
Abstract
Goal
Presentation of the first Russian computer program (www.carotidscore.ru) for risk stratification of postoperative complications of carotid endarterectomy (CEE).
Material and methods
The present study is based on the analysis of a multicenter Russian database that includes 25,812 patients after CEE operated on from 01/01/2010 to 04/01/2022. The following types of CEE were implemented: 6814 classical CEE with plastic reconstruction of the reconstruction zone with a patch; 18,998 eversion CEE.
Results
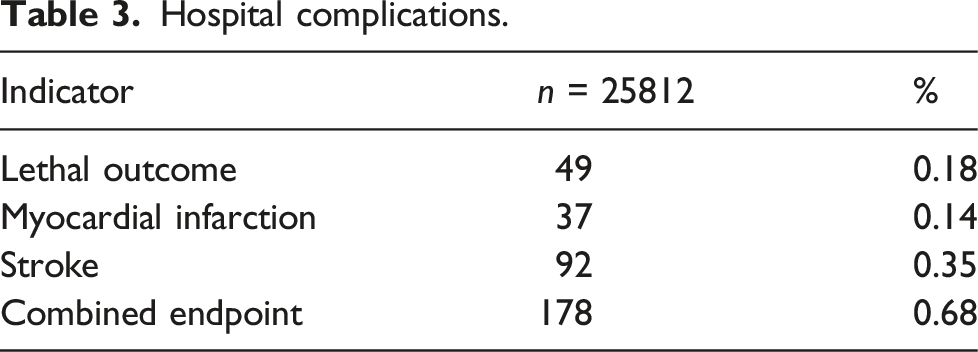
In the hospital postoperative period, 0.18% developed a lethal outcome, 0.14%—myocardial infarction, 0.35%—stroke. The combined endpoint was 0.68%. For each factor present in patients, a predictive coefficient was calculated. The prognostic coefficient was a numerical indicator reflecting the strength of the influence of each factor on the development of postoperative complications. Based on this formula, predictive coefficients were calculated for each factor present in patients in our study. The total contribution of these factors was reflected in “%” and denoted the risk of postoperative complications with a minimum value of 0% and a maximum of 100%. On the basis of the obtained calculations, a computer program CarotidSCORE was created. Its graphical interface is based on the QT framework (https://www.qt.io), which has established itself as one of the best solutions for desktop applications. It is possible not only to calculate the probability of developing a complication, but also to save all data about the patient in JSON format (for the patient’s personal card and his anamnesis). The CarotidSCORE program contains 47 patient parameters, including clinical-demographic, anamnestic and angiographic characteristics. It allows you to choose one of the four types of CEE, which will provide an accurate stratification of the risk of complications for each of them in person.
Conclusion
CarotidSCORE (www.carotidscore.ru) is able to determine the likelihood of postoperative complications in patients undergoing CEE.
Introduction
Carotid endarterectomy (CEE) is the most common open operation on the arteries both in Russia and worldwide.1-5 To date, specific standards for the implementation of this intervention are known. The current Russian recommendations presented the acceptable incidence of postoperative complications for those institutions that are engaged in the implementation of this intervention. 6 Thus, the value of the indicator “stroke + stroke mortality” should not exceed 3% in patients after transient ischemic attack (TIA) and 5% after ischemic stroke. 6 And the choice of treatment strategy should be based on the risk stratification of postoperative complications.6-8 Currently, there are two popular interactive calculators for determining the probability of developing adverse cardiovascular events after interventions on the cardiovascular system—Euro SCORE II and STS Score.9-13 However, due to their versatility, they do not meet the requirements of personalized medicine.14,15 Recently, there has been a growing trend of creating such computer programs for each type of revascularization separately.16-18 As a rule, they include an individual set of risk factors that are relevant specifically for one patient profile.16-18 However, specifically for the CEE, such interactive calculators have not yet been developed in the Russian Federation.
The purpose of this study was to demonstrate the first Russian computer program for risk stratification of postoperative CEE complications.
Materials and methods
The present study is based on the analysis of a multicenter Russian database that includes 25,812 patients after CEE operated on from 01/01/2010 to 04/01/2022. The following types of CEE were implemented: 6814 classical CEE with plastic reconstruction of the reconstruction zone with a patch; 18,998 eversion CEE. A 6/0 polypropylene suture was used to perform the vascular suture. To assess the compensatory capabilities of the brain, an invasive measurement of retrograde pressure in the internal carotid artery (ICA) was performed intraoperatively. When the latter was less than 60% of systemic arterial pressure, a temporary shunt was used. Before cross-clamping of the carotid arteries, 5000 units of unfractionated heparin were intravenously injected. In the postoperative period, the patient received 125 mg of acetylsalicylic acid once a day. Color duplex scanning was performed to discover the ICA stenosis. To visualize the ICA stenosis, color duplex scanning of the brachiocephalic arteries was performed. Then the patient was referred for computed tomography (CT) with angiography of the brachiocephalic arteries. Before hospitalization, all patients underwent echocardiography and examination by a cardiologist. If necessary, coronary angiography was performed. The SYNTAX Score interactive calculator (www.syntaxscore.com) was used to determine the severity of coronary lesion.
