
Abstract
Background
Acute limb ischemia (ALI) is an emergency vascular pathology in which perfusion is disrupted in the lower extremity and threatens extremity viability. The admission blood glucose (ABG)/estimated average glucose (eAG) value has recently been shown as a prognostic marker in acute cardiovascular events. In this study, we aimed to investigate the predictive role of an ABG/eAG value in predicting development of early postoperative major amputation after emergency thromboembolectomy operations in patients presenting with ALI.
Method
Patients who admitted to our hospital with ALI between November 01, 2016 and September 01, 2021 and underwent surgical thromboembolectomy were retrospectively included in the study. Patients who did not undergo postoperative limb amputation were recorded as Group 1, and patients who underwent major amputation in the early postoperative period (in-hospital), were recorded as Group 2.
Results
The median age of the 226 patients included in Group 1 and 72 patients in Group 2 were 58 (34–86) years and 69 (33–91) years, respectively (p<0.001). In univariate analysis, in-hospital amputation was found to significantly correlate with age>70 years (odds ratio [OR]: 1.914, 95% confidence interval [CI]: 1.351–2.319, p<0.001), PAD (OR: 1.698, 95% CI: 1.270–1.992, p = 0.002 re-embolectomy (OR: 2.184, 95% CI: 1.663–3.085, p < 0.001), admission Rutherford class (OR: 0.762, 95% CI: 0.591–0.859, p = 0.032), admission time>6 h (OR: 1.770, 95% CI: 1.480–1.152, p = 0.009), ABG (OR: 1.275, 95% CI: 1.050–1.790, p < 0.001), and ABG/eAG (OR: 1.669, 95% CI: 1.315–2.239, p < 0.001).
Conclusion
According to our study, we can predict patient groups with a high risk of major amputation with the ABG/eAG value calculated from the blood values of the patients at the time of admission.
Introduction
Acute limb ischemia (ALI) is an emergency vascular pathology in which perfusion is disrupted in the lower extremity and threatens extremity viability. Although this situation is mostly caused by cardiac thrombus, it can also occur due to atherosclerosis and vascular aneurysms. This condition has a very high morbidity and 1-year amputation rates range from 11 to 37%. 1 As soon as these patients are diagnosed, urgent vascular intervention require to be planned.
Disorders in glucose metabolism increase the mortality and morbidity of cardiovascular diseases. 2 In addition, while acute hyperglycemia causes prothrombotic events, it increases oxidative stress and leads to endothelial dysfunction. 3 This situation affects the development of adverse events after acute cardiovascular events, regardless of whether the person has diabetes mellitus. 4 In this way, the admission blood glucose (ABG)/estimated average glucose (eAG) value has recently been shown as a prognostic marker in acute cardiovascular events.5,6
In this study, we aimed to investigate the predictive role of an ABG/eAG value in predicting development of early postoperative (in-hospital) major amputation after emergency thromboembolectomy operations in patients presenting with acute lower extremity ischemia.
