
Abstract
Objectives
Open lower extremity revascularization is controversial among octogenarians; however, the indications for surgical bypass are higher in the elderly population. The aim of the study was to compare postoperative outcomes between octogenarians and non-octogenarians following femoropopliteal bypass surgery.
Methods
Our regional, multi-institutional database was queried for femoropopliteal bypass procedures performed between 1995 and 2020. Electronic medical records were individually reviewed for operative and postoperative data. Univariable and multivariable logistic regression were utilized to determine predictors of postoperative outcomes.
Results
Among 1315 patients who underwent femoropopliteal bypass, 234 (17.8%) were octogenarians. Octogenarians more frequently underwent bypass for lower extremity tissue loss (48.7% vs 30.2%), whereas claudication was more common among non-octogenarians (24.0% vs 9.8%) (p < .001). Below-knee bypass target (72.2% vs 59.3%) and prosthetic conduit utilization (58.5% vs 43.7%) were more frequent in octogenarians (p < .001 each). Overall hospital length of stay was longer among patients > 80 years (median 6 days [interquartile range [IQR] 4–9] vs 5 days [IQR 4–8], p = .017). The overall 30-day (5.6% vs 1.5%) and one-year mortality rates (25.6% vs 7.9%) were higher among octogenarians (p < .001 each). On multivariable analysis, age greater than 80 years was found to be an independent risk factor for postoperative mortality (OR 3.79 [1.75–8.20], p = .0007)
Conclusions
Octogenarians undergoing bypass femoropopliteal bypass surgery have considerably worse postoperative outcomes, compared with non-octogenarians. These data may help inform elderly patients prior to undergoing open lower extremity revascularization.
Introduction
Peripheral artery disease (PAD) is prevalent in the elderly population.1,2 A variety of treatment modalities may be employed in the management of PAD, ranging from medical therapy, to endovascular techniques, to open surgical intervention, and to hybrid open/endovascular procedures. 3 Among these, providers have been reluctant to offer complex open revascularization procedures to the elderly population. The reasons for this sentiment are manifold, and coincidentally, the utilization of endovascular techniques has witnessed an exponential growth over the past several decades.4,5 Various studies have reported worse outcomes in octogenarians; however, these reports have been primarily situated within the cardiac surgery literature.6–11 Data on postoperative outcomes in octogenarians after vascular surgery, on the other hand, has been sparse and anecdotal.
Octogenarians may be a high-risk patient population for any surgical intervention. This special population deserves careful consideration of surgical risks and benefits, given a higher prevalence of comorbidities and frailty.12–14 This becomes a dilemma as the indications for lower extremity revascularization increase with age. 15 On the basis of these facts, no population-based studies have investigated outcomes after open infrainguinal revascularization surgery in octogenarians. The primary aim of this study was to compare postoperative outcomes in octogenarians versus non-octogenarians after femoropopliteal bypass.
Methods
A retrospective cohort study was performed using the multi-institutional Research Patient Data Registry (RPDR) database. The RPDR was queried for patients who underwent femoropopliteal bypass using International Classification of Diseases, 9th and 10th edition (ICD-9/10) and current procedural terminology (CPT) procedural codes. Demographic data and medical comorbidities were obtained through the RPDR. Electronic medical records were then queried for operative details and postoperative outcomes. The study period was between 1995 and 2020.
Patients were grouped into two cohorts according to age at time of bypass. Patients aged greater than 80 years (octogenarians) were compared to patients aged 18–79 years (non-octogenarians). Primary outcomes of interest were 30-day mortality, hospital length of stay (LOS), and unplanned hospital readmission.
Continuous variables were reported in median and interquartile range (IQR); and categorical variables were reported in frequency (n) and percentages (%). Univariate analysis was performed using t and χ2 tests. Logistic regression analysis was performed for categorical variables, and linear regression was utilized for continuous variables. Statistical analysis was performed with Stata software version 15.1 (StataCorp, College Station, TX). This study was approved by the Institutional Review Board at the Mass General Brigham hospital system.
