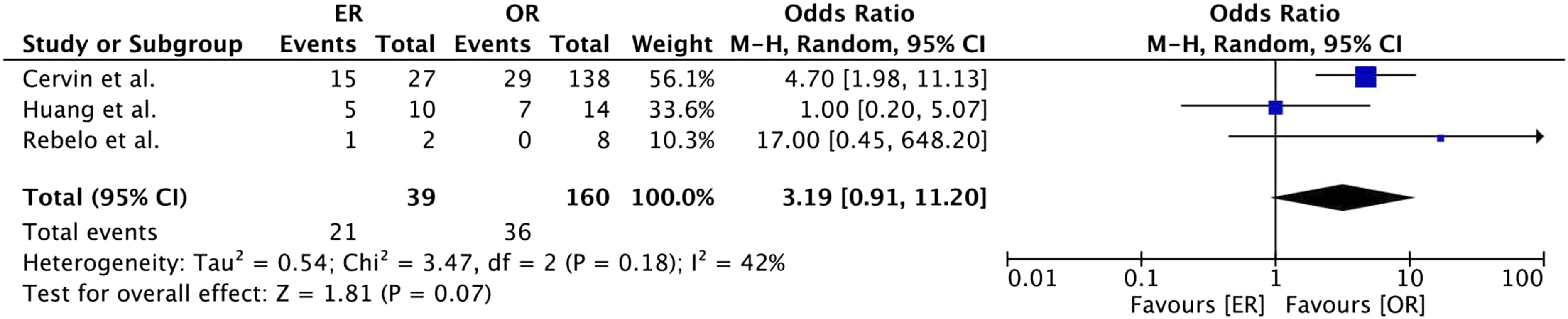
A higher loss of primary patency (1 year) was observed in the emergency group when compared to the elective group (29% vs 17%, Odds Ratio 2.16, 95% CI [1.45; 3.23], p < .05). The same observation persisted in the ER (54% vs 28%, Odds Ratio 2.94, 95% CI [1.36; 6.34], p = .006) and OR (23% vs 15%, Odds Ratio 1.93, 95% CI [1.21; 3.09], p = .006) subgroup analysis (Figure 8). When comparing ER and OR in emergency surgery, no statistically significant result was obtained (54% vs 23%, Odds Ratio 3.19, 95% CI [0.91; 11.20], p = .07) (Figure 9). Forest plot of pooled odds ratio with 95% CI for emergency versus elective surgery regarding loss of primary patency (1 year) with subgroup analysis for ER and OR. Forest plot of pooled odds ratio with 95% CI for ER versus OR in emergency surgery regarding loss of primary patency (1 year).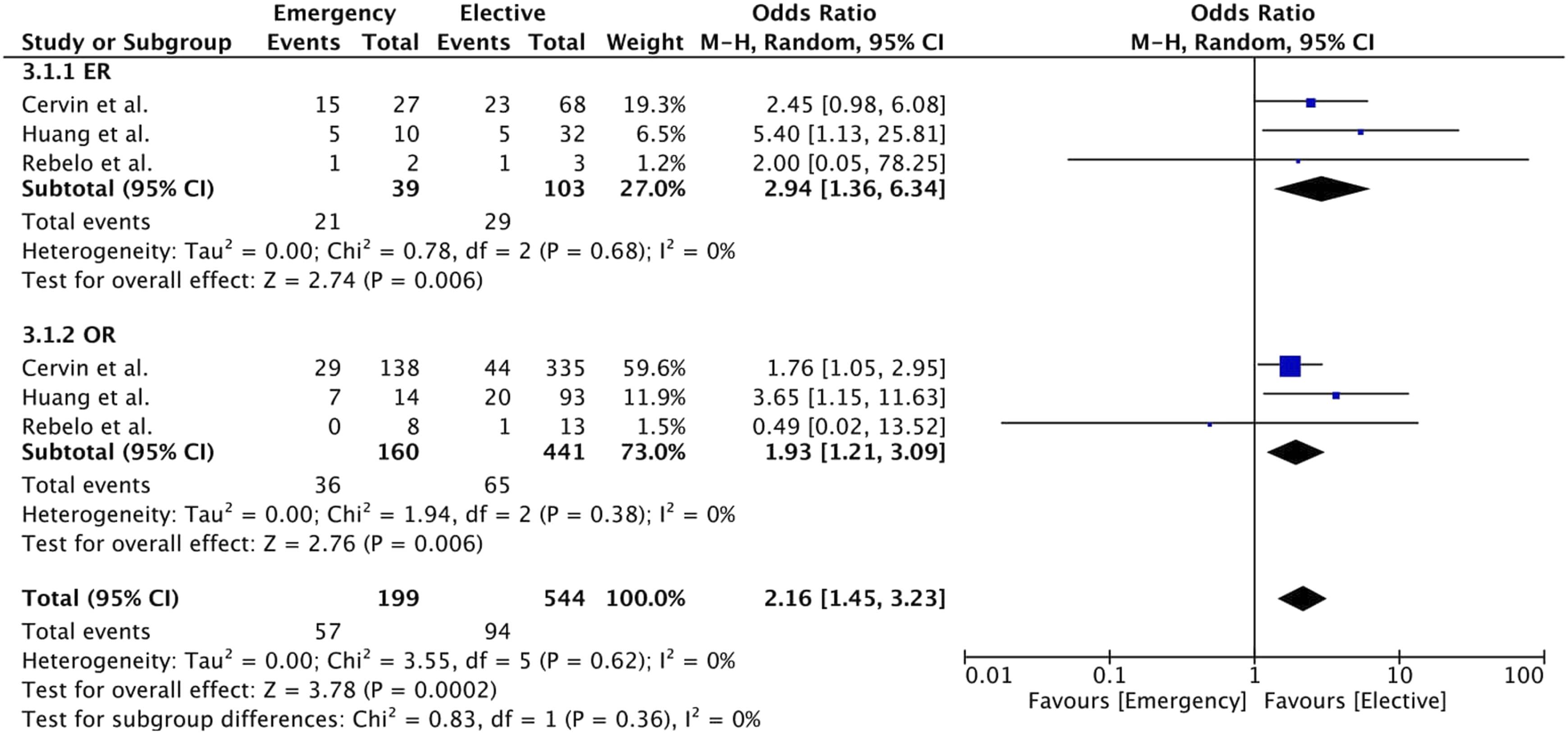
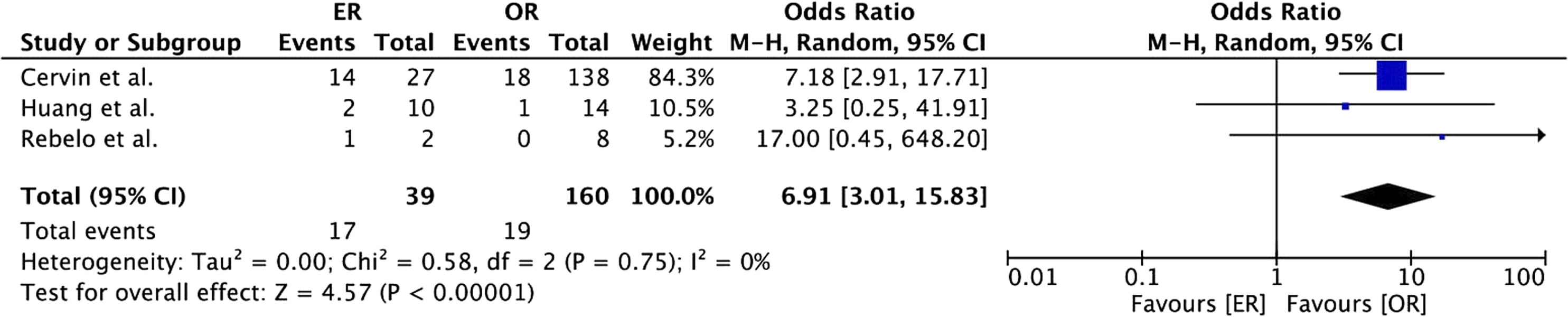
Loss of secondary patency (1 year) was higher in the emergency group (18% vs 9%, Odds Ratio 2.41, 95% CI [1.21; 4.78], p = .01). In the subgroup analysis of ER and OR, a similar result was observed (44% vs 15%, Odds Ratio 4.48, 95% CI [1.90; 10.60], p < .05; 12% vs 8%, Odds Ratio 