The choice of treatment tactics was carried out by a council, which included a cardiovascular surgeon, an endovascular surgeon, a neurosurgeon, a neurologist, a cardiologist, a resuscitator, an anesthesiologist.
Postoperative complications taken into account in the study were: lethal outcome, stroke, myocardial infarction (MI), combined endpoint (lethal outcome + stroke + MI).
In a study we performed earlier, we developed a formula capable of calculating the prognostic coefficient (R) for each factor present in a patient with multifocal atherosclerosis, where I is the number of patients with this factor; j is the number of patients with the development of postoperative complications with this factor; and Pij is the risk of postoperative complications (Figure 1). Formula for calculating the prognostic coefficient (R) for each factor present in a patient with multifocal atherosclerosis.
The prognostic coefficient was a numerical indicator reflecting the strength of the influence of each factor on the development of postoperative impediment. Based on this formula, predictive coefficients were calculated for each factor present in patients in our study. The total contribution of these factors was reflected in “%” and denoted the risk of postoperative complications with a minimum value of 0% and a maximum of 100%. On the basis of the obtained calculations, a computer program CarotidSCORE was created. Its graphical interface is based on the QT framework (https://www.qt.io), which has established itself as one of the best solutions for desktop applications. It is possible not only to calculate the probability of developing a complication (this is the likelihood of developing a combined endpoint), but also to save all patient data in JavaScript Object Notation format (for the patient’s personal card and his anamnesis).
Ethical standards
The study was performed in compliance with the ethical principles of scientific medical research involving humans. The work was performed in accordance with the standards of good clinical practice (Good Clinical Practice) and the principles of the Declaration of Helsinki, did not contradict the Federal Law of the Russian Federation of 21 November 2011 No. 323-FZ “On the basics of protecting the health of citizens in the Russian Federation,” the order of the Ministry Health of the Russian Federation dated 1 April 2016 N 200n “On approval of the rules of good clinical practice.”