Results
A total of 1315 patients underwent femoropopliteal bypass during the study period. Octogenarians comprised 17.8% (n = 234) of all patients. The median age of the non-octogenarian group was 67 years (IQR 60–72) compared to 83 years (IQR 81–86) for octogenarian patients (p < .001). Patient population is broken down by decade on Figure 1(a). (a) Patient population by age group. (b) Surgical indication by age group.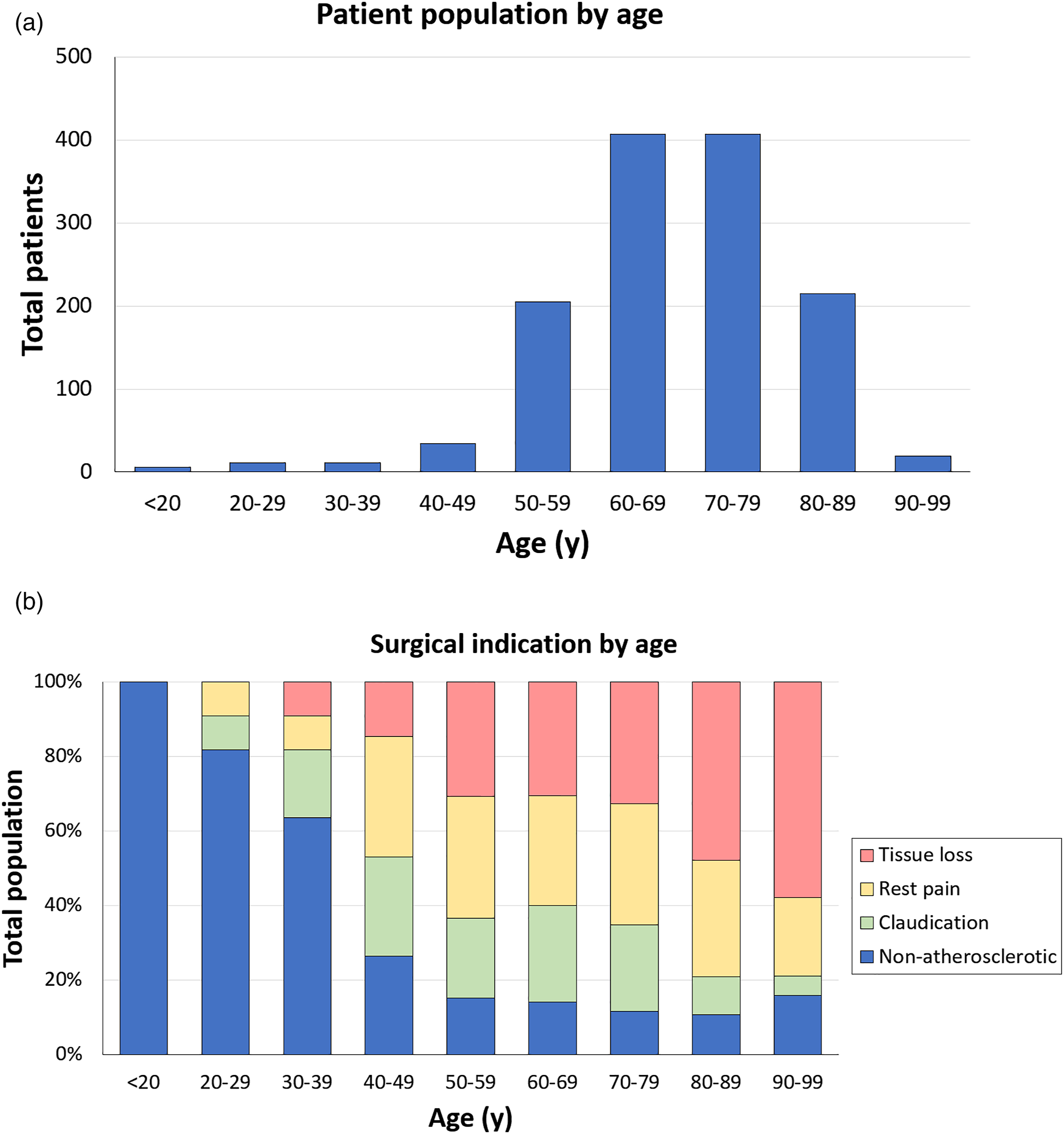
Patient demographics by age group.
