
Abstract
Background
Despite being rare, pancreaticoduodenal artery aneurysms (PDAAs) carry a risk of rupture of up to 50% and are frequently associated with coeliac artery occlusion.
Methods
PubMed and Embase databases were searched using appropriate terms. The systematic review was conducted according to PRISMA guidelines.
Results
We present the case of a 2 cm pancreaticoduodenal artery aneurysm pre-operative angiography demonstrated that the coeliac artery was occluded and the pancreaticoduodenal artery was providing collateral blood supply to the liver. Treatment was a staged hybrid intervention inclusive of an aorto-hepatic bypass using a 6 mm graft, followed by coil embolisation of the aneurysm. We also present a systematic review of the management of PDAAs. Two hundred and ninety-two publications were identified initially with 81 publications included in the final review. Of the 258 peripancreatic aneurysms included, 175 (61%) were associated with coeliac artery disease either occlusion or stenosis. Abdominal pain was the main presentation in 158 cases. Rupture occurred in 111 (40%) of patients with only ten (3.8%) cases being unstable on presentation. Fifty (18%) cases were detected incidentally while investigating another pathology. Over half the cases (n=141/54.6%) were treated by trans arterial embolisation (TAE) alone, while 37 cases had open surgery only. Twenty-one cases needed TAE and a coeliac stent. Seventeen cases underwent hybrid treatment (open and endovascular). Sixteen cases were treated conservatively and in 26 cases, treatment was not specified.
Conclusion
PDAAs are commonly associated with coeliac artery disease. The most common presentation is pain followed by rupture. The scarcity of literature about true peripancreatic artery aneurysms associated with CA occlusive disease makes it difficult to assess the natural history or the appropriate treatment. Revascularisation of hepatic artery is better done with bypass in setting of median arcuate ligament compression and occluded celiac trunk.
Introduction
Visceral artery aneurysms (VAAs) are rare with an incidence of between 0.01% and 0.2%. 1 The clinical presentation is non-specific ranging from incidental finding to rupture and shock. Being rare, the actual incidence of rupture is unknown.1,2 Pancreaticoduodenal artery aneurysms (PDAAs) comprise about 2% of visceral artery aneurysms. Multiple pathologies are reported to be involved in its aetiology, including pancreatitis, surgical trauma, collagen vascular disease and occlusion or stenosis of the coeliac artery due to arteriosclerosis or median arcuate ligament compression. The risk of rupture in these aneurysms is independent of the size of aneurysm 3 treatment of PDA aneurysms appropriate even if asymptomatic. Endovascular treatment is considered to be the first line treatment due to its lower morbidity and mortality; however, flow to the hepatic artery should not be compromised.4,5
Our aim is to present a case report of a patient with a PDAA and coeliac artery occlusion in addition to a systematic review of this rare condition.
Case report (Figure 1)
A 39-year-old lady presented with an incidental finding of a PDA aneurysm on CT following four episodes of intermittent abdominal pain, one of which resulted in ED attendance. The epigastric pain was associated with vomiting, initially of undigested foods and then became bilious in nature. The patient also complained of intermittent dyspepsia, with no identifiable triggers. She denied haematemesis, melaena, diarrhoea, constipation or weight loss. Her abdominal exam was unremarkable. Her past medical history was significant for a papillary thyroid carcinoma (thyroidectomy 2010), non-smoker, no history of portal hypertension or liver disease. CTAP revealed a 2.7 cm aneurysm involving the proximal inferior pancreaticoduodenal artery with no other aneurysms and occluded proximal celiac artery.