Methods
Patients who admitted to our hospital with ALI between November 01, 2016 and September 01, 2021 and underwent emergency surgical thromboembolectomy were retrospectively included in the study. The data of the patients were obtained from the hospital registry system and patient files. Demographic data of all patients, blood values at the time of admission and postoperative complications were recorded. Patients with ischemic foot due to active or chronic infection (Diabetic foot and/or Buerger disease), patients with a diagnosis of hypercoagulable states, those with oncological disease, those with liver and/or kidney insufficiency, patients who had previously undergone vascular surgery, patients with irreversible tissue damage (Rutherford class III), or patients who do not need urgent surgery (Rutherford class I) were excluded from the study. After the exclusion criteria, 298 consecutive patients were included in the study (Figure 1). Patients who did not undergo postoperative limb amputation were recorded as Group 1, and patients who underwent major amputation in the early postoperative period (in-hospital) were recorded as Group 2. Flowchart of patient enrollment.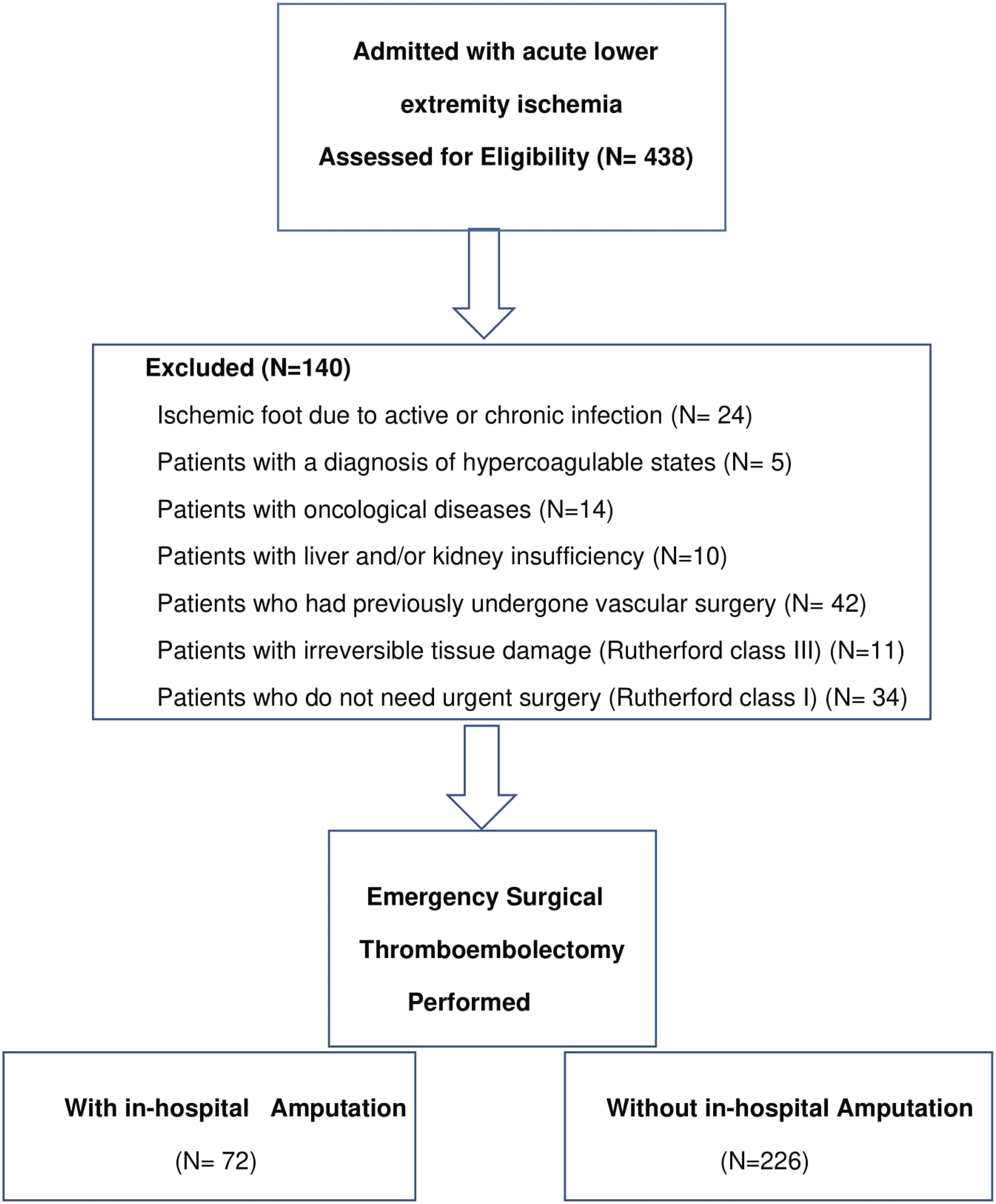
Diagnosis of Acute Lower Extremity Ischemia and Treatment
Detailed anamnesis was obtained from all patients and physical examinations were performed. Clinical diagnoses were supported by Doppler ultrasonography. Angiography was performed in patients with extensive atherosclerotic disease. Patients with a stenosis percent of 50% or above in the doppler ultrasonography or angiography images were considered as having peripheral arterial disease (PAD). After the diagnosis, Tromboembolectomy operations were performed emergently by Fogarty catheter (3–7 french) under local anesthesia and mild sedation. Tromboembolectomy was terminated in cases in which thrombus or embolism material was suggested to be completely cleared in both proximal and distal vessel segments and anterograde and retrograde flow was suggested to be sufficient. After the operation, patients were followed up in intensive care unit for at least 1 day and given heparin infusion (activated clotting time remained between 200 and 250 s) and then continued with low molecular height heparin (1 mg/kg, sc) for a week. Also 100 mg/day acetylsalicylic acid and clopidogrel in 75 mg/day dose was administered from the first day. We did not use thrombolytic therapy in our patient group. Re-embolectomy decision was made according to the postoperative clinic and pulse monitoring. Amputation was performed by a joint decision with the Department of Orthopedics in patients with ongoing ischemia for which demarcation line was developed postoperatively. The below-knee (in 58 patients) and above-knee (in 14 patients) amputations were defined as major lower extremity amputations.
