
Abstract
Foam sclerotherapy is considered an acceptable method to treat great saphenous vein (GSV) insufficiency, promoting occlusion of its trunk and eradicating reflux. Yet, certain technical points have not been standardized while issues regarding the ultrasonographic appearance of successful or acceptable GSV obliteration or the end-points of the method are not clearly defined. This article comments on the aforementioned using examples based on personal experience.
We read with enthusiasm the recent article by Karacalilar and Kutas reporting on the technical and clinical success of treating insufficient tortuous great saphenous veins (GSVs) with foam scleroterapy. 1 The authors document a technical success rate of 100% in 62 patients and significant decrease in Venous Clinical Severity Score (VCSS) scores. The successful occlusion rate was 88.7% in the 1st postoperative month while decreased further to 82.3% after 6 months of follow-up. 1 In our opinion, the latter reflects the ‘real-world’ experience and merits further attention and discussion.
Usually, the relevant studies report foam sclerotherapy results in GSV varicose veins based on eradication of reflux and/or the recanalization of GSV.2,3 The pioneers from Birmingham in GSV sclerotherapy have reported immediate eradication in GSV reflux above or below the knee in percentages greater than 95% even by a single sclerotherapy session, leaving visible varicose veins in 11.6% after one treatment.
3
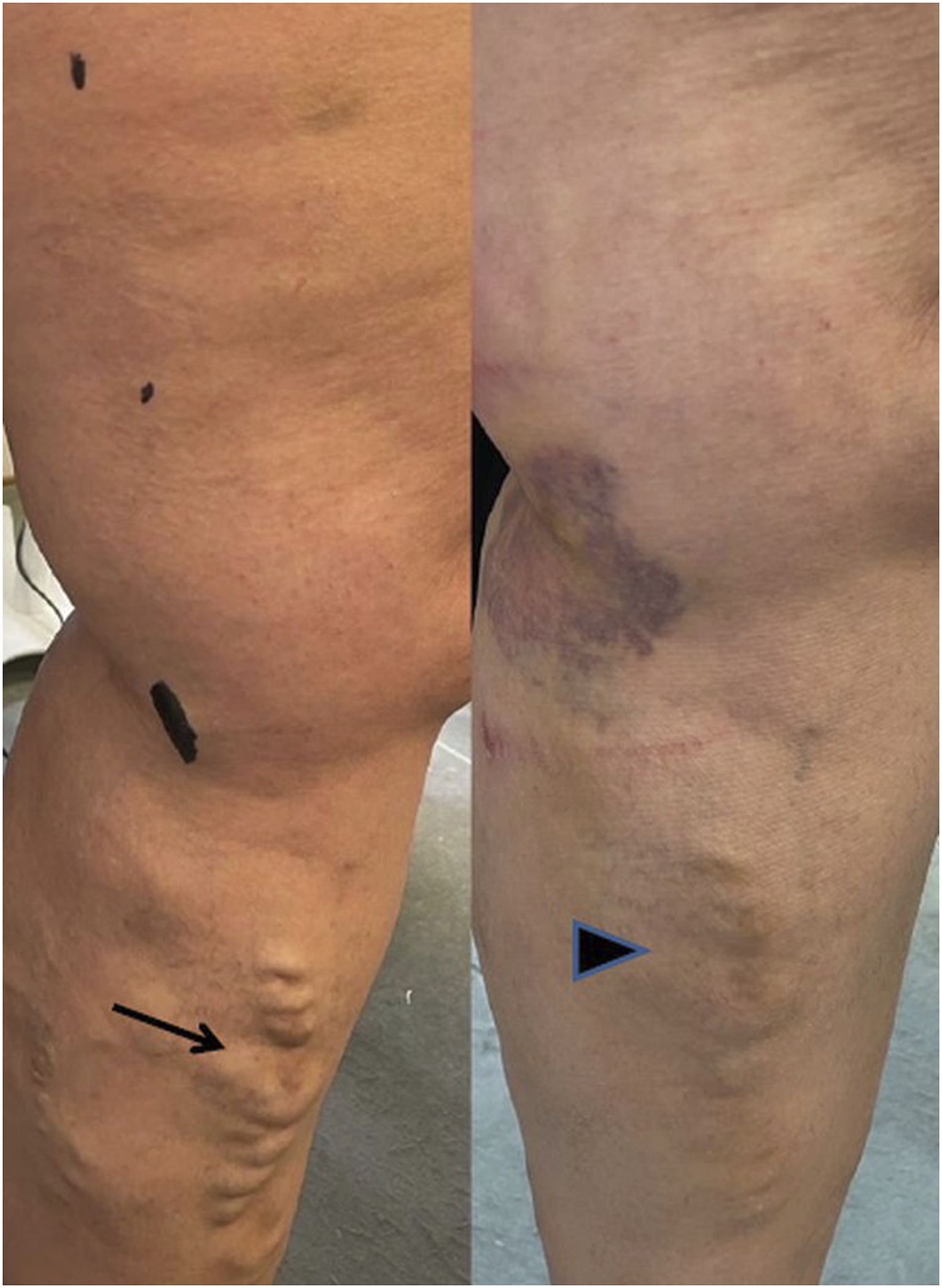
Yet, the eradication or decrease of reflux (especially below the knee) can significantly reduce the discomfort and other symptoms associated with the GSV varicose veins (Figure 1). Indeed, many of our patients often experience marked improvement in their symptoms after elimination of the GSV reflux after a single session, despite the persistence of below the knee varices, yet markedly deflated (Figure 2). Accordingly, no further treatment is requested by the patient. Therefore, the assessment of a venous severity scoring system, as the authors adapted, provides a useful and practical insight in the estimation of clinical – and not only aesthetic – results of GSV foam scleroterapy.
4