The case was discussed in our Multi-disciplinary meeting (MDT) and the decision was to treat the aneurysm giving the young age of the patient and size of aneurysm. Initially coil embolisation was considered; however, first angiography demonstrated complete occlusion of the coeliac artery from the origin to bifurcation and the PDA supplied the entire hepatic circulation. This led to concern that embolisation of the aneurysm would risk foregut ischaemia and so embolisation was aborted and a decision was made to perform first a bypass from the aorta to the hepatic artery and to embolise the aneurysm at a later stage. (Figure 1(a)–(d)) Angiographic images for the aneurysm pre-embolisation and after A.B.C.D first preoperative angiogram showing the aneurysm and collateral vessels E.F second angiogram images before and after embolisation.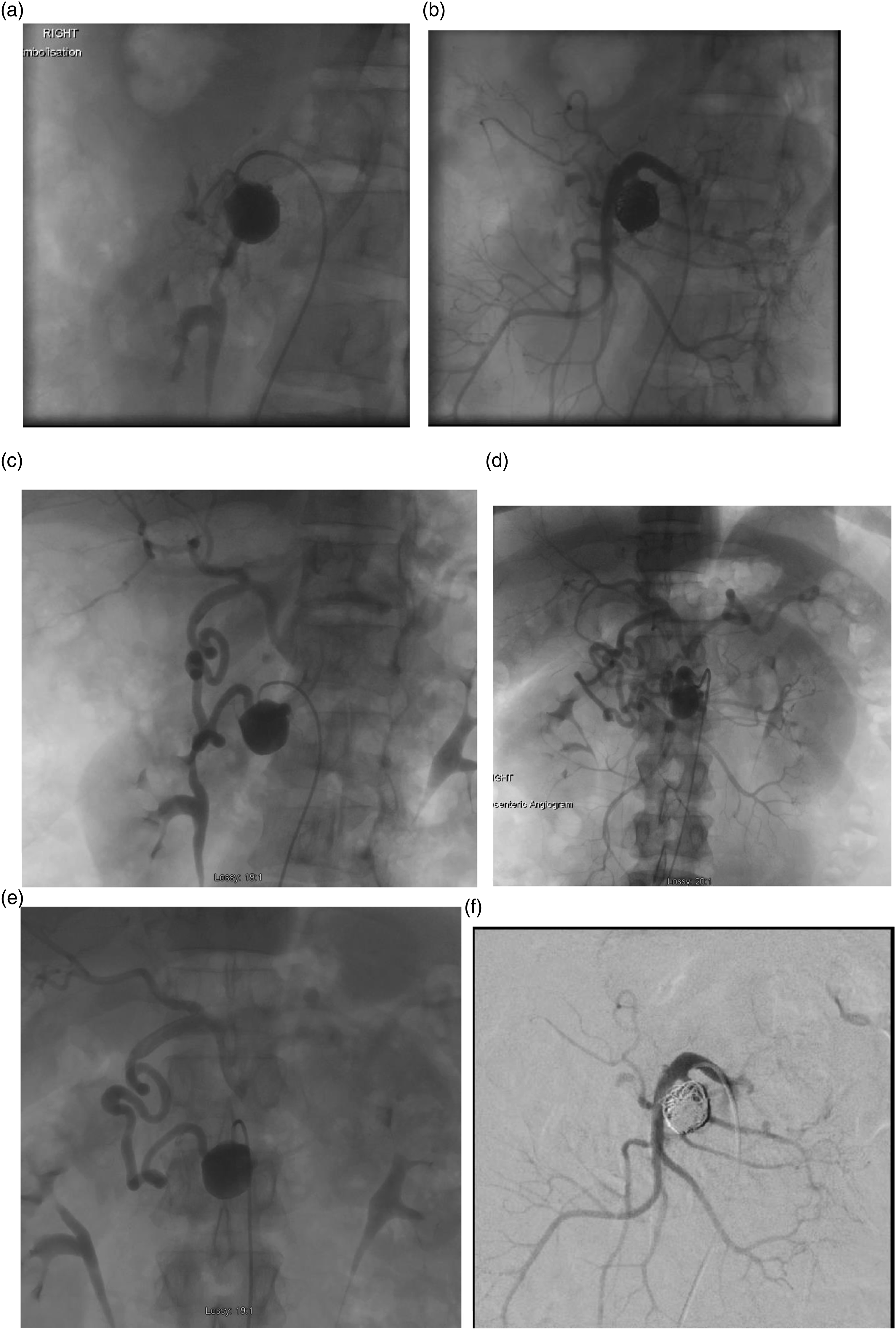
The operation was performed using a transabdominal approach with control of the supraceliac aorta at the hiatus. The hepatic artery was controlled at the lesser sac. The median arcuate ligament was divided as was very tight and we performed aorto-hepatic bypass was performed using 6 mm Dacron end to side anastomosis for both aorta and hepatic artery. The patient recovered well after the bypass and was discharged home for scheduled embolisation of the aneurysm 2 weeks later. The second stage involved Right femoral access and through the Superior mesenteric artery, cannulation of inferior PDA using microcatherters and 0.014 inch wire with help of our interventional radiology, coils were inserted in the aneurysm to occlude the aneurysm itself and completion angiogram showed complete occlusion of the aneurysm (Figure 1(e) and (f)). Follow-up CTA after 6 weeks and 6 months revealed complete occlusion of the aneurysm and a patent bypass with planned yearly CTA to assess the bypass.
