
Abstract
Objectives
According to guidelines, the autogenous saphenous vein (ASV) is the preferred conduit for femoropopliteal bypass surgery in all patients with peripheral artery disease. However, in contrast to patients with critical limb ischemia (CLI), patients with intermittent claudication (IC) only, tend to have milder disease, and thus a prosthetic graft may be as good as a vein conduit. The objective of this study was to compare patency rates of the ASV and a prosthetic graft in femoropopliteal bypass surgery in patients with IC.
Methods
A systematic literature search was performed in the PubMed, Embase, and Cochrane databases to identify randomized controlled trials comparing prosthetic graft versus ASV in patients with IC. Articles with a mixed IC and CLI study population were included if more than 50% of the study cohort was treated for IC. Primary analysis was performed on IC patients only. Secondary analysis was performed on the mixed group. The primary endpoint was short- and long-term patency and secondary endpoints were complications, limb salvage, and mortality.
Results
In total, six studies with 524 patients were included. Only two studies reported solely on patients with IC. All these patients underwent above-the-knee bypasses and average patency rates at one and 5 years were 88% and 76% vs 81% and 68% in the ASV and the PTFE groups, respectively. One and five-year patency was not statistically different between the groups (OR 5.21; 95% CI 0.60–45.36 and OR 2.10; 95% CI 0.88–5.01). In a mixed population of patients with IC and CLI (84% IC patients), 1 year patency was comparable (OR 1.40; 95% CI 0.87–2.25). However, after a follow-up of over 3 years, this mixed group had significantly higher patency rates in favour of the ASV (OR 2.06; 95 % CI 1.30–3.26). Complication and amputation rates were comparable in both groups.
Conclusions
Limited data are available for patients receiving above-the-knee femoropopliteal bypass for intermittent claudication. The ASV remains the conduit of choice for femoropopliteal bypass surgery. However, the prosthetic conduit seems a feasible alternative for patients with intermittent claudication in whom the ASV is not present or unsuitable.
Keywords
Introduction
Most patients with intermittent claudication (IC) due to superficial femoral artery disease can be treated conservatively with supervised exercise training, control of risk factors, and medical therapy.1–3 However, severe IC can result in functional impairment, which consequently can lead to a decrease in quality of life and even reduced survival. 4 If conservative management does not lead to satisfactory results, and a patient is experiencing IC that is significantly inhibiting their daily activity, invasive therapy might be considered.
A minimum threshold of 50% expected clinical improvement for at least 2 years after treatment has been suggested as a criterion to consider invasive treatment. 5 Invasive treatment options include endovascular interventions and femoropopliteal bypass surgery. Although endovascular interventions have been proven to be less invasive, have a low complication rate and a shorter hospital stay, patient-specific or lesion-specific characteristics can give direction to a surgical approach.1,6–8 For example, patients with lesions of more than 25 cm in length with or without extensive calcifications, patients with small caliber arteries and patients that had prior failed endovascular treatment, might benefit more from bypass surgery compared with endovascular therapy. 5 Therefore, a patient with these characteristics who is fit for surgery, will ideally be treated by bypass surgery.1,5
Current guidelines state that this is especially true for patients with a good quality autogenous saphenous vein (ASV).1,5 However, the question arises whether this advice should apply to both patients with IC and patients with critical limb ischemia (CLI), and whether this should apply for both above and below-the-knee anastomoses. Patients with IC usually have better operative and clinical outcomes, as they tend to be in a better clinical condition, have better distal outflow, and a less severe level of peripheral artery disease. Also, IC has a relatively benign and stable prognosis since only a small number of patients will progress to developing CLI.3,9,10 The use of a prosthetic conduit in femoropopliteal bypass surgery will result in a shorter procedure time and a less extensive intervention, which could subsequently lead to a lower complication rate and a faster recovery. 11 Therefore, the aim of this study was to compare the short- and long-term patency outcomes of the use of ASV versus a prosthetic graft as a conduit in femoro-popliteal bypass surgery in patients with IC. A systematic review and meta-analysis were performed to answer this question.