Characteristics of the sample
Clinical and anamnestic characteristics of patient groups.
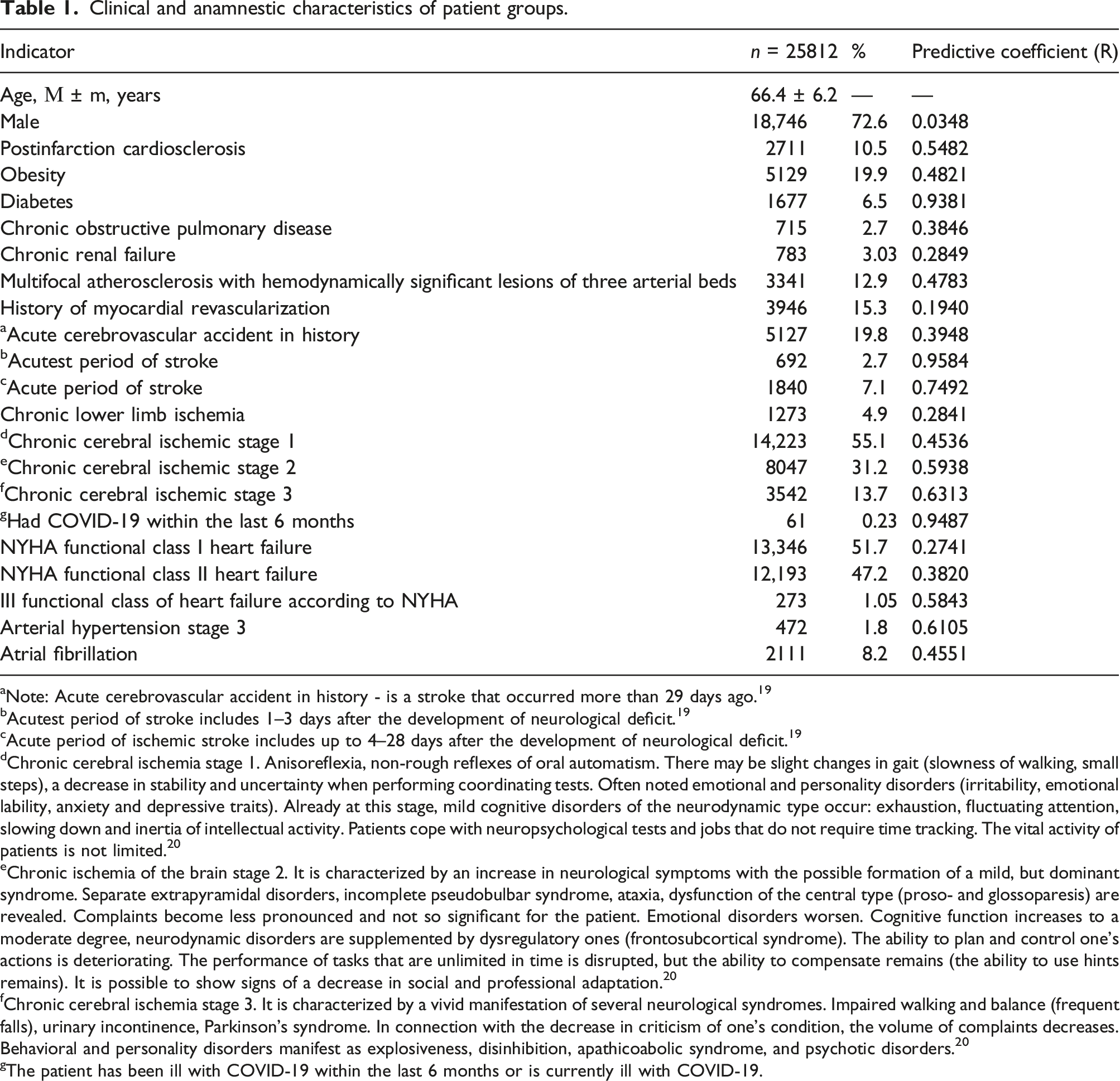
aNote: Acute cerebrovascular accident in history - is a stroke that occurred more than 29 days ago. 19
bAcutest period of stroke includes 1–3 days after the development of neurological deficit. 19
cAcute period of ischemic stroke includes up to 4–28 days after the development of neurological deficit. 19
dChronic cerebral ischemia stage 1. Anisoreflexia, non-rough reflexes of oral automatism. There may be slight changes in gait (slowness of walking, small steps), a decrease in stability and uncertainty when performing coordinating tests. Often noted emotional and personality disorders (irritability, emotional lability, anxiety and depressive traits). Already at this stage, mild cognitive disorders of the neurodynamic type occur: exhaustion, fluctuating attention, slowing down and inertia of intellectual activity. Patients cope with neuropsychological tests and jobs that do not require time tracking. The vital activity of patients is not limited. 20
eChronic ischemia of the brain stage 2. It is characterized by an increase in neurological symptoms with the possible formation of a mild, but dominant syndrome. Separate extrapyramidal disorders, incomplete pseudobulbar syndrome, ataxia, dysfunction of the central type (proso- and glossoparesis) are revealed. Complaints become less pronounced and not so significant for the patient. Emotional disorders worsen. Cognitive function increases to a moderate degree, neurodynamic disorders are supplemented by dysregulatory ones (frontosubcortical syndrome). The ability to plan and control one’s actions is deteriorating. The performance of tasks that are unlimited in time is disrupted, but the ability to compensate remains (the ability to use hints remains). It is possible to show signs of a decrease in social and professional adaptation. 20