Systematic review
Aim
To review the treatment of PDAAs in association with coeliac artery disease.
Eligibility criteria
Studies were included if they were prospective or retrospective studies which evaluate the relation between PDAAs and coeliac artery occlusive disease. Studies were excluded if they had insufficient data, duplicated studies, non-English, consisted of a comment or letter to a study or included aneurysms in other visceral arteries.
Literature search strategy
The literature review was conducted in PubMed and Embase databases. Two groups of key words were used and combined with Boolean operator ‘AND’. The first group comprised: ‘pancreaticoduodenal artery aneurysm’ or ‘gastroduodenal artery aneurysm’. The second group was: celiac artery OR celiac bypass OR aortohepatic bypass OR celiac artery stent. Additional studies were also examined from references of original studies on the topic. All studies were carefully examined, and selected as per the eligibility criteria outlined above. Each publication was assessed as regards patient characteristics, aneurysm site, presentation, treatment and outcome if mentioned. PRISMA was followed.
Data abstraction and quality assessment
Characteristics of included paper.

Abbreviation: GSV:GREAT SAPHENOUS VEIN. NS: NON SIGNIFICANT. FU: FOLLOW UP. TTT: TREATMENT.
Results
Two hundred and ninety-two publications were identified and after duplicated publications were removed, 277 were included for initial assessment. 177 publications were excluded based on title and abstract as they did not fulfilling the search criteria. A further 19 reports were excluded as they included coeliac artery aneurysms leaving 81 publications for inclusion in the review. (Figure 2) Flowchart of search.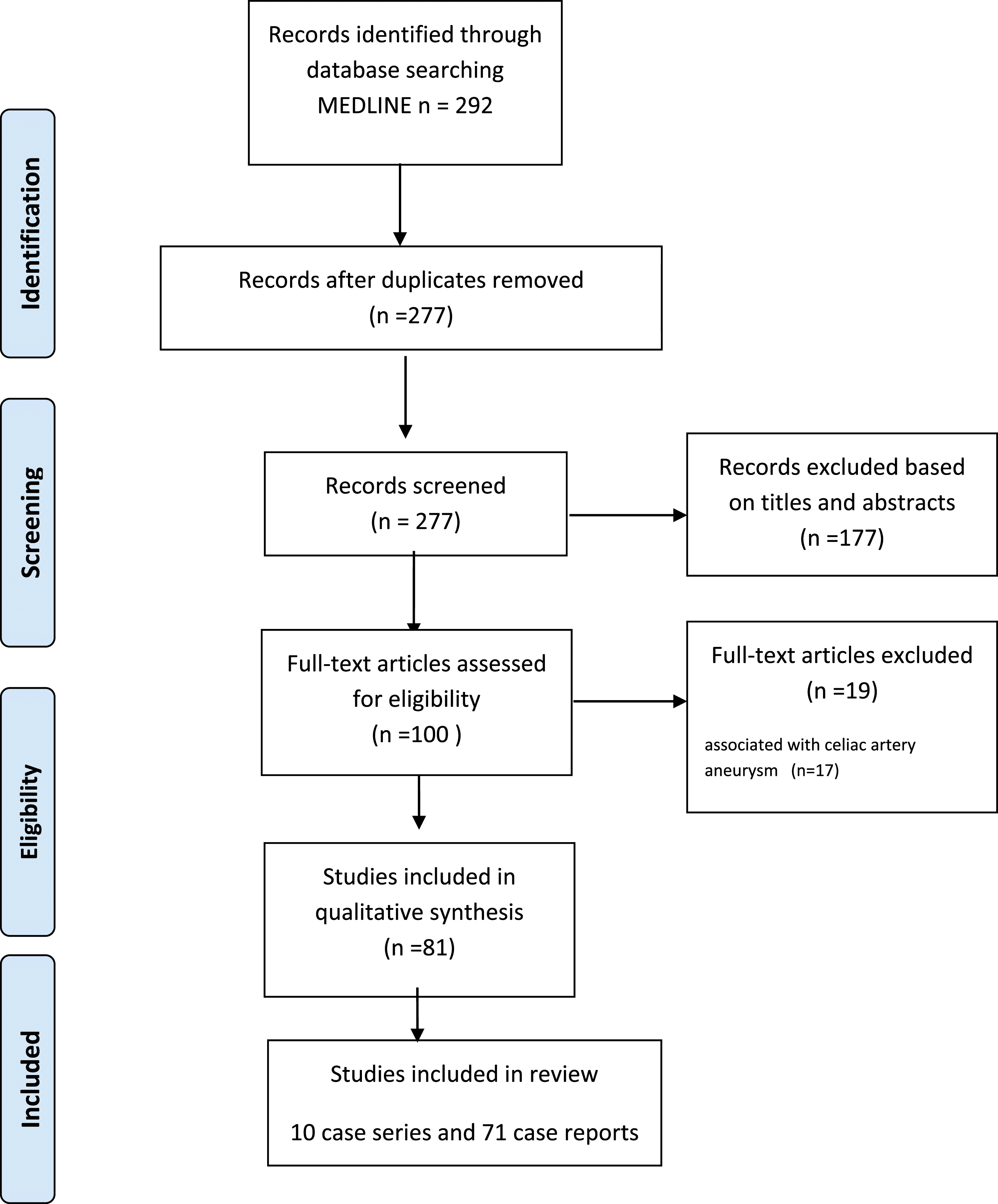
Table 1 summarises the main findings of the eligible studies. Seventy-one were case reports and 10 studies were case series. No randomised controlled studies were identified. Using the Down’s and Black Tool, quality assessment of included studies ranged between poor and moderate quality.
Presentation
Two hundred and fifty-eight pancreaticoduodenal aneurysms (PDAAs) were identified, 175 (61%) were associated with coeliac artery disease either occlusion or stenosis.