1.25, 95% CI [0.35; 4.49], p = .73) (Figure 10). In the meta-analysis of ER versus OR in emergency treatment, higher rates of loss of secondary patency (1 year) were observed in the ER group (44% vs 12%, Odds Ratio 6.91, 95% CI [3.01; 15.83], p < .05) (Figure 11). Forest plot of pooled odds ratio with 95% CI for emergency versus elective surgery regarding loss of secondary patency (1 year) with subgroup analysis for ER and OR. Forest plot of pooled odds ratio with 95% CI for ER versus OR in emergency surgery regarding loss of secondary patency (1 year).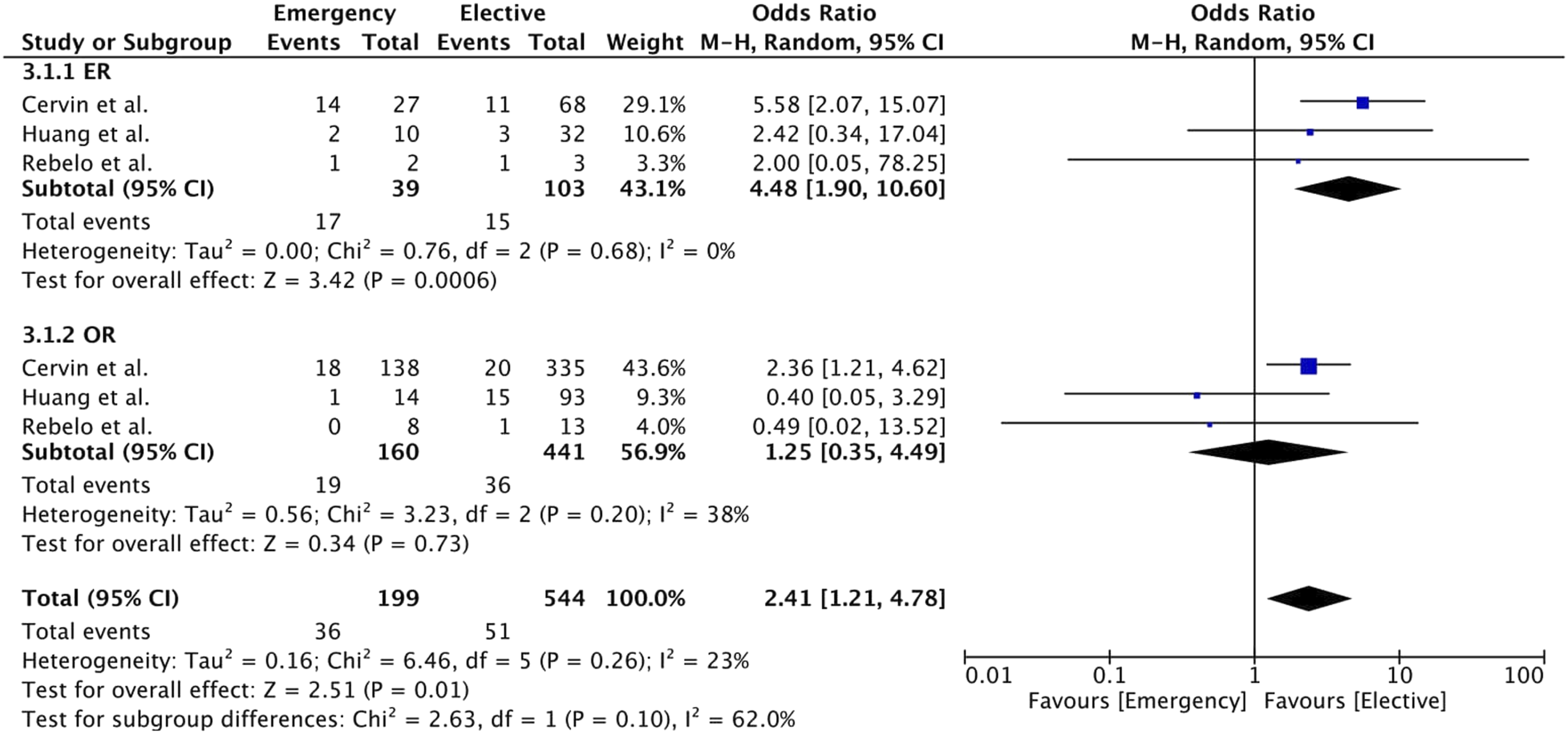
Discussion
In our analysis, there are two major findings, concerning both short-term and long-term outcomes. The first is the higher 30-day mortality and major amputation rate for ER for emergency treatment. The second is that 1-year major amputation rates and rates of loss of 1-year primary and secondary patency are higher after endovascular repair in emergency surgery.
Our meta-analysis is the first one comparing OR and ER for emergency surgery. Studies concerning popliteal aneurysms are scarce and mostly reporting on asymptomatic patients undergoing elective repair without comparing ER and OR in an emergency setting. In a Cochrane Database Systematic Review on endovascular versus open repair of asymptomatic popliteal aneurysms, only one single RCT was identified. 18 In this study from Antonello et al., 15 patients underwent ER and 15 patients OR. The primary patency rate at 12 months was 100% for OR and 86.7% for ER. 9 In another study involving 390 patients with asymptomatic popliteal aneurysms, no mortality was observed. OR showed lower primary patency loss (HR 0.25; 95% CI, 0.10–0.58; p < .05). 19 In a Study from Germany including 206 patients with OR, overall mortality was 2% with no differences in 5-year primary patency between emergent and elective therapy. 20 Concerning ER, 1-year primary patency rates between 74.2% and 87% have been described.21-25 In another study, Speziale et al. analyzed 53 patients who underwent ER. At a mean follow-up of 37.4 ± 29.3 months, primary patency, secondary patency, and limb salvage rate were 73.6, 92.4, and 100%, respectively. 26 In our analysis, major amputation rate at 30 days and 1 year, loss of 1-year primary patency and loss of 1-year secondary patency rates were higher for emergency surgery in both the ER and OR groups. This reinforces the need for an analysis including only emergency patients.