fChronic cerebral ischemia stage 3. It is characterized by a vivid manifestation of several neurological syndromes. Impaired walking and balance (frequent falls), urinary incontinence, Parkinson’s syndrome. In connection with the decrease in criticism of one’s condition, the volume of complaints decreases. Behavioral and personality disorders manifest as explosiveness, disinhibition, apathicoabolic syndrome, and psychotic disorders. 20
gThe patient has been ill with COVID-19 within the last 6 months or is currently ill with COVID-19.
Results
Angiographic and perioperative characteristics.
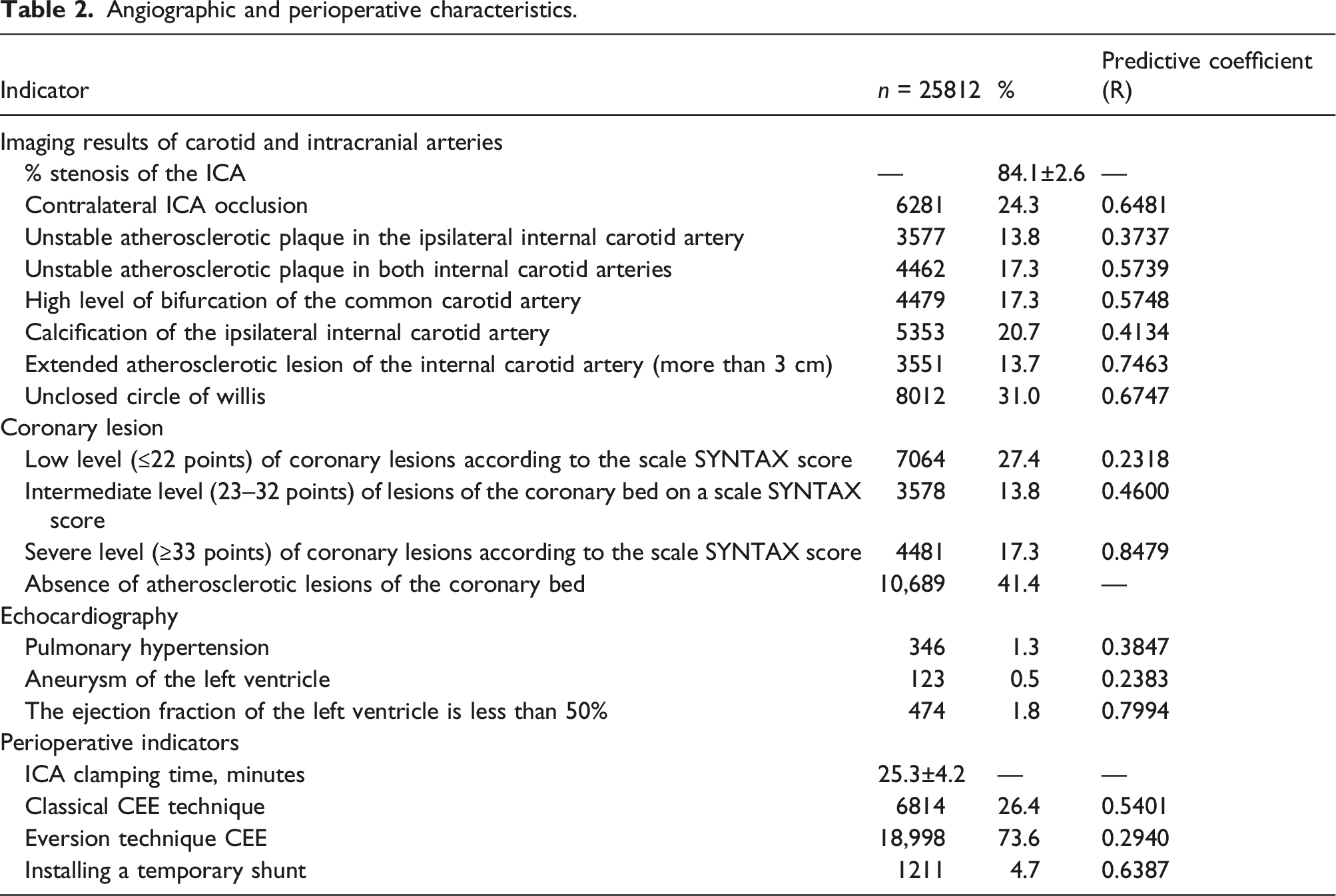
The least common was the classical CEE with the plastic of the reconstruction area with a patch. During the implementation of eversion CEE, in 857 cases, glomus-sparing surgical techniques, popular in the Russian Federation, were also performed, including the technique according to A.N. Kazantsev (n = 642) 4 and the «Chik–chirik» technique (n = 215) 21 (Table 2).
A temporary shunt was installed according to the indications in accordance with the current Russian recommendations (during clamping of the common carotid artery and external carotid artery, with a decrease in retrograde pressure in the internal carotid artery below 60% of systemic arterial pressure). 6
3596 patients required myocardial revascularization as the next step. In 893 patients, CEE was performed as part of a combined CEE + coronary bypass operation, 2676 as part of a hybrid operation of percutaneous coronary intervention + CEE.
Hospital complications.
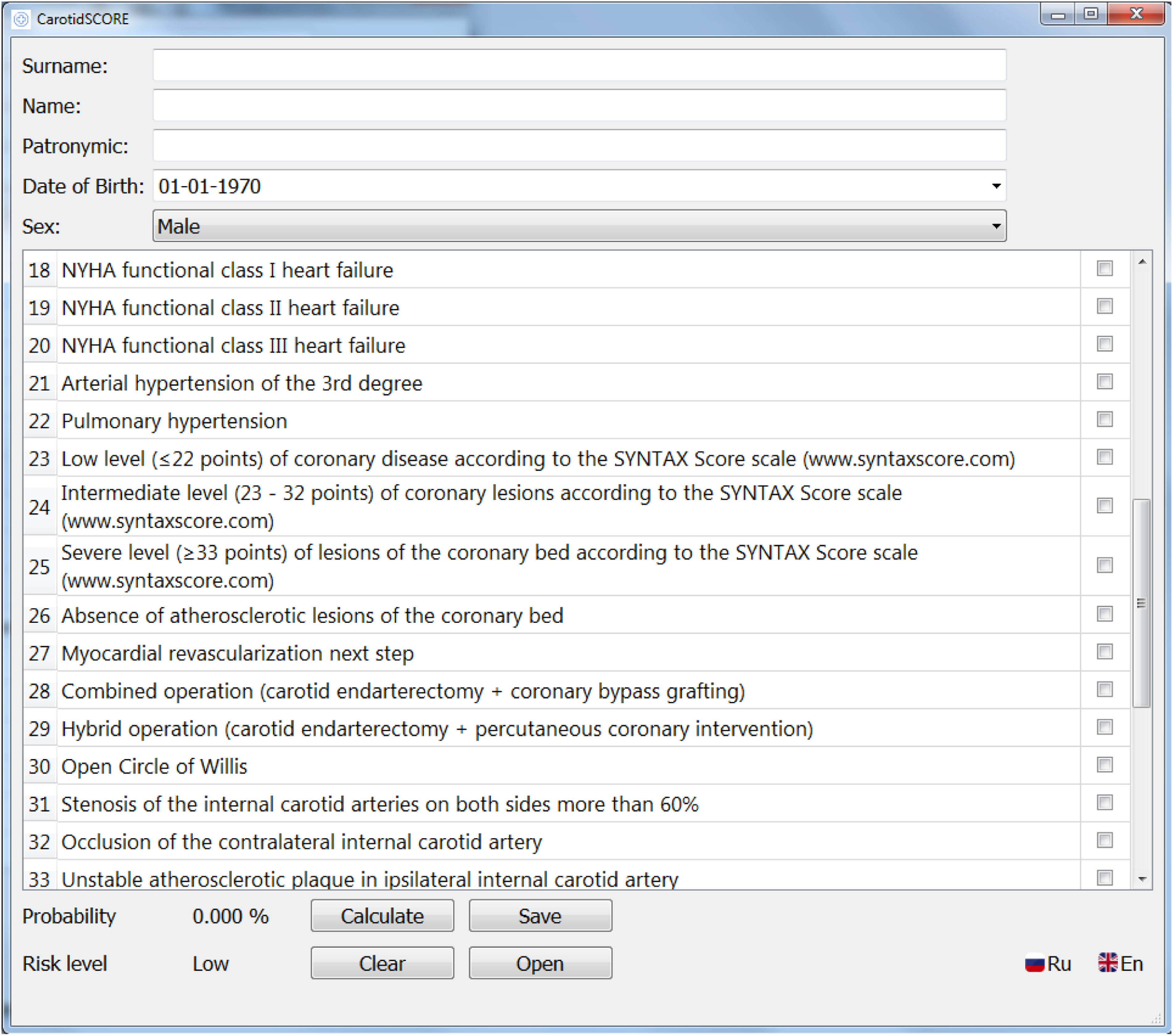
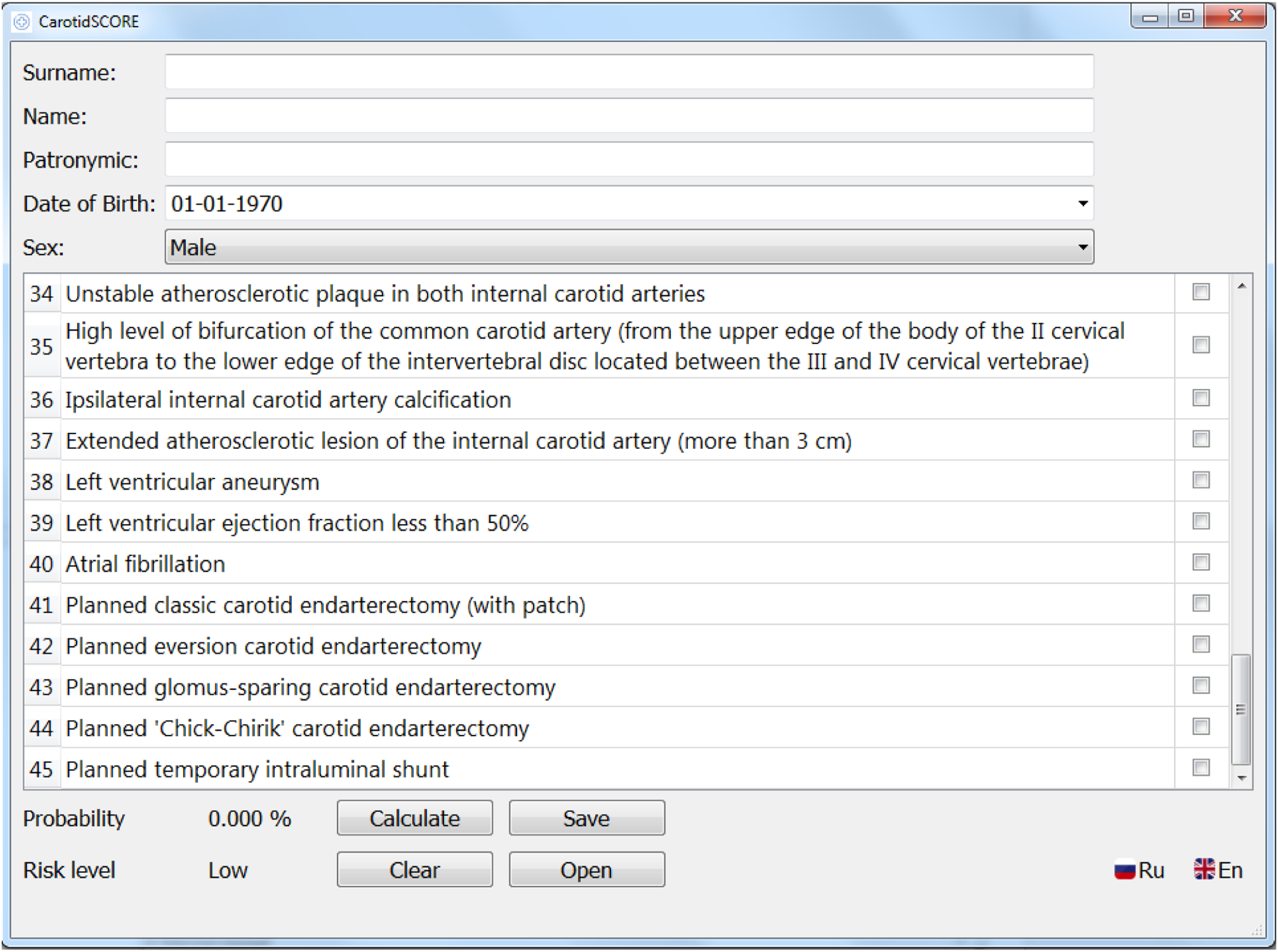
Based on the calculation of prognostic coefficients using a complex mathematical analysis and the formula presented in Figure 1(a) prognostic model and a program for risk stratification of postoperative complications of CEE – CarotidSCORE (www.carotidscore.ru) (Figure 2, Figure 3 and Figure 4) were built. The gradation of the risk of developing complications has three levels: low risk (0–33%), medium risk (34–67%), high risk (68–100%). The first page of the interface of the CarotidSCORE (www.carotidscore.ru) program. The second page of the interface of the CarotidSCORE (www.carotidscore.ru) program. Third page of the CarotidSCORE (www.carotidscore.ru) interface.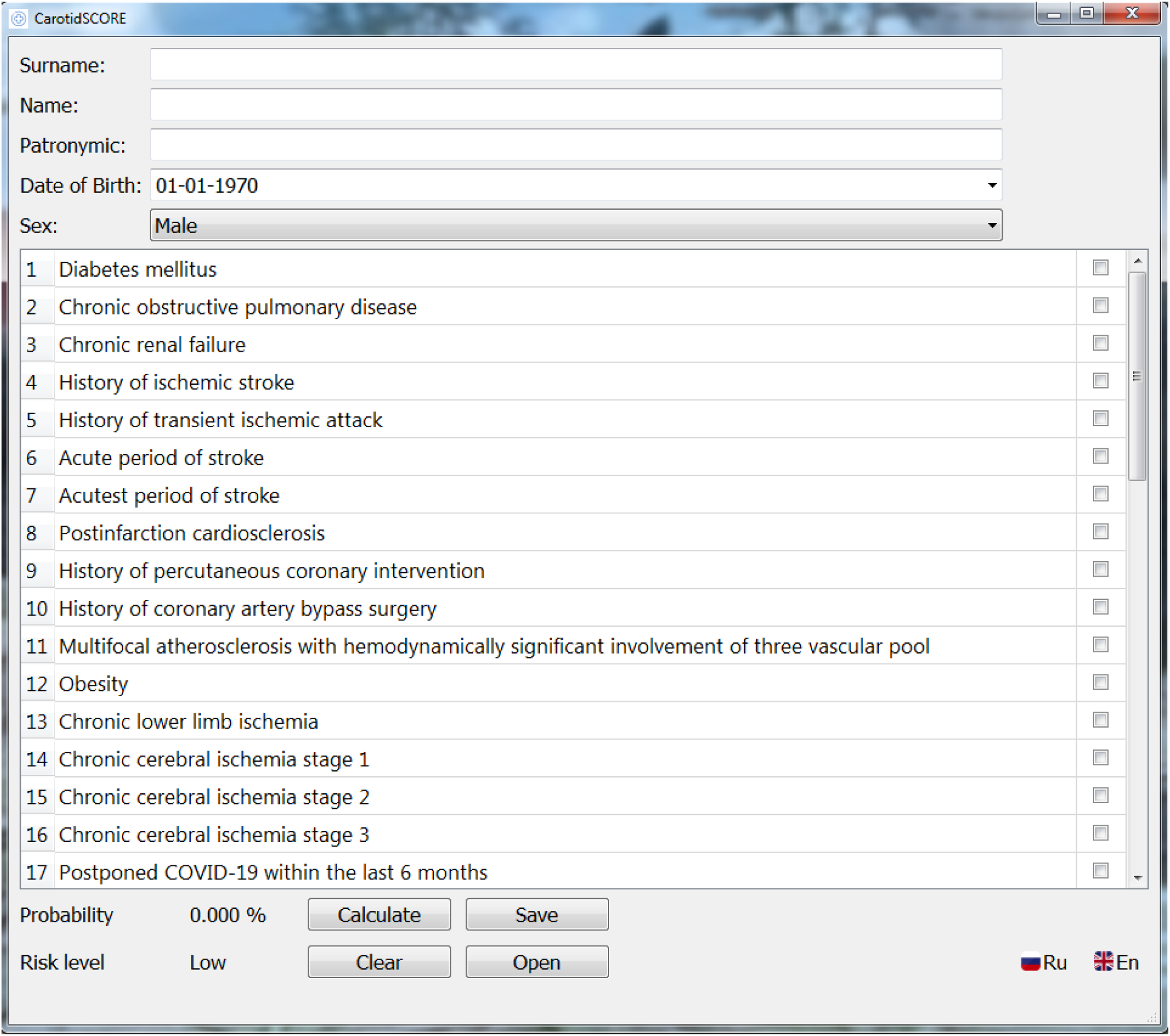
