
Abstract
Objective
Presentations of a spontaneous ilio-iliac arteriovenous fistula are considered a rare occurrence and warrant urgent intervention. They are usually a result following trauma, previous surgery or uncommonly from a ruptured aneurysm.
Method
We describe a case of a patient presenting with general malaise who examined to have a pulsatile abdominal mass with an associated bruit. He was found to have an ilio-iliac arteriovenous fistula secondary to a ruptured iliac aneurysm that was treated successfully with open surgical repair.
Result
The patient was brought forward for open surgical repair due to haemodynamic instability as well as likely predicted difficulties with endovascular repair. Intra-operatively, his sigmoid colon was adherent to the aneurysm prompting the need for a Hartmann’s procedure to allow for better visualisation of the aneurysm. A combination of external digital compression and Prolene suture was used to close the arteriovenous fistula.
Conclusion
Open surgical repair of an ilio-iliac arteriovenous fistula secondary to a ruptured iliac aneurysm appears to be safe and feasible approach. The advancement of medical technology does open up the possibility of an endovascular approach; however, in a small subset of patients, open repair would appear to be better.
Case
A 76-year-old man presented to the Emergency Department with 3 days of feeling unwell with nausea and vomiting. This was associated with left lower abdominal pain. This was localised and not radiating to the back. On examination, he was peripherally shutdown, tachycardic, stable blood pressure (118/60 mmHg) and tachypnoeic with an oxygen saturation of 94% on room air. Jugular venous pressure was not elevated. His abdomen was soft but tender to palpate over the left lower quadrant. There was a palpable, pulsatile mass in the left lower quadrant. The abdomen was dull to percussion throughout. There was a large bruit on auscultation over the lower abdomen. He had bilateral palpable femoral and pedal pulses with pitting oedema.