Methods
Search strategy
A systematic search of the literature was performed in the PubMed, EMBASE, and Cochrane databases to identify all studies up to 1 February 2022. The search strategy is described in the appendix. In addition, all the references of the included studies were reviewed to identify additional publications. This report is written in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement. 12
Study selection
Two reviewers independently selected the studies (R.J.V and T.M.F). In case of disagreement, a third reviewer was consulted (A.C.V). Only original articles were included. Articles were selected for inclusion if they compared outcomes of the ASV with any prosthetic graft in patients with IC due to superficial femoral artery disease. Only randomized controlled trials (RCT) and comparative controlled studies were included. Studies reporting solely on patients with CLI were excluded. If a mixed population of both patients with CLI and IC were studied, articles were initially included to avoid loss of information. However, if less than 50% of the total number of patients were treated for IC, studies were considered ineligible for the purposes of this study and therefore excluded. All potentially relevant studies, including the abstracts of those studies which did not provide sufficient information for inclusion or exclusion, were obtained as full articles. Both reviewers independently assessed eligible studies for inclusion based on the full article. Disagreement was resolved by discussion until consensus was reached.
Outcome measures
Outcome measures that had to be reported were primary, primary assisted, and/or secondary patency rates. In accordance with the SVS–ISCVS guidelines, primary patency was defined as uninterrupted patency without any manipulation of the graft.13,14 Primary assisted patency was defined as uninterrupted graft patency, but maintained by prophylactic intervention such as angioplasty, patch angioplasty, or small graft interpositions. Secondary patency was defined as restored patency after occlusion with or without revision of the graft. A “redo” or secondary reconstruction, does not contribute to secondary patency unless most of the original graft and at least one anastomosis is retained in continuity. For the scope of this study, we combined all post-intervention procedures that were used to keep the original graft patent. This will be referred to as patency in this manuscript. Secondary outcome measures were amputation, complication, and mortality rates.