Abdominal pain was the main presentation in 158 cases (61%) (Figure 3) Rupture occurred in 111 (43%) patients with only ten patients (3.8%) being unstable on presentation. Fifty (19%) cases were detected incidentally while investigating another pathology. Nine cases (3.9%) presented with vomiting secondary to duodenal obstruction. Two cases (0.89%) presented with rectal bleeding and two cases presented with obstructive jaundice from compression on the common bile duct. (Figure 3) Presentation of PDAAs according to literature review.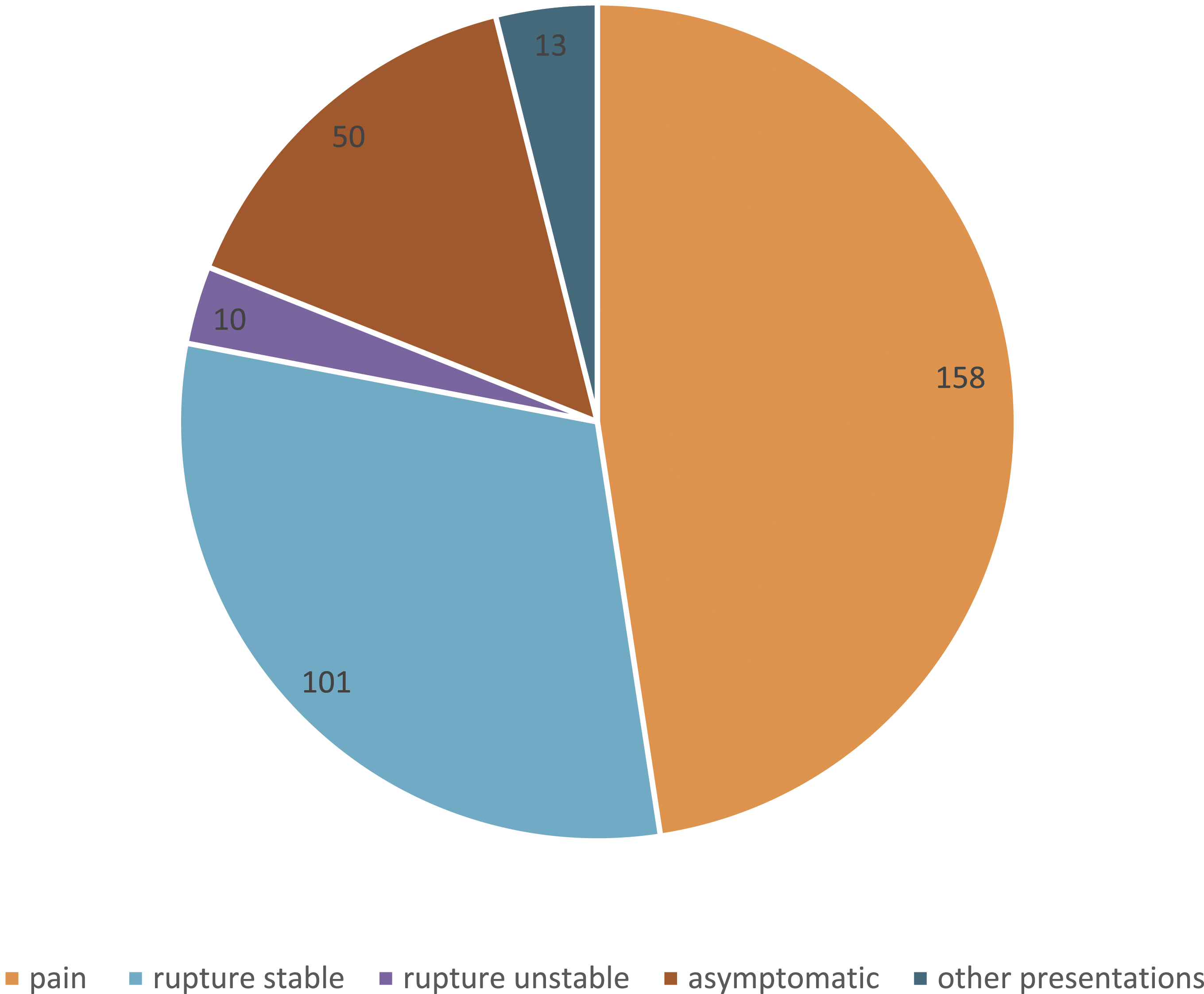
Treatment
One hundred and forty-one (54.6%) cases were treated by coil embolisation alone. Of these five failed and subsequently three underwent open surgical repair, one, CT guided injection and one was treated conservatively.
Thirty-seven (14%) cases had open surgery alone. Sixteen of them had exclusion and bypass with nine cases have additional Median Arcuate Ligament release (MALR). Eleven cases had exclusion alone while three cases had MALR release alone and seven cases had exclusion with MALR.
Twenty one (8%) cases underwent TAE and coeliac stenting. Three stents were occluded on follow up with one having subsequent restenting with a high radial force stent and the other two patients were treated conservatively. One patient of this group had additional open surgery for decompression after compartment syndrome from rupture.