(A). Tortuous great saphenous vein (GSV) above and below the kne in a thin male patient. (B). Cannulation of the GSV below the knee and injection of polydocanole 3% foam. (C). Substantial clinical improvement with occlusion of the GSV with elimination of reflux. Female patient with varicose veins of the great saphenous vein below the knee (left, arrow). Successful occlusion with reflux eradication in the great saphenous vein via puncture above the knee and treatment with polydocanole 3% foam (Atossisclerol 3%, Kreussler Pharma, Wiesbaden) led to immediate alleviation of discomfort symptoms despite the persistence of patent veins (right, arrowhead). The patient declined further treatment.
Another point that needs further clarification in future studies is the ultrasonographic characterization of the ‘mechanism’ leading to reflux eradication, as the latter is defined as ‘occlusion of the treated saphenous trunk assessed by a lack of compressibility and absence of any flow’.
2
The foam injection aims to immediate destruction of the vein endothelium and spasm (Figure 3). Yet, despite application of a bandage-Class II stocking combination immediately and during the first postoperative days, we often see in follow-up sessions a thrombotic appearance of the GSV which still remains ‘incompressible without flow’, thus in alignment with clinical success, especially since this is not accompanied with symptoms of thrombophlebitis (i.e. redness and pain).
5
In our experience, the patient’s compliance and, mainly, the body mass index affects significantly the efficacy of stockings in maintaining the GSV collapsed and obilterated rather than thrombosed and occluded. Interestingly, a good point for further discussion would be the existence of any correlation between the thrombosed rather than obliterated GSV state and mid-term reocclusion. Immediate spasm and collapse of the great saphenous vein trunk after 3% polydocanole foam injection (arrow).
Finally, an ill-discussed issue remains whether two-point insertion cannulae at the level of the knee and above the ankle (Figure 4) for sclerotherapy along the entire length of GSV would provide better results compared to single cannulation in cases of GSV varicose veins below the knee, obviating the need for second therapeutic session and further declining the incidence of recanalization. Catheterization of great sephenous vein below the knee and above the ankle.
Once again, we congratulate the authors for sharing their ‘real-world’ experience and anticipate for further discuss and improvement of this technique.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.