Quality assessment and data extraction
Quality assessment was performed using the Cochrane Collaboration’s tool for the assessment of the risk of bias in randomized controlled trials. 15 Studies in each individual domain were classified as low-, unclear-, or at high risk of bias. Any disagreement between the two reviewers was resolved by discussion. A summary of the methodological quality of the included studies will be presented. The primary outcome measures that were extracted from each study were primary-, primary assisted-, and secondary patency rates. Secondary outcome measures were postoperative outcomes and amputation, complication and mortality rates, and functional or patient-reported outcome measures (PROMs).
Strategy for data extraction and synthesis
Extracted data were analyzed using RevMan 5.3 software provided by the Cochrane Collaboration. The I2 statistics was used to analyze the heterogeneity between studies. If studies were sufficiently homogeneous and reported on the same outcome measure, we pooled the data using a fixed-effects model to estimate the odds ratios (ORs) of patency. Statistical significance was set at a p < .05.
Analyses
Primary analysis was performed in a study group of patients treated solely for IC. In the secondary analysis, the total cohort was analyzed, by including the studies that treated at least 50% of the patients for IC as well as the studies that solely treated patients for IC.
Study protocol
The study protocol is registered on PROSPERO (CRD42017080732), available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42017080732
Results
Search results
In total, 527 studies were identified (Figure 1). After screening titles and abstracts, 19 articles remained for full-text assessment. Additionally, ten articles were excluded. Reasons for exclusion were using previously published data that were already included in our analysis or wrong study design. Three studies were excluded after extracting the patient data, as it became apparent that the proportion of patients with IC did not exceed the minimum of 50% of the total cohort. Study selection in flowchart.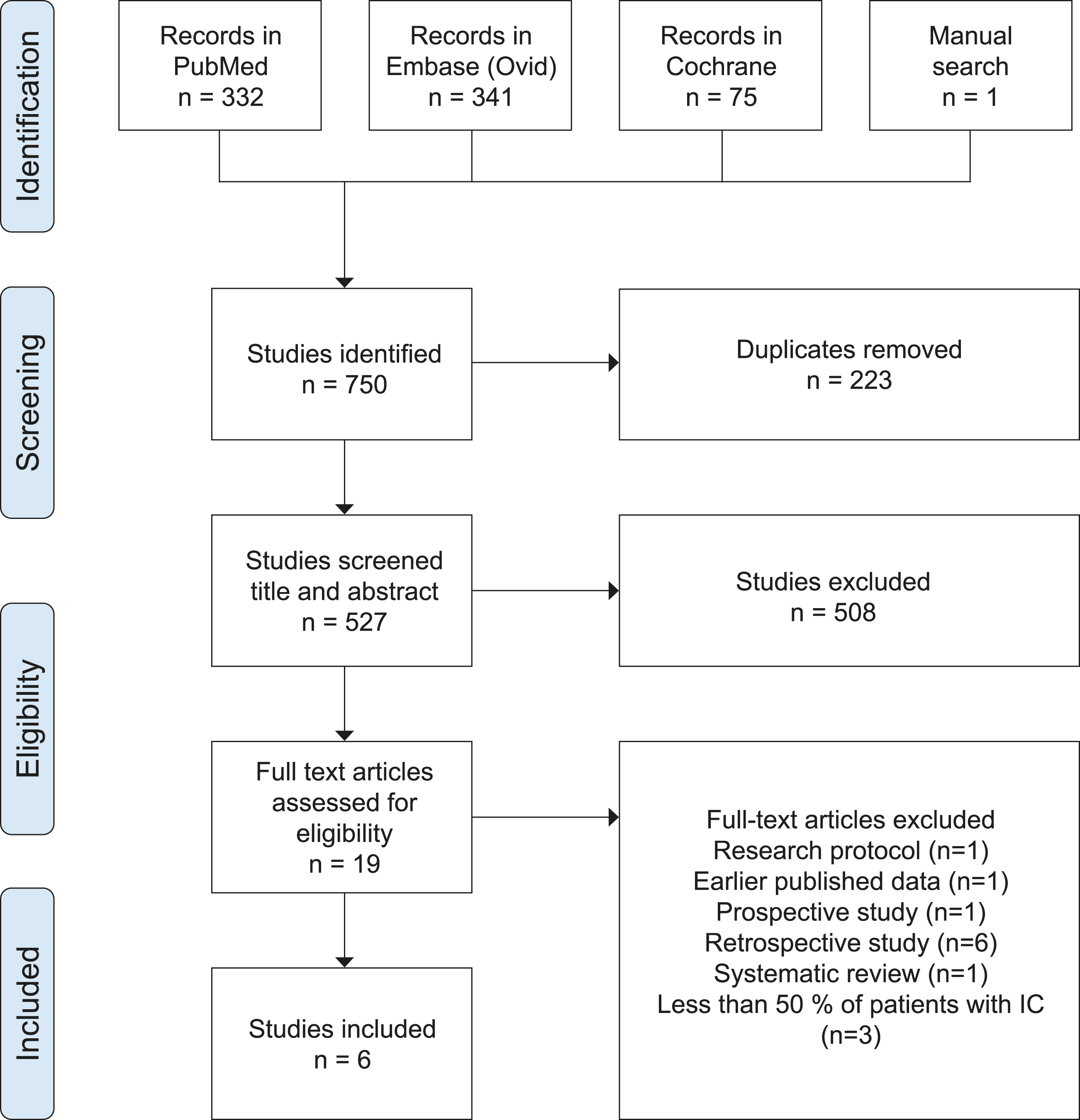
Study descriptions
Study characteristics.
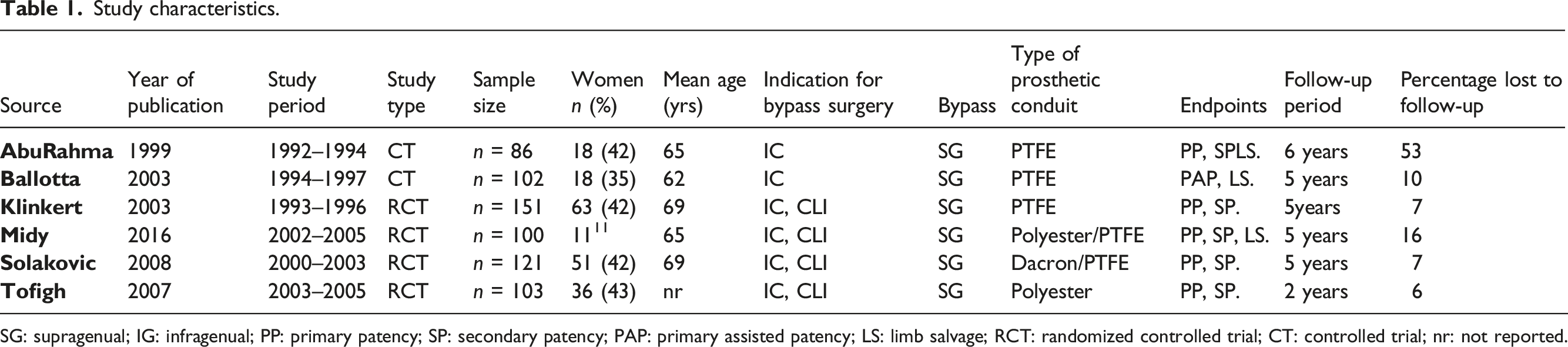
SG: supragenual; IG: infragenual; PP: primary patency; SP: secondary patency; PAP: primary assisted patency; LS: limb salvage; RCT: randomized controlled trial; CT: controlled trial; nr: not reported.