Discussion
Accurate surgical risk stratification is critical in cardiac surgery.15,16 It allows you to assess the possible risks of intervention, and make an informed choice of treatment strategy.15,16
In order to determine the tactics of myocardial revascularization, the following scales have been recognized in clinical practice: “TIMI” (Thrombolysis in Myocardial Infarction), “Global Risk Classification,” “GRACE” scale (Global Registry of Acute Coronary Events), “Euro Score,” “CADILLAC” (the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications), “ACEF score” (Value of Age, Creatinine, and Ejection Fraction).22-26 The Euro SCORE scale and its logistic variant are the most widespread in Russia and Europe.9-11,15,16 The Euro SCORE scale, based on an additive system obtained using a logistic regression model, was developed on data collected in 1995 and registered in 1999 to predict the risk of surgical complications in the 30-day postoperative period.9–11 However, the predictive power of any risk stratification algorithms may change over time as a result of changes in the epidemiology of cardiovascular diseases, modernization of surgical treatment methods, instrumentation, indications for operations.15,16 It has been shown through a high-risk group assessment that Euro SCORE is not able to provide an accurate assessment of the possible development of complications.15,16,27,28 To overcome these limitations, an updated version of the scale was created—Euro SCORE II, modeled in modern conditions, in a group of 22,381 patients in 150 clinics from 43 countries.9-13 However, a number of researchers agree that Euro SCORE II underestimates the mortality rate and risks of complications in the high-risk group of patients, and also does not take into account the anatomical component of atherosclerotic lesions of the coronary arteries.15,16,27,28 The Euro SCORE scale took into account the following patient risk factors: age, height, sex, body