Calculation of ABG/aAG
Blood parameters of all patients were obtained from blood samples taken from peripheral venous structures during hospitalization. ABG/eAG was then acquired with the following formula: 6
ABG/eAG = Admission blood glucose levels (mg/dl)/[(28.7 × glycosylated hemoglobin %) - 46.7].
Statistical Analysis
Statistical analysis was performed with the SPSS 21.0 (IBM Statistical Package for the Social Sciences Statistic Inc. Version21.0, Chicago, IL, USA) program. Student’s t-test was used for numerical values with normal distribution, and Mann–Whitney U test was utilized for numerical data without normal distribution. Numerical values were expressed as mean (standard deviation) or median (minimum-maximum). The Chi-square test was used to compare categorical variables. p<0.05 was considered statistically significant. First, univariate logistic regression analysis was utilized. Then, variables associated with a p value ≤0.20 in univariate analyses were considered for inclusion in the multivariate analyses. Multivariate logistic regression analysis Model 1 with ABG and Model 2 with ABG to eAG ratio were applied. Receiver Operating Characteristic (ROC) analysis was performed to evaluate the predictive value of ABG/eAG for amputation and the area under the curve (AUC) was calculated.
Results
Demographic, preoperative labaratory features and peroperative data of the patients.
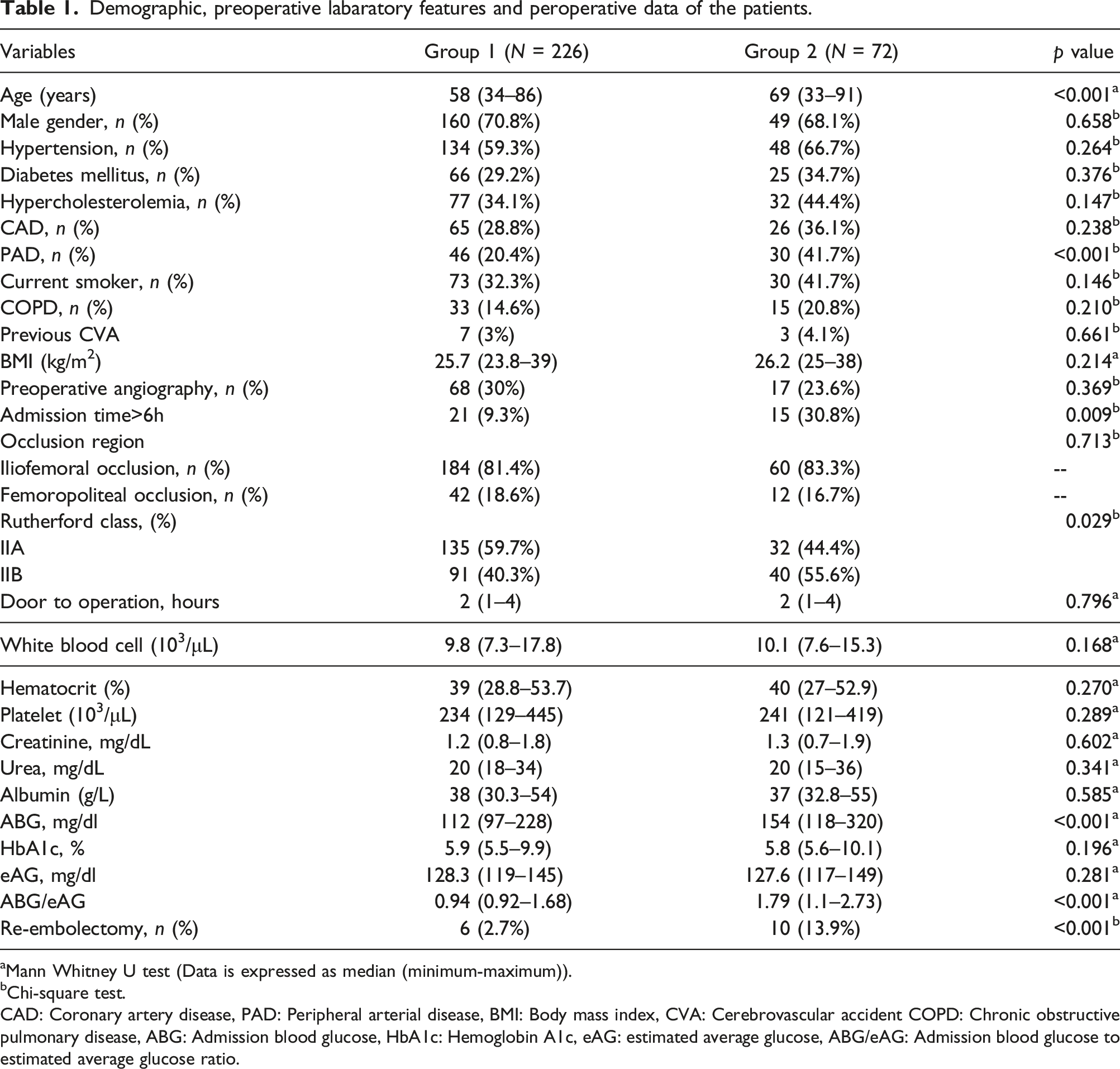
aMann Whitney U test (Data is expressed as median (minimum-maximum)).