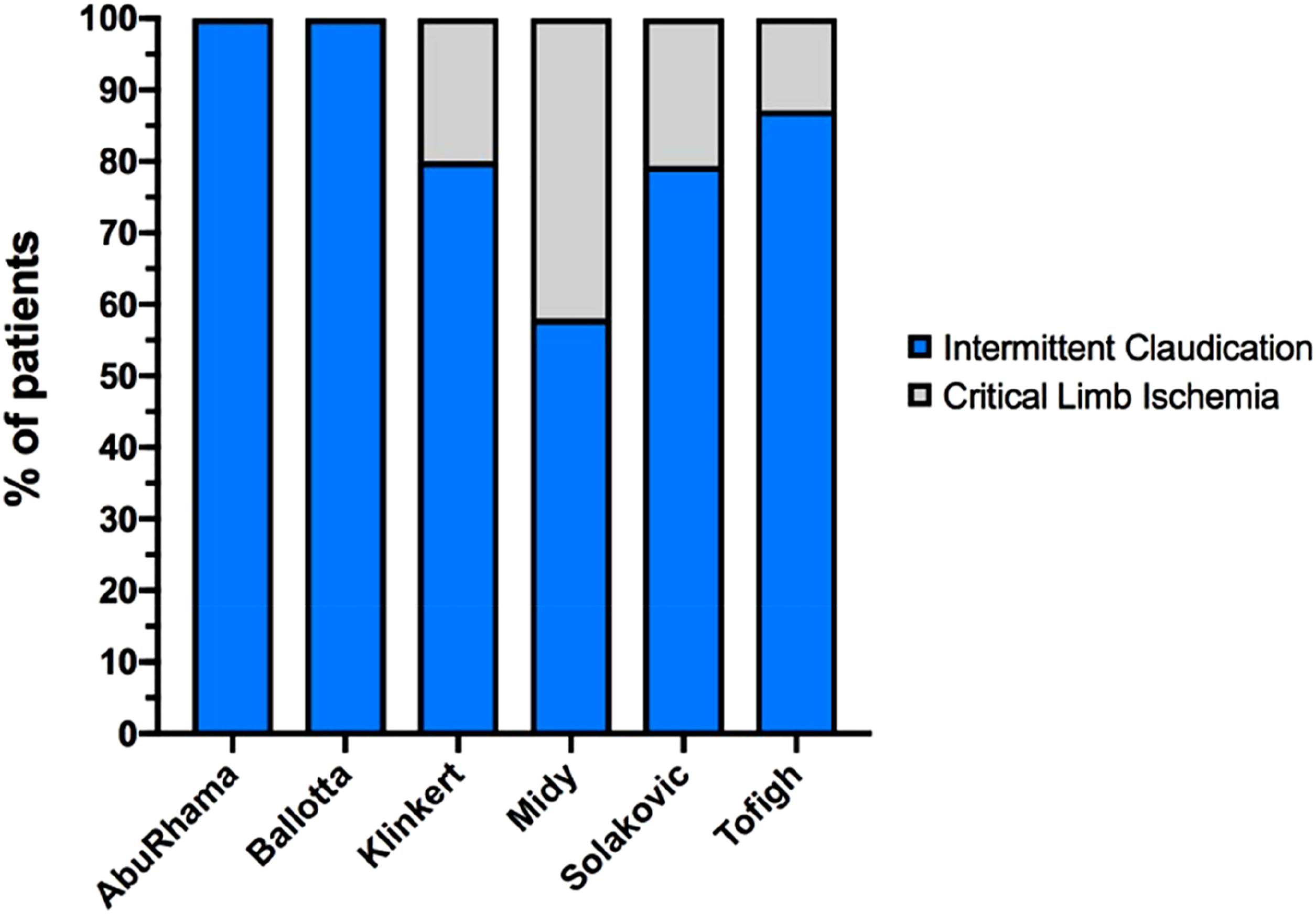
Indications for femoropopliteal bypass surgery.