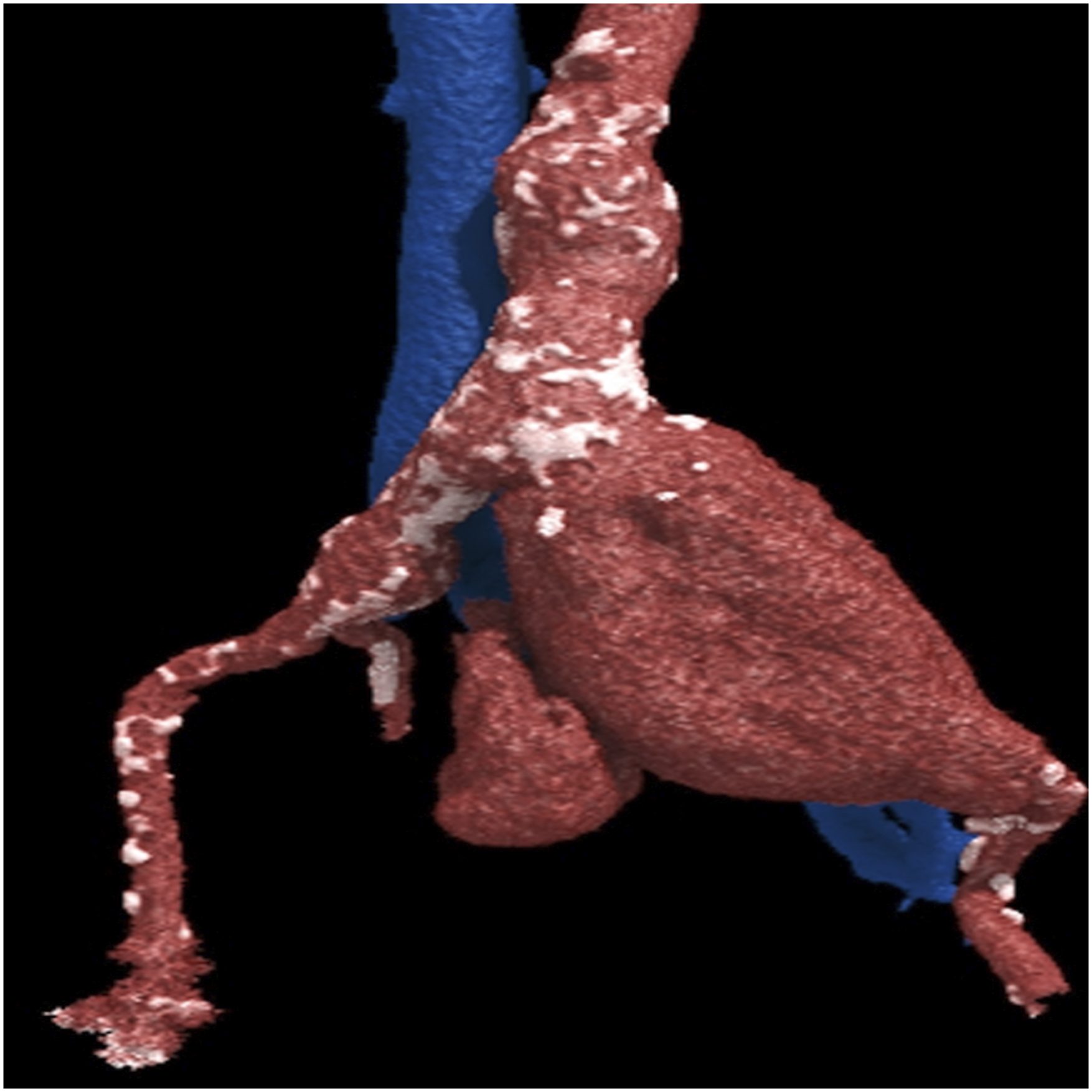
The initial laboratory test showed a haemoglobin of 128 g/L, lactate 8.3 mmol/L and acute renal injury (creatinine 287 μ mol/L and urea 21.2 mmol/L). Ultrasound showed a large left common iliac artery aneurysm (CIAA). An urgent computed tomography angiography (CTA) scan showed a ruptured left CIAA, measuring 100 mm in diameter, with surrounding stranding. There was a fistula between the left CIAA and the left common iliac vein (CIV) with arterialisation of the inferior vena cava (IVC). This is shown in Figure 1 as well as a 3D reconstruction on Figure 2. Axial image of the ruptured left CIA aneurysm (A) with a fistula (shown by red arrow) to the left CIV (V) at 7 o’clock with IVC (I) arterialisation. 3D reconstruction coronal CT angiography image of the left CIA aneurysm.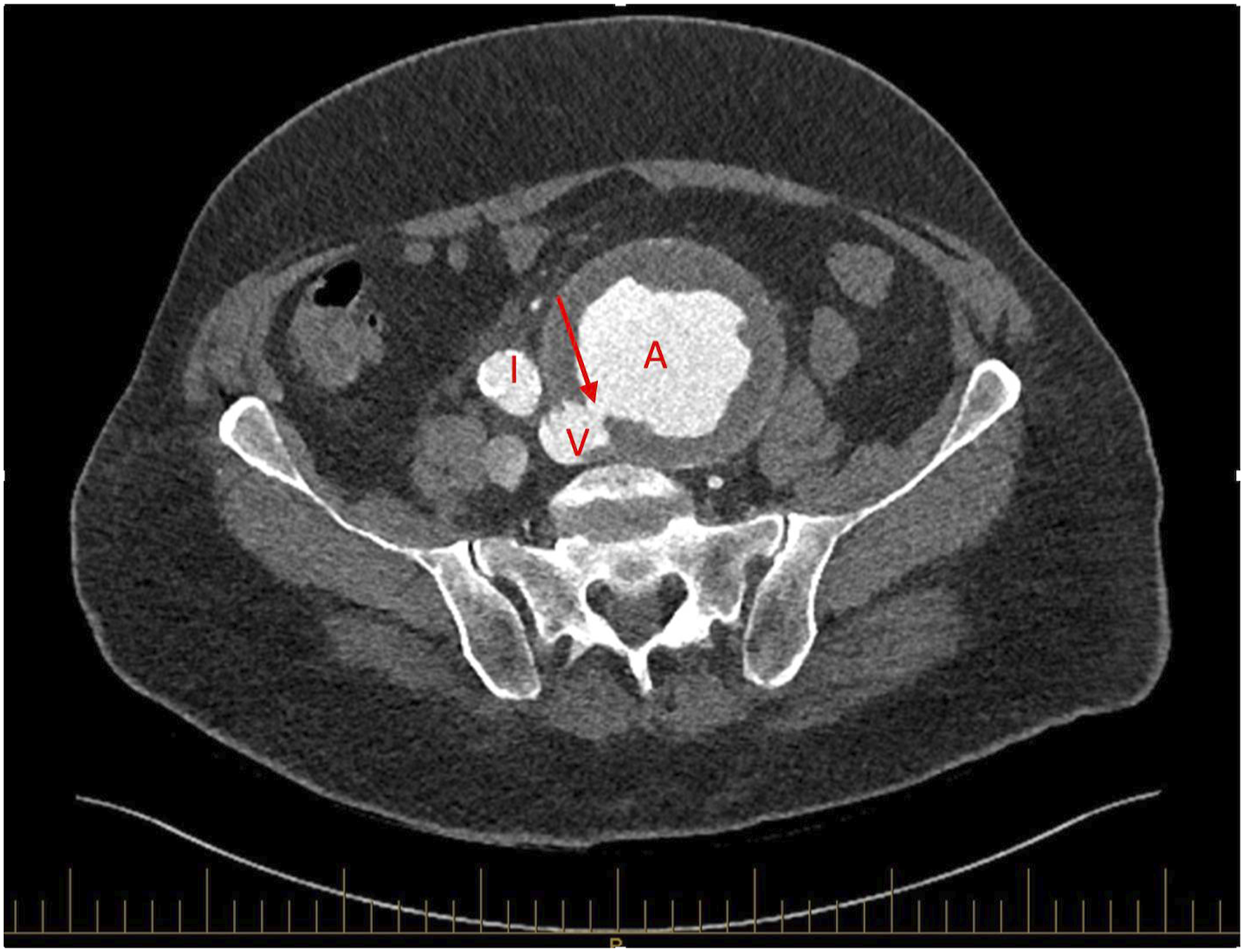
An emergency midline laparotomy was performed. It was anticipated that the sigmoid colon would be lying across and adherent to the left CIAA. This is shown in Figure 3. Intraoperative image showing the left common iliac artery aneurysm.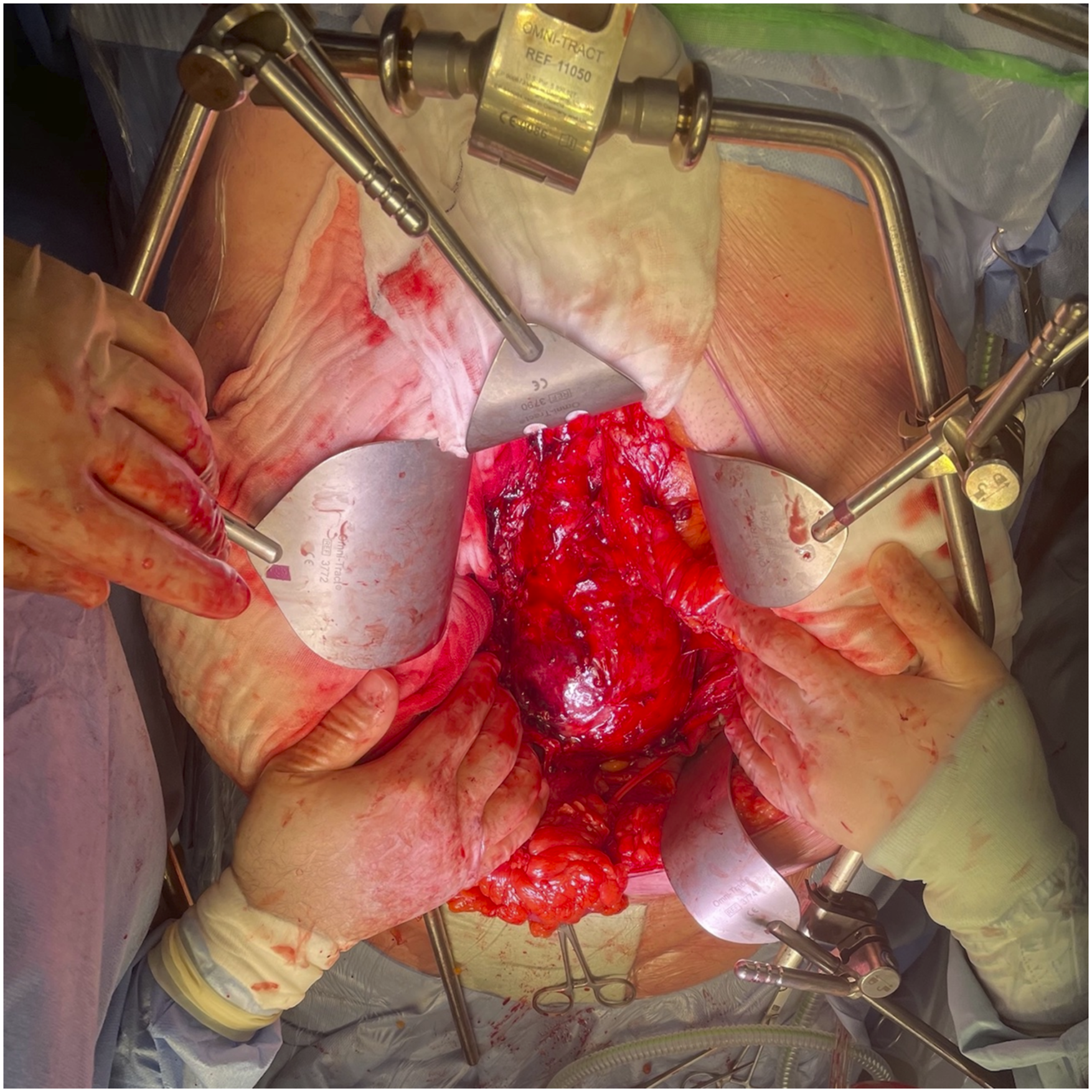
Therefore, we planned to achieve vascular dissection as well as proximal and distal control. As better visualisation of the intra-aneurysmal sac is imperative for control of bleeding and repair, we decided to proceed with a sigmoid colectomy and a Hartmann’s procedure. This was performed by the General Surgery team. Vascular clamps were placed over the infrarenal abdominal aorta for proximal control and over the right common iliac artery (CIA) and left external iliac artery (EIA) for distal control. The aneurysm sac was opened. There was no back bleeding