bChi-square test.
CAD: Coronary artery disease, PAD: Peripheral arterial disease, BMI: Body mass index, CVA: Cerebrovascular accident COPD: Chronic obstructive pulmonary disease, ABG: Admission blood glucose, HbA1c: Hemoglobin A1c, eAG: estimated average glucose, ABG/eAG: Admission blood glucose to estimated average glucose ratio.
Patients’ preoperative laboratory values were summarized in Table 1. There was no significant difference between the groups in terms of white blood cell, hematocrit, platelet, urea, albumin, HbA1c, and eAG levels. In Group 2, ABG and ABG/eAG were significantly higher (p<0.001, p<0.001, respectively). Mean time from admission to the hospital to definitive embolectomy was 2 h (range: 1–4 h). Re-embolectomy was performed in 16 patients. Re-embolectomy rates were significantly higher in Group 2 (p<0.001) (Table 1).
Logistic regression analysis to identify factors affecting development of postoperative amputation after surgical thromboembolectomy.
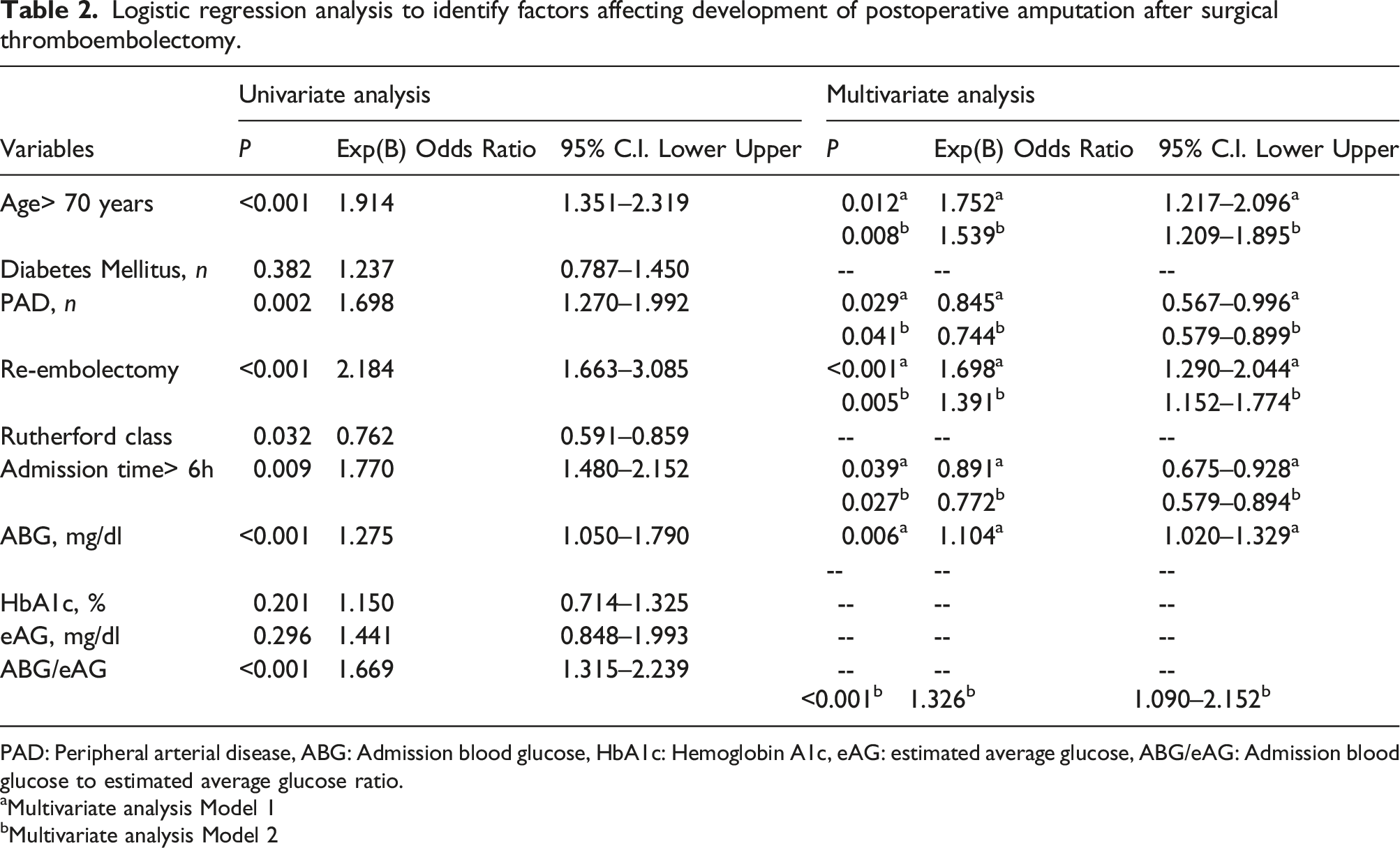
PAD: Peripheral arterial disease, ABG: Admission blood glucose, HbA1c: Hemoglobin A1c, eAG: estimated average glucose, ABG/eAG: Admission blood glucose to estimated average glucose ratio.
aMultivariate analysis Model 1
bMultivariate analysis Model 2