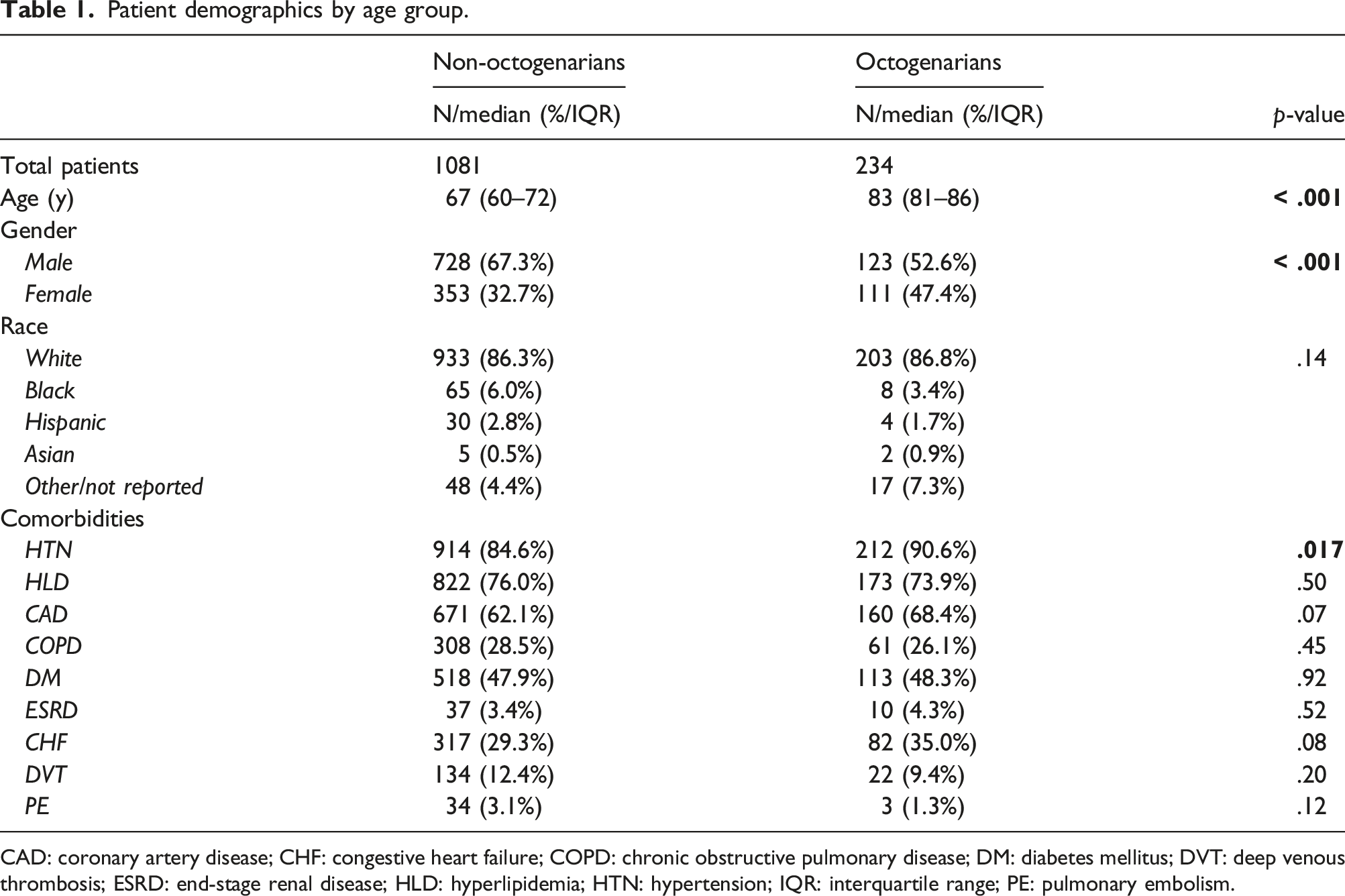
CAD: coronary artery disease; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; DVT: deep venous thrombosis; ESRD: end-stage renal disease; HLD: hyperlipidemia; HTN: hypertension; IQR: interquartile range; PE: pulmonary embolism.
Indications for surgery by age group.