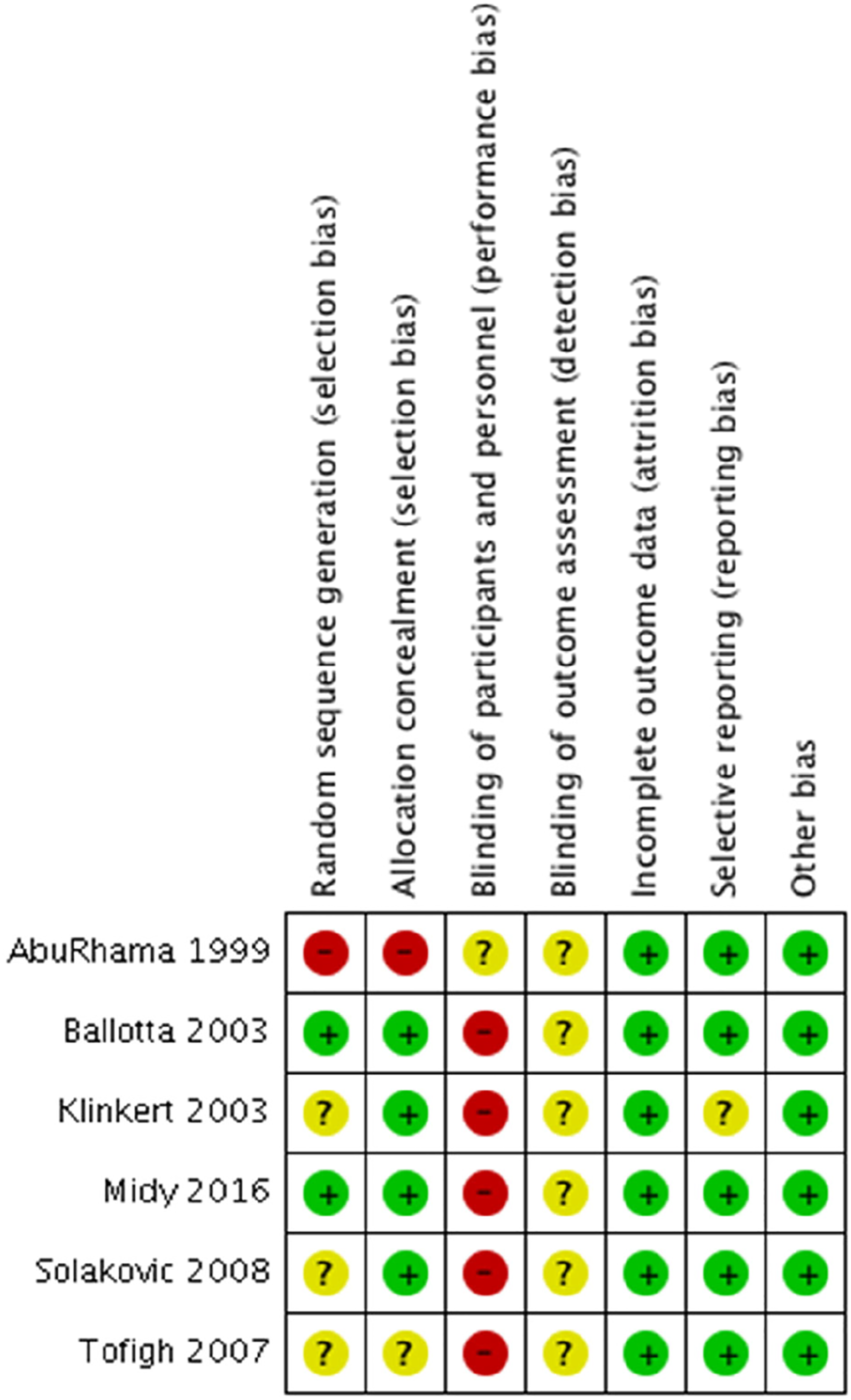
Risk of bias summary of each included study.