from the left internal iliac artery. Large amounts of thrombus was evacuated from the aneurysm sac. The orifice of the fistula was visible and venous bleeding control was achieved by external digital compression on the left CIV. The fistula was directly closed from within the aneurysm using 4-0 Prolene suture (Ethicon Inc, New Jersey, United States of America). Aneurysm repair was completed using a silver-impregnated Dacron bifurcated graft (Maquet, Rastatt, Germany) with the proximal anastomosis over the infrarenal aorta and the distal anastomosis performed over the right CIA and left EIA. The patient was stable at the end of the procedure with an unsupported blood pressure, mean arterial pressure (MAP) >70 mmHg and a haemoglobin of 122. He was given a total of three doses of prophylactic antibiotics post procedure. He had an uncomplicated recovery and was discharged home day 9 post procedure. An ultrasound scan performed prior to discharge demonstrated normal flow suggesting successful fistula closure. He was followed-up in clinic 6 weeks post discharge without any reported complications. He was seen by the General Surgery team 8 weeks post-surgery for consideration of reversal of colostomy but the patient declined further surgical intervention.
Discussion
The incidence of ilio-iliac arteriovenous fistula (AVF) is quoted to be as low as 1% in the medical literature.1,2 Spontaneous arteriovenous fistula formation secondary to a ruptured common iliac aneurysm are a rare occurrence with the first ever being described in the literature in the 1970s. 3 A triad of presenting symptoms are usually described in these patients – high output cardiac failure, pulsatile abdominal mass with a palpable thrill or bruit and peripheral oedema or limb ischaemia.1,3,4 However, these were only found to be true in 50–80% of patients. 4 Timely diagnosis is crucial as the risk of an untreated arteriovenous fistula causing haemodynamic compromise could lead to poor prognosis.