ROC curve analysis revealed that the cut-off value for ABG/eAG was 1.55 (AUC: 0.712, 95% CI: 0.632–0.792, p < 0.001, 89.4% sensitivity and 49.6% specificity) (Figure 2). ROC (Receiver operation characteristic) curve and AUC (Area under the curve) for admission blood glucose (ABG)/estimated average glucose (eAG) ratio for predicting in-hospital amputation. (Cutoff: 1.55, AUC: 0.712, 95% CI: 0.632–0.792, p< 0.001, 89.4% sensitivity and 49.6% specificity).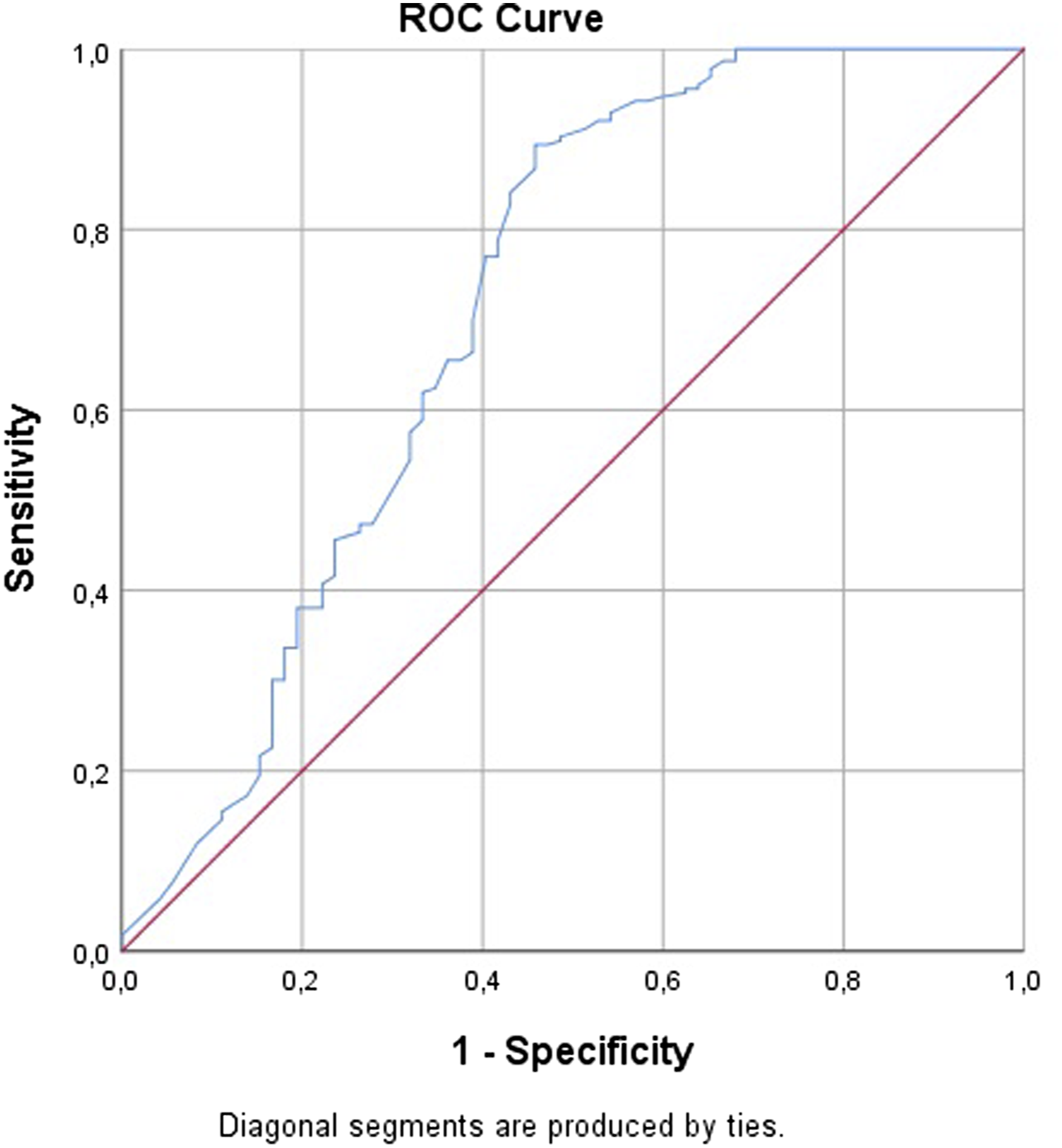
Discussion
Acute lower extremity ischemia is a serious clinical condition that suddenly threatens the vitality of the lower extremity and progresses with extremity loss, unless crucial interventions are performed. In addition to the psychological trauma, it produces in individuals loss of a limb also results in labor loss in societies and considerably increases the cost of treatment. Therefore, urgent intervention in these patients and analysis of amputation risk factors are very important. In the current study, to the best of our knowledge, we first identified the ABG/eAG value as an independent risk factor for early amputations after surgical thromboembolectomy, in patients presenting with ALI.
It has been shown that hyperglycemia occurring in acutely developing clinical conditions is related to poor clinical outcomes, regardless of whether the patients are diabetic. 7 Acutely occurring hyperglycemia participates in the activation of prothrombotic pathways, increases oxidative stress, causes endothelial dysfunction, and thus disrupts microvascular circulation. 3 It has been shown that acute hyperglycemia is characterized by larger infarct areas in patients with myocardial infarction. 8 HbA1c is a valuable parameter used in the long-term follow-up of diabetic patients. In previous studies conducted, high HbA1c levels were found to be associated with cardiovascular mortality and morbidity, regardless of whether the patients were diabetic. 9
In an experimental study conducted on rats by Levigne et al., they found that hyperglycemia increased susceptibility to necrosis in ischemic extremities. 10 In a recent study by Kronfli et al., 505 patients who underwent lower extremity bypass surgery were included and the effect of hyperglycemia developing immediately after surgery on clinical outcomes was investigated. At the end of the study, the authors found that elevated blood glucose levels immediately after surgery were significantly associated with 30-day amputation rates. They showed that this situation is also associated with poor long-term outcomes. 11 Surgery undoubtedly creates a situation of stress for the body and in their study; it was revealed that the risk of amputation increased according to the hyperglycemia response to surgical stress in patients. In our study, similarly, the hyperglycemia response of the body to acute extremity ischemia was significantly higher in patients who developed amputation.