Primary analysis
Primary patency
Primary patency rates were reported by only one study. 11 One and 5-year patency rates were 88% and 76% versus 81% and 68% for the ASV and the PTFE groups, respectively (p = .85). At 5-year follow-up, 10 of 43 vs 13 of 43 bypasses were occluded in the ASV group and PTFE groups, respectively. No significant difference between the two conduits was found, with an OR of 1.74 (95% CI 0.52–5.81) at 1-year follow-up and 1.43 (95% CI 0.55–3.74) at 5-year follow-up. However, long term results need to be interpreted cautiously, as this study had a large number of censored patients, starting at 3 years follow-up.
Patency
The pooled outcome of two studies (n = 94, both controlled trials) showed no significant difference in both short- and long-term patency between the two groups. At 1-year follow-up, zero versus four bypasses were occluded in favor of the ASV, resulting in an OR of 5.21 (95% CI 0.60–45.36) (Figure 4(a)). At 5-year follow-up, nine versus 17 bypasses were occluded in favor of the ASV group, which was not significantly different between the two groups (OR 2.10; 95% CI 0.88–5.01) (Figure 4(b)). Patency of prosthetic conduit versus autogenous vein at 1-year follow-up 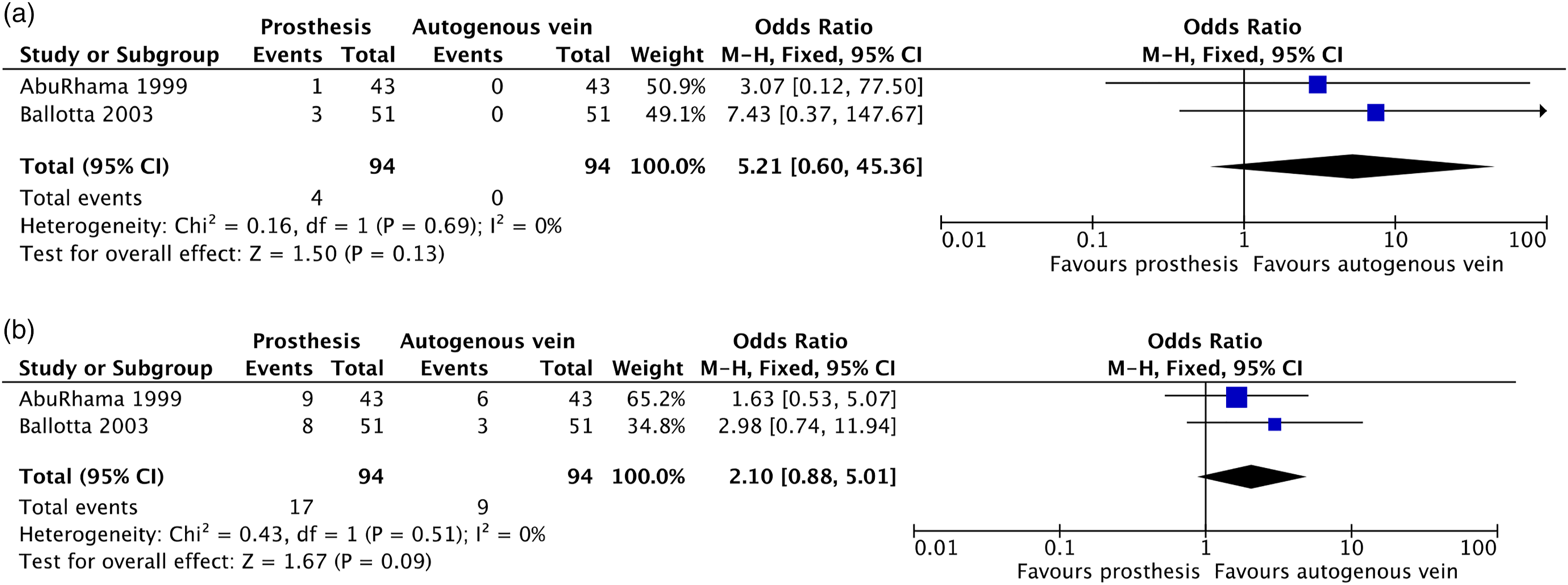
Secondary analysis
Primary patency (mixed study group (>50% CI)
Five studies reported on primary patency.11,16–19 The RCT by Midy et al., reports no significant difference between the two treatment groups at 5-year follow-up.