weight, the presence of concomitant pathology (chronic obstructive pulmonary disease, MPA), myocardial contractility, the urgency of the operation, the presence of endocarditis, previous cardiac surgery, pulmonary artery pressure, features operations (time of cardiopulmonary bypass, time of aortic cross-clamping, time of circulatory arrest), critical condition of the patient before surgery, renal dysfunction, decreased plasma protein level, symptoms of the disease (functional class of angina pectoris and heart failure).
The Euro SCORE II scale has a number of differences from the first version: age limit (minimum 18 years, maximum 90), diabetes mellitus (insulin-dependent), angina functional class IV (CCS), heart failure functional class (NYHA), pulmonary hypertension ranking (31–50 mmHg and >50 mmHg). The type of operation was taken into account (myocardial revascularization, surgery on the valvular structures of the heart, combined interventions), and there was also a division into four types of surgical intervention: planned, urgent, emergency, resuscitation; such a risk factor as postinfarction ventricular septal defect has been excluded.9-13
In 2008, the Society of Thoracic Surgeons of the United States created another risk stratification scale—STS SCORE, which was based on a multicenter database of more than 100,000 patients. Using 67 demographic and operational parameters, it demonstrates the likelihood of complications and death, but its bulkiness creates inconvenience in use.29-33 In general, according to the literature, the STS SCORE model has a high degree of evidence and has found its acceptance in risk stratification in a more severe cohort of patients.29-33 Like Euro SCORE II, STS SCORE is an easy-to-use online calculator (www.sts.org) for predicting postoperative mortality in patients undergoing open heart surgery, but requires more detailed patient data. As with other models, mortality is the main endpoint in the STS SCORE; however, this calculator also determines the likelihood of other adverse events, such as 30-day mortality, neurological deficit, wound infection, prolonged mechanical ventilation, renal failure, reoperation, while