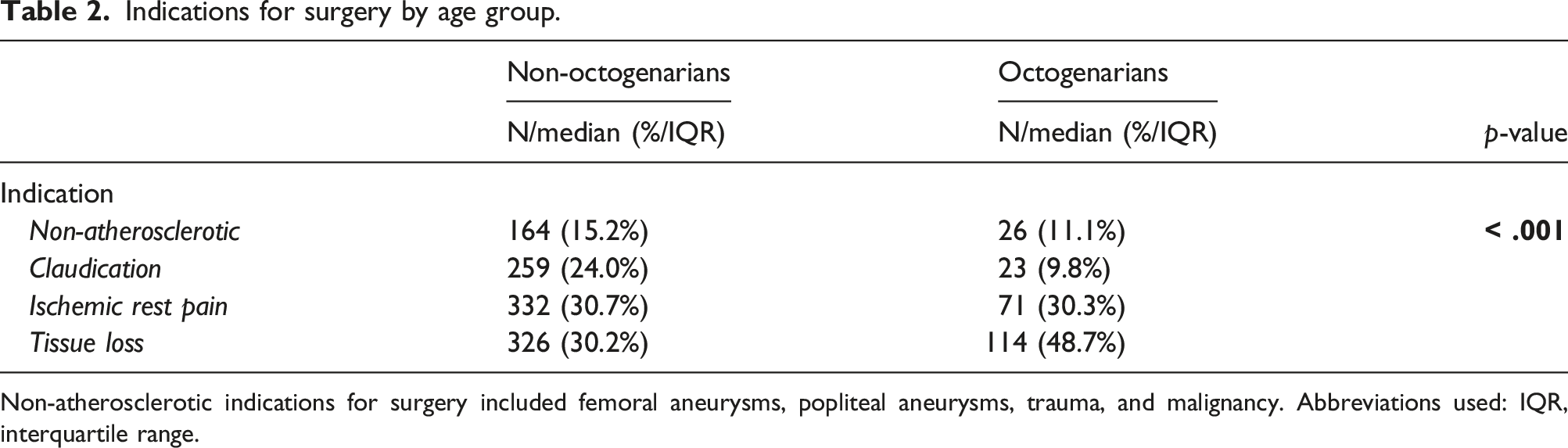
Non-atherosclerotic indications for surgery included femoral aneurysms, popliteal aneurysms, trauma, and malignancy. Abbreviations used: IQR, interquartile range.
Operative details by age group.
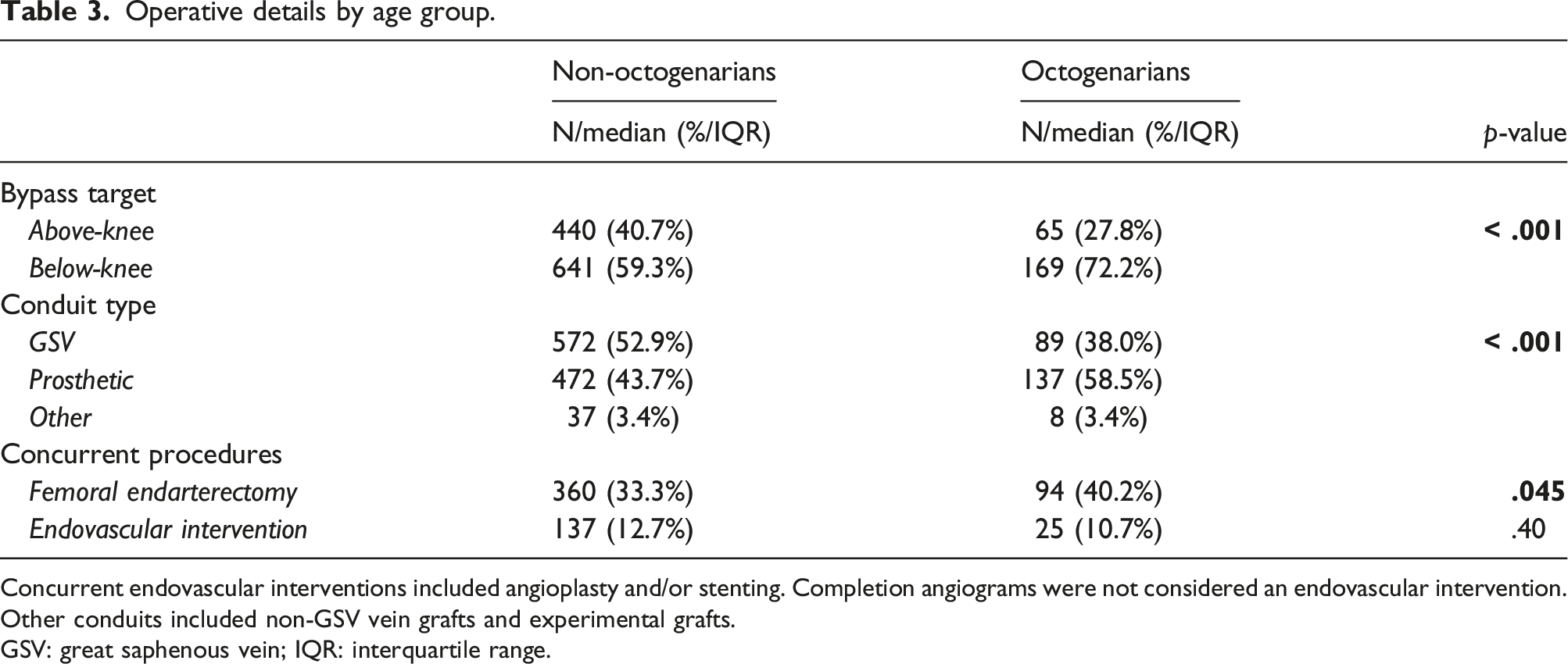
Concurrent endovascular interventions included angioplasty and/or stenting. Completion angiograms were