One of the technical difficulties in performing open repair is obtaining control of venous bleeding from the fistula. Multiple methods have been described in previous studies either with the use of digital compression, sponge stick or balloon catheters with good effect.1,5
Management options in the past were mainly via open approach. However, the advancement of medical technology has opened up the possibility of endovascular repair. Endovascular repair allows for quicker recovery, shorter inpatient stay and lower risk of bowel, respiratory and renal complications as well as mortality. 4 There have been reports of endovascular aortic repair with embolization or the use of covered stents and arterial coils with good results.2,4 The main challenge with an endovascular approach would be the closure of the fistula since it would be the main source of type 2 endoleak with no specific venous covered stents currently available in the market. It also carries a high risk of fistula recurrence, aneurysm sac expansion and stent migration. 4 Ultimately, this does not guarantee complete exclusion of the aneurysm and fistula which could be achieved with open surgical repair. Despite the risks involved, it should be noted that open repair would perhaps be a better option in a specific subset of patients.
Conclusion
Open surgical approach can be challenging but is a feasible approach in acute ilio-iliac arteriovenous fistula secondary to a ruptured aneurysm. Endovascular techniques has its own challenges and drawbacks but nonetheless could be considered in certain clinical scenarios.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical consideration
Written consent has been obtained from the patient for use of images and publication of case study.