After emergency treatment, 30-day mortality and major amputation rates were higher for endovascular repair
In our analysis, the major amputation rate at 30 days was 0.7% for elective patients and 6% for emergency surgery. These results are comparable with a study from Vascunet, involving data from 1471 popliteal aneurysm repairs from 10 countries: the overall major amputation rate was 2.0% after elective and 6.5% after emergency surgery. Major amputation rates were higher for hybrid repair (26.3%) compared to OR (1.8%) and ER (1.0%, p < .0001). 27 In another study from Italy, involving 234 open procedures, the 30-day major amputation rate was 3.8%. 28 Concerning acute popliteal artery aneurysm thrombosis and leg ischemia, a study analyzed the outcomes of preoperative and intraoperative use of intra-arterial thrombolysis reporting 30-day amputation rates of 18% and 29%, respectively. 7 Leak et al. reported on 186 popliteal aneurysms (110 OR, 76 ER). OR was performed in more patients with thrombosis (41.8% vs 5.3%; p < .001), acute ischemia (24.5% vs 9.2%; p < .010), and ischemic rest pain (34.5% vs 6.6%; p < .001). There was no difference in major amputation rates (OR, 3.7%; ER, 1.3%; p = .65). 29 In a meta-analysis comparing ER with OR and comprising 652 patients, there were no differences regarding limb salvage between groups (Odds Ratio 0.59, 95% CI 0.16–2.15). 30 These data highlight again the need to separate emergency and elective treatment when comparing ER and OR. According to our analysis OR is superior to ER concerning both short-term major amputation and mortality.
Higher rates of 1-year major amputation and loss of primary and secondary patency were observed in the ER group in emergency treatment
Regarding long-term outcomes, the available data mostly do not separate between elective and emergency treatment. In a retrospective study, Saunders et al. reported primary and secondary patency for ER of 88% and 90%, respectively. 31 In a study from Italy, no differences on secondary patency were observed at 1 year between ER and OR (94% vs 94%, p = .9). 32 In a 2016 meta-analysis, 14 studies with 4880 popliteal artery aneurysm repairs (OR, 3915 and ER, 1210) were identified. One-year Primary patency was better for OR (Hazard Ratio 0.607, p = .01) and no difference in 1-year secondary patency (Hazard Ratio 0.770, p = .46) was observed. 5 Another meta-analysis from 2015 reported outcomes for 514 popliteal artery aneurysm repairs. Pooled primary and secondary patency rates at 5 years were 69.4% (95% CI 63.3%–76.2%) and 77.4% (95% CI 70.1%–85.3%), respectively. No difference in primary patency (Hazard Ratio 1.30, 95% CI 0.79 to 12.14, p = .189) was described. 6 The data on long-term results of ER after emergency surgery are scarce, but long-term results of OR are superior to ER. Better patient selection regarding suitable anatomy for ER and improvement of endovascular stent grafts could improve results for this approach.
The main limitation of this meta-analysis is that it is based exclusively on two small non-randomized studies and a small unpublished and not peer-reviewed single center patient collective. Furthermore, the lack of patient-level data from the included studies and potential publication bias are also important limitations, leading to a potentially high risk of bias. Because of the low statistical power and corresponding wide 95% confidence intervals, the results should be appreciated with caution. Multicentric RCTs and registries with patients who underwent emergency repair of popliteal aneurysms are needed to identify which patients could benefit from ER or OR.
Conclusion
In this meta-analysis, all relevant studies providing comparative information on the outcome of patients undergoing ER or OR for the treatment of PAA in the emergency setting were included. Limited evidence from the available non-randomized studies shows unfavorable outcomes for patients undergoing ER. However, the results are prone to selection bias, and only randomized trials comparing ER to OR might reveal whether a subgroup of patients would benefit from ER as primary treatment of PAA in an emergency setting.
Footnotes
Authors’ contributions
AR outlined, wrote, and drafted the manuscript. All authors critically revised the manuscript and read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.