In a study by Goldman et al., the effect of glycemic control on extremity amputations was investigated in peripheral arterial patients with Type 2 DM. In the multivariate analysis performed in this randomized controlled study, which included 124 patients, HbA1c was shown to be a strong predictor of the occurrence of amputation (HR 2.07 per 1% increase in HbA1c, 95% CI 1.67 to 2.57, p <0.0001). 12 Our study consisted of diabetic and non-diabetic patients with ALI, and HbA1c levels were higher, although not statistically significant, in patients with early amputation after surgical embolectomy, at the end of our study. In studies conducted in the literature, high HbA1c levels have also been shown as a risk factor for cardiovascular mortality and morbidity in non-diabetic patients. 13
Considering the negative effects of acute hyperglycemia and the negative effects of the HbA1c value on non-diabetic patients, the effect of the ABG/eAG ratio on cardiovascular diseases has been investigated in recent years. In a prospective study conducted by Marenzi et al. in 2018, the predictive role of the ABG/aAG ratio in patients presenting with acute myocardial infarction (AMI) was investigated. The primary endpoints of the study, which included 1553 patients, were mortality, pulmonary edema, and the development of cardiogenic shock. The authors found the ABG/eAG value to be more predictive than baseline glucose values in predicting the primary outcome, in all patients and patients with isolated DM. 14 In a similar study conducted by Gao et al. in 2019, the ABG/eAG value was shown to be a significant predictor of prognosis in AMI patients. 5 In a recent study conducted by Simsek et al. and published in 2021, the predictive role of the ABG/eAG value in showing the development of no-reflow after acute MI was investigated. In this study, which included 955 patients, patients after percutaneous coronary intervention were divided into two groups, namely, those who developed no-reflow (N = 206) and those who did not (N = 749). As a result of the multivariate analysis, the ABG/eAG value (OR: 2.274, p < 0.001) was determined more predictively (OR: 1.869, p<0.001) according to the relevant target artery diameter (OR: 0.844, p<0.001) and thrombus grade. 6 In our current study, we found ABG/aAg to be an independent predictor of early amputation in patients who presented with ALI and underwent surgical thromboembolectomy.
In patients presenting with acute lower extremity ischemia, advanced age, and the duration of admission to the hospital after the first complaint, that is, the prolongation of ischemia and the presence of underlying atherosclerotic disease, are also known as factors that increase the risk of amputation. 15 In the study conducted by Saskin et al., in which the predictive effects of inflammatory parameters on amputation were investigated in patients with acute arterial occlusion, a significant correlation was found between hospital admission time and amputation (OR:1.11, p = 0.07). 16 In another study investigating the risk factors for amputation in patients with acute arterial embolism, a time to admission greater than 6 h was shown as a strong and independent predictor of amputation (OR: 40.3, 95% CI: 5.3–304.9, p = 0.0013). 17 In our study, being over 70 years old, 6 h after the first complaint and having atherosclerotic peripheral vascular disease, were independent predictors of amputation occurrence.
Rutherford’s ALI classification divides an extremity into variable damaged categories. 18 In our study, we included patients with Rutherford IIa and IIb who underwent emergency acute thromboembolectomy. And, there was a higher proportion of Rutherford IIb cases in the amputation group (p = 0.029).
All patients in our study underwent surgical thromboembolectomy with a Fogarty catheter. The use of these catheters also affects surgical success: failure to properly inflate the balloon can lead to endothelial damage. Although this situation triggers thrombosis in the early period, it can also lead to complications, such as pseudoaneurysm, in the late period. In an experimental study model on rabbits, the development of intimal hyperplasia due to a Fogarty balloon catheter was demonstrated histopathologically. 19 In a case report by Smith et al., a case of progressive intimal hyperplasia developing in the third month after embolectomy was reported. 20 In our study, we identified early re-embolectomy as an independent predictor of amputation development, in both multivariate analysis models.
The most important limitations of our study are that it is a single-center retrospective study and the small number of patients. In addition, due to the retrospective design of our study, inflammatory parameters such as interleukin-6 and myeloperoxidase could not be evaluated in the perioperative period.
Conclusion
Extremity losses are a very important socioeconomic problem in all societies. Lower extremity thromboembolism is an important cause of extremity loss, and amputation rates can be reduced with correct and timely intervention. In this study, we showed that the ABG/eAG value calculated at the time of presentation in thromboembolism cases, can predict the risk of amputation. According to our study, we can predict patient groups with a high risk of amputation with the ABG/eAG value. As an inexpensive and available laboratory marker, ABG/eAG could be used for the risk stratification of acute lower extremity ischemia patients on admission.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Ethical approval
The study was approved by our hospital clinical research ethics committee (Approval no: 2011-KAEK-25 2022/03–12).