in comparison with Euro SCORE II, STS SCORE underestimates the perioperative risk of complications.29-33 With the publication of the results multicenter randomized study “SYNTAX” (www.syntaxscore.com), which included 1800 patients and based on a comparative assessment of PCI and CABG in patients with multiple occlusive-stenotic changes in the coronary bed, it became possible to assess the severity of the lesion in the coronary basin.34-38 According to the severity of the lesion, the following gradation is distinguished on the basis of this calculator: low level (≤22 points), intermediate (23–32 points) and severe (≥33 points). 39 An important shortcoming of this study was the lack of inclusion of clinical characteristics of patients, which was eliminated in the modified SYNTAX II calculator.32-36 The results of this analysis assessed the 4-year outcomes of the previous study. Among the predictors of adverse events, the following were identified: the severity of coronary artery lesions on the SYNTAX scale, stenosis of the unprotected trunk of the left coronary artery, age, female sex, left ventricular ejection fraction, creatinine clearance, atherosclerotic lesions of the peripheral arteries, chronic obstructive pulmonary disease. Based on this analysis, an improved scale “SYNTAX II” was created, which makes it possible to reasonably determine the method of coronary revascularization for each patient individually.34-38
Thus, there are a number of prognostic scales that allow risk stratification in patients with a cardiovascular profile, the main ones being Euro SCORE II, STS SCORE and SYNTAX. However, each of them has a number of limitations and disadvantages: Euro SCORE II—versatility in use for all cardiosurgical patients, lack of indicators of coronary disease; STS SCORE—bulkiness, lack of indicators of coronary lesion; SYNTAX II - limited number of records of clinical indicators. In addition, these scales are not intended for risk stratification in a cohort of patients with carotid atherosclerosis and the choice of the optimal strategy for cerebral revascularization. In this regard, there is a need to develop new algorithms and models.