Seventeen (6.5%) cases underwent hybrid treatment. Nine cases had TAE and bypass with six performed at the same sitting. Inflow was from the aorta in seven cases, right renal in one case and right common iliac artery in the remaining case. Seven cases needed TAE and median arcuate ligament release, four were performed at the same sitting and one before and one after TAE. One case had an aorto-hepatic bypass and intraoperative US guided coiling of the PPAA. Sixteen (6.2%) cases underwent conservative treatment. In 26 (10%) cases, treatment was not specified. (Figure 4) Treatment of PDAAs according to literature review.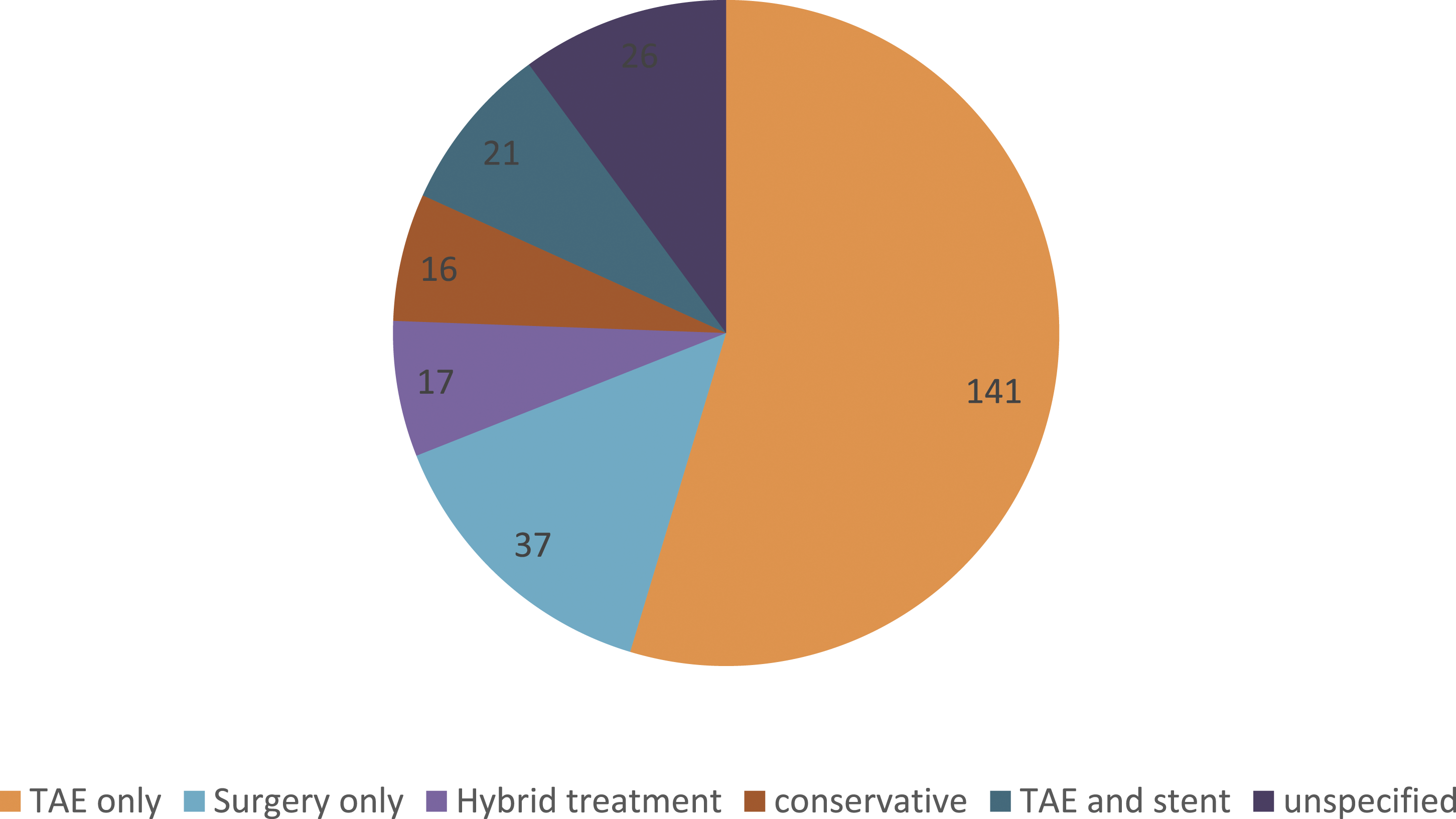
Follow-up
Forty-two studies reported follow-up. Two stents were occluded on follow-up. Both were treated conservatively. One bypass was occluded on follow-up with no further treatment required. One study reported liver injury during the bypass surgery and another study reported graft infection which was treated conservatively. Seven cases died with three deaths in endovascular group and two in open surgery group and one died just before the surgery. Yamena and his colleagues reported that after ligation of PDA aneurysm, it continued to enlarge on follow-up and the patient developed a new PDAA besides the excluded one and these aneurysm regressed only after aortohepatic bypass was performed with normalisation of the pressure in peripancreatic arterial arcade.