not considered an endovascular intervention. Other conduits included non-GSV vein grafts and experimental grafts.
GSV: great saphenous vein; IQR: interquartile range.
Univariate analysis of postoperative outcomes.
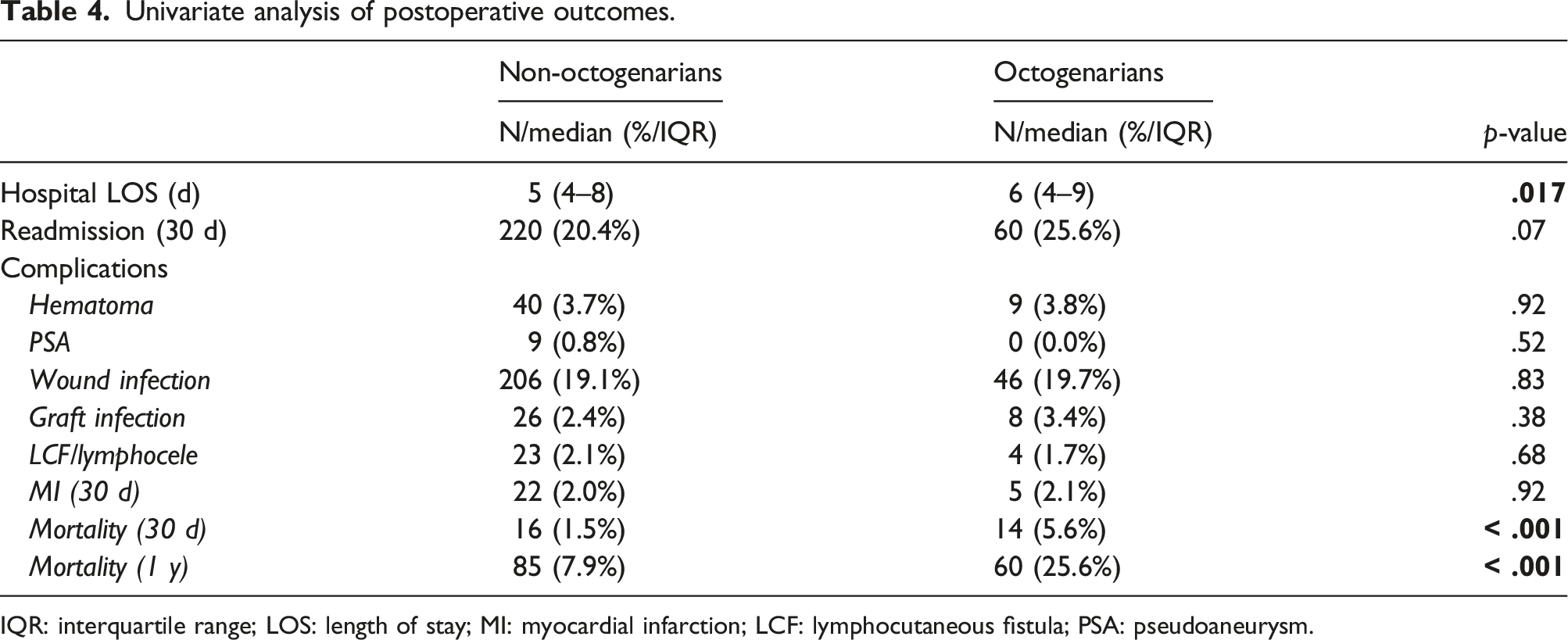
IQR: interquartile range; LOS: length of stay; MI: myocardial infarction; LCF: lymphocutaneous fistula; PSA: pseudoaneurysm.