One of the advantages of CarotidSCORE, which distinguishes it from other well-known risk stratification calculators, is that it takes into account the patient’s history of COVID-19. When creating CarotidSCORE, data from 61 patients were taken into account, of which 43 patients underwent emergency carotid endarterectomy against the background of COVID-19 and thrombosis of the internal carotid artery. A study on these results was published by us earlier.40,41 We found that coagulopathy and internal carotid endothelitis associated with COVID-19 increases the risk of recurrent thrombosis. Therefore, emergency carotid endarterectomy in patients with COVID-19 is accompanied by an increased risk of complications. However, in our previously published study, no cases of re-thrombosis of the internal carotid artery were found, which is associated with the continuous administration of unfractionated heparin intravenously at a rate of 1500 units per hour for several days after surgery.40,41
Against this background, it should be noted that in the Russian Federation there are several interactive calculators for risk stratification of postoperative complications for patients with atherosclerotic lesions of different arterial beds. Under the leadership of the Kazantsev A.N. in 2017, a program and a method for determining treatment tactics for patients who are indicated for carotid endarterectomy and myocardial revascularization were developed.42,43 Based on the results of various strategies of staged, combined and hybrid revascularization, which were used in the city of Kemerovo, Russia, in the period from 2011 to 2015. A complex analysis was carried out and a mathematical model was created that can personalize, taking into account the individual factors of the patient, determine the level of risk of postoperative complications in the implementation of a particular treatment strategy. 44
In 2017, under the guidance of MD. Vinogradova R.A. developed a method “Predicting the risk of postoperative complications of stenosis of the internal carotid arteries”. 45 However, this development did not have an interactive implementation and therefore was not widely used. Later, in 2018, under the guidance of MD. Vinogradova R.A. a computer program was developed “Predicting complications in carotid endarterectomy and carotid angioplasty with stenting”. 46 But this interactive calculator also did not become popular due to several reasons: (1). Small sample size of patients; (2). Limited number of risk factors taken into account; (3). No available online version.
The CarotidSCORE (www.carotidscore.ru) computer program has no analogues today. Several tens of thousands of CEEs are performed annually in the Russian Federation. Thus, the need for risk stratification of adverse cardiovascular events for this cohort of patients is particularly acute. CarotidSCORE (www.carotidscore.ru) is able to determine the likelihood of postoperative complications in patients undergoing CEE. But it must be remembered that the level of risk that it offers cannot be an indication or contraindication for revascularization. The latter are widely known to all and are set out in the current recommendations. Thus, at a high level of risk of postoperative complications of CEE, the council that chooses the treatment tactics for the patient may consider interventional or drug correction.
Currently, most interactive calculators are built on the basis of complex statistical analyzes with the search for risk factors that, according to the calculations, significantly affect the development of complications. At the same time, many predictors that are important for clinicians can be regarded as insignificant. In this situation, insignificant factors are not taken into account when creating such calculators. As a result, such programs meet all the requirements of complex statistical analysis, but do not meet the requirements of clinicians. As a result, they are not popular in medical practice. The CartoidSCORE calculator was built on the principle of calculating prognostic coefficients for all factors present in patients. The more often the factor occurred in patients with postoperative complications, the higher its prognostic coefficient. Thus, a wide personalized set of factors that the CartoidSCORE calculator offers to take into account is new, and the method of creating CartoidSCORE is not standard, which is of interest. The weakness of the CartoidSCORE calculator is that it is currently in prospective testing. In this connection, a search is underway for representatives of the world medical community to test the CartoidSCORE calculator on the basis of various institutions.
Conclusion
CarotidSCORE (www.carotidscore.ru) can be used to stratify the risk of postoperative adverse cardiovascular events in patients undergoing. Carotid endarterectomy o conflict of interest
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.