Discussion
PPAAs are considered a rare form (2%) of all visceral artery aneurysms (VAAs) and are commonly associated with coeliac artery disease which has been reported in literature between 59% and 95%. We think that the common association between PDAAs and celiac artery occlusive disease is due to a haemodynamic change in the peripancreatic arterial arcade with higher pressure through collaterals with resultant increase in the incidence of PPAAs formation.7,8
Yoon and his colleagues 9 had developed two theories to examine the relation between the CA stenosis and PDAAs development. They used electrical simulation circuit to test their theory. The stenosis first theory showed that when CA stenosis develops, it is associated with increase flow in peripancreatic arterial arcade and due to high pressure in the aorta it favours PDAAs development through higher flow through these weak collaterals. The other theory, the aneurysm first theory suggests that when a PDAA develops, it steals the blood from the CA with consequent collapse of the CA. They conclude that either condition could be the predisposing factor for the other. In our opinion, the stenosis first theory is more related to the formation of these PDAAs as shown by Yamamoto and his colleagues when they ligated the PDAA and the aneurysm continued to enlarge and the patient developed a new aneurysm in the peripancreatic arcade that did not regress except after normalisation of the pressure with aortohepatic bypass. 10
Our review showed that 40% of cases presented with rupture PDAAs but only 10% were unstable at the time of presentation. Despite being rare, treatment of PDAAs is advised as rupture is independent of size and the associated mortality is in excess of 50%. 11 Most cases who presented with rupture were stable on presentation which could be explained by rupture in the retroperitoneal space rather than intraperitoneal with small, confined space in peripancreatic area limits haematoma expansion. Our case presented with abdominal pain and the aneurysm was picked up incidentally on CT. 10,12,13
Treating these lesions should not be dependent on size of the aneurysm as many cases mentioned rupture even when the aneurysm was <1 cm. Surgery, endovascular, hybrid treatment and conservative treatment are all treatment options with endovascular favoured as it is less invasive and surgical accessibility can be difficult. Treatment recommendations are difficult to assess as most publications are case reports. 14 However, trans arterial embolisation (TAE) is getting popularity as first line treatment as it is less invasive and has a reduced mortality for these type of aneurysms with difficult surgical access. The main drawback and concern are preserving the foregut circulation in the presence of CA disease as TAE can compromise the hepatic blood flow with insufficient collateral circulation. 15
As shown in the review, trans arterial embolisation (TAE) with coils was the most common reported treatment (54%). Recommendations for revascularisation of associated coeliac artery disease cannot be clearly defined from the literature.