The specific causes of 30-day mortality among octogenarians included myocardial infarction (n = 4), renal failure (n = 1), polytrauma (n = 1; bypass for traumatic limb ischemia), septic shock (n = 1; bypass for foot gangrene), stroke (n = 1), spinal cord ischemia following fenestrated endovascular aortic repair (n = 1; bypass for acute limb ischemia), fulminant C. difficile colitis (n = 1), and not reported (n = 4).
Multivariable analysis of postoperative outcomes.
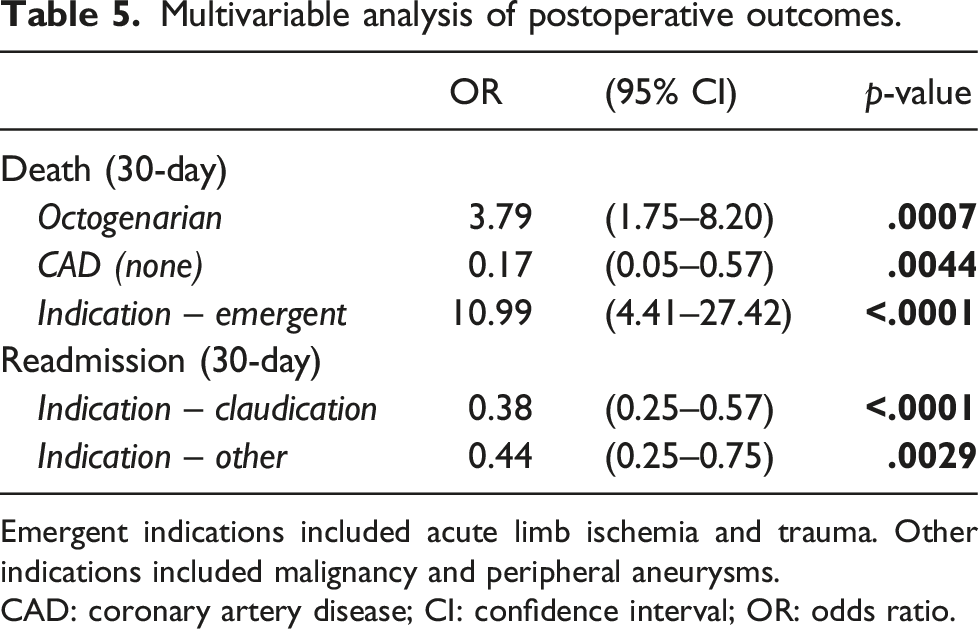
Emergent indications included acute limb ischemia and trauma. Other indications included malignancy and peripheral aneurysms.
CAD: coronary artery disease; CI: confidence interval; OR: odds ratio.
Discussion
In the present study, we investigated postoperative outcomes after femoropopliteal bypass in the octogenarian population. The overall hospital length of stay was longer among the octogenarian cohort, and 30-day mortality rate was 25.6% in octogenarians, compared to 7.9% in non-octogenarians. Even after accounting for patient comorbidities and operative factors, on multivariable analysis, age greater than 80 years was found to be an independent risk factor for postoperative mortality. Taken together, octogenarians undergoing bypass femoropopliteal bypass surgery have considerably worse postoperative outcomes, compared with non-octogenarians. These data may help further inform clinical decision making in this high-risk surgical population.