Bonardelli et al. 16 reported 5 open repair, 3 MAL release and 2 aorto-hepatic bypasses. They coiled 16 patients and 4 of them developed visceral ischaemia with three of them requiring further urgent open revascularisation. They had three mortalities in the endovascular group and one in the open group. Kimura et al. 17) described a case of embolisation for posterior branch PDAA that complicated with gall bladder necrosis and they had to release MAL 5th day post op but the patient died on 10th day as another aneurysm in the anterior branch of PDAA which ruptured. TAE alone may jeopardise the foregut circulation with ischaemia of the liver or gall bladder and revascularisation seems to be a safe alternative way to revascularise the foregut before TAE. We thought initially that TAE will be sufficient treatment, however, on performing the angiogram, the entire hepatic circulation seems to get its supply from PDA and performing TAE could jeopardise the hepatic circulation. Consequently, the case was aborted and discussion in our MDT revealed that staged treatment with revascularization first then embolization later could be the safer treatment in this young female.
Additionally, some authors have reported continuous growth of the aneurysm despite coiling as the pressure inside the aneurysm was presumably still high through the collateral circulation. Yamana et al. 33 used coils to occlude the PDAA first but the aneurysm continued to grow on follow-up with development of a new aneurysm in peripancreatic arterial arcade that regressed only after they did aortohepatic bypass to revascularise the celiac artery with resultant normalisation of the pressure inside the aneurysm. Several authors support normalisation of the pressure in the peripancreatic arterial arcade to avoid growth of these aneurysms and revascularisation of the foregut territory to avoid ischaemic complications.20,21
Revascularisation alone was adopted by some authors in their case reports as they argue that the aneurysm will regress when pressure is normalised and several authors reported regression of aneurysm by revascularisation18,19 or release of the Median arcuate ligament only (MAL). 20 However, we do not feel that release of MAL only is completely safe as it was illustrated by case presentation by Kimura et al. 17 when they coiled ruptured posterior PDAA but the patient developed Gall bladder necrosis 5th day postoperative and they have to revascularise the celiac artery by MAL release but the patient died 1 week later from ruptured anterior PDAA. This may denote that revascularisation alone with theory to normalise the pressure in the peripancreatic arterial arcade did not prevent rupture of PDAA and the aneurysm itself should be treated additionally to prevent progression and rupture.
Shibata and his colleagues used intraoperative haemodynamic pressure monitoring to guide revascularisation in their case report where the patient had anterior branch pancreaticoduodenal artery aneurysm and the posterior pancreaticoduodenal artery (PDAA) was small in calibre, and the patient was considered high risk for liver ischaemia. Surprisingly, no change in pressure on occlusion balloon test to the anterior branch PDA and posterior branch PDA enlarged with circulation maintained to liver. 21
Aorto-hepatic bypass as employed in our case was the most commonly used bypass in the literature. Takeuchi and his colleagues 22 reported bypass from the right renal to the common hepatic artery using great saphenous vein. Aryal and co-authors also used the common iliac artery as inflow. 23
A staged hybrid approach appears to be the safer option combining both TAE to occlude the aneurysm and revascularisation to normalise the pressure and avoid foregut ischaemic complications. Wattez et al. 11 used a hybrid approach differently; they performed an aorto-hepatic bypass as well as ultrasound-guided intraoperative coiling and aneurysm injection.
Endovascular treatment for both CA disease and PDAA could be an appealing useful option as used by some authors. However, the presence of associated MAL syndrome could jeopardise the stent and cause occlusion. 24–26
Conclusion
PDAAs are commonly associated with coeliac artery disease. The most common presentation is pain followed by rupture. The scarcity of literature about true peripancreatic artery aneurysms associated with CA occlusive disease makes it difficult to assess the natural history or the appropriate treatment. Staged hybrid treatment seems to be safer approach for such disease entity. Revascularisation of hepatic artery is better done with bypass in setting of in presence of median arcuate ligament compression and occluded celiac trunk.
What does this study/review add to the existing literature and how will it influence future clinical practice
We hereby present one rare and difficult case with literature review. The association between pancreatic-duodenal arterial aneurysm and celiac artery stenosis is not well explored in literature and the management is not well understood. We present our case report with our approach explained to avoid foregut ischaemia and we did literature review to highlight this rare presentation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Patient signed consent