Octogenarians may be a high-risk patient population for any major surgical intervention. This relationship between advanced age and postoperative mortality has most thoroughly been investigated in the cardiac surgical literature.6,8–10 For instance, octogenarians have been shown to suffer worse outcomes after surgery for acute aortic dissection, spanning both type A and B classifications. 7 In light of these data, some providers have refrained from offering cardiac surgery to patients aged greater than 80 years, and consider advanced age a surgical contraindication16,17 While there exists a wealth of data on postoperative outcomes after cardiac surgery in octogenarians, data on vascular surgery outcomes in this patient population is limited.
This presents a dilemma, as the elderly constitute a significant percentage of the US population, and the prevalence of vascular disease increases substantially with age. 15 In this multi-institutional series, 17.8% of patients undergoing femoropopliteal bypass were over 80 years old (Figure 1(a)). Octogenarians more frequently underwent bypass for lower extremity tissue loss, whereas disabling claudication was more common in non-octogenarians. Moreover, both below-knee bypass targets and prosthetic conduits were more frequently encountered in octogenarians, each of which portends worse long-term outcomes. 18 Even after accounting for these factors, however, advanced age was found to be an independent predictor of postoperative mortality following femoropopliteal bypass.
Prior reports from Dermody et al. have also demonstrated worse outcomes after bypass among the elderly population. 19 In their analysis of the Vascular Study Group of New England (VSGNE) database, in-hospital mortality rates were highest among patients over 80 years compared to 50–79 and < 50 years (4.1% vs 1.5 vs 0.6%, p = .001). One-year mortality rates were also highest among octogenarians (25.7% vs 9.5% vs 5.9%, p < .001).
Our findings were similar in that octogenarians suffer higher post-bypass mortality rates. Interestingly, the VSGNE dataset demonstrated higher rates of comorbidities among the elderly, whereas octogenarians had similar rates of medical comorbidities in our study. Several hypotheses may explain this finding. First, our study was limited by small numbers (n = 1315). Notably, two comorbidities trended towards being greater among octogenarians, including coronary artery disease (68.4% vs 62.1%, p = .07) and congestive heart failure (35.0% vs 29.3%, p = .08) but did not meet statistical significance. A second reason may be surgical indication. Octogenarians were more likely to undergo bypass for rest pain and tissue loss compared with non-octogenarians (79.0% vs 60.9%, p < .001). While surgical indication was included in multivariate modeling, the presence of CLTI may reflect the presence of other medical comorbidities not reported in the RPDR database. To build upon this further, third, the bypass procedures themselves were disadvantaged among octogenarians, including below-knee bypass, prosthetic conduit, and concurrent femoral endarterectomy. While these variables were accounted for in the multivariable model, the combination of these factors undeniably increases the complexity of the bypass procedure itself, which is difficult to demonstrate statistically.
While the premise of this study was to compare outcomes between octogenarians and non-octogenarians, no specific chronologic age, in particular, should be considered a contraindication to surgery. Even though we report worse outcomes in this study, our aim was to provide necessary data to help inform clinical decision making, rather than prohibit elderly patients from obtaining the appropriate treatment. Naturally, there exists a wide variability in physiologic capacity with advanced age. 20 Recent studies have also shown that preoperative cardiac stress testing may not be accurate in predicting adverse perioperative events after vascular surgery.21,22 These details highlight the importance of sound clinical judgment and consideration of alternative treatment options, even if the patient has suitable anatomy for an infrainguinal bypass surgery. Ultimately, all patients deserve thoughtful clinical care, and the elderly population may warrant even greater attention to detail.
The primary limitation of this study is its retrospective nature, and our conclusions must be taken in context of the possibility of bias and incomplete data. Additionally, we did not investigate long-term outcomes in this study, such as amputation-free survival or graft patency, as this was outside of the scope of our investigation. Instead, we focused on short-term, postoperative outcomes in the octogenarian population, given that this is where the majority of physiologic insults occur following open lower extremity revascularization.
Conclusions
In conclusion, octogenarians undergoing bypass femoropopliteal bypass surgery suffer higher rates of postoperative mortality, compared with non-octogenarians. These data may help inform elderly patients prior to undergoing open lower extremity revascularization.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.