18
Their study population consisted of 58% of patients with IC. However, these results need to be interpreted with caution, as the predefined study size was not met and there was a high rate of loss to follow-up in this study. Data could not be extracted for meta-analysis. Four studies were included for meta-analysis.11,17-20 These studies included both patients with IC and CLI with an average of 84% patients with IC. The 1-year primary patency rates did not significantly differ between the treatment groups (OR 1.40, 95% CI 0.87–2.25, Figure 5(a)). Patients who were treated with ASV had significantly better results on long-term primary patency, which became apparent at 3-year follow-up. After a follow-up period of 5 years, the use of ASV resulted in significantly better results compared with a prosthetic graft, with an OR of 2.06 (95% CI 1.30–3.26, Figure 5(b)). Primary patency of prosthetic conduit versus autogenous vein at 1-year follow-up–mixed population 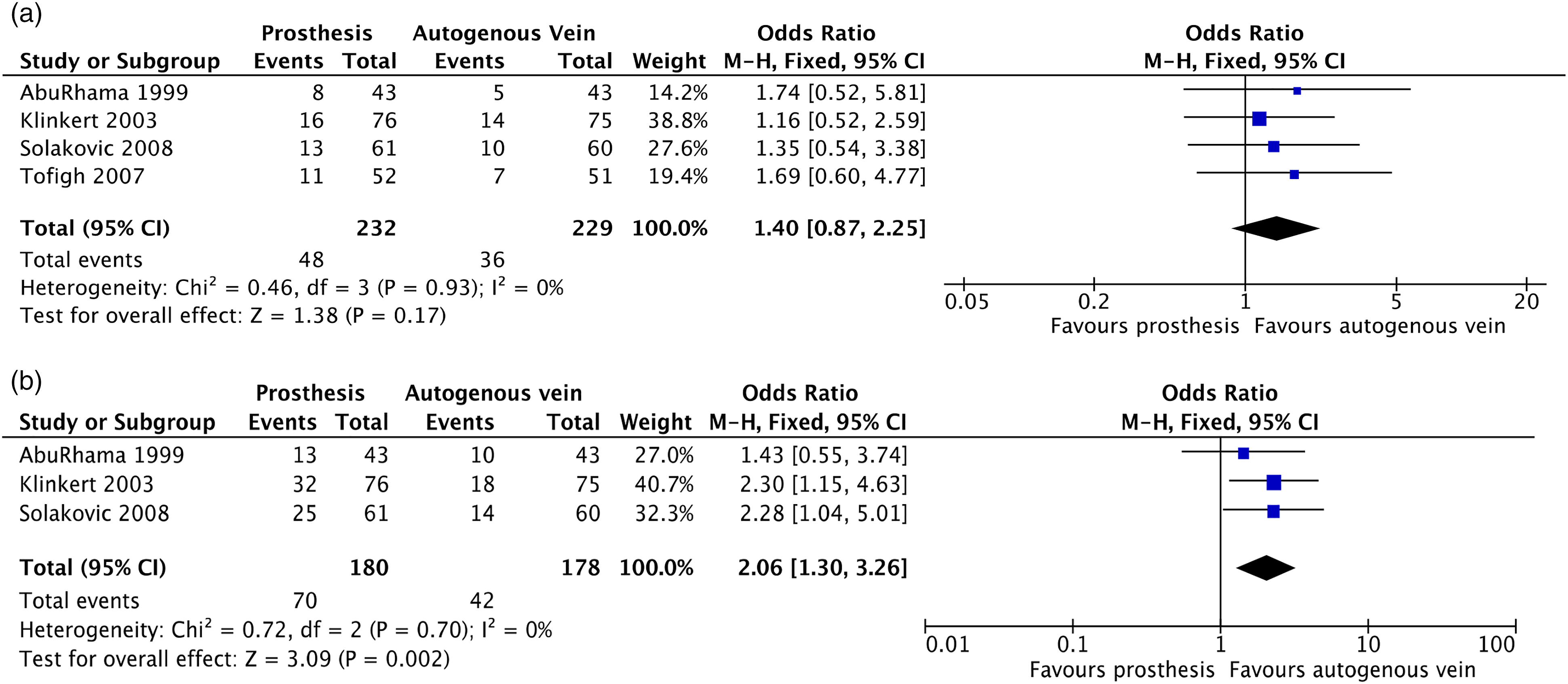
Secondary patency (mixed study group (>50% CI))
Five studies reported on secondary patency.11,17-20 The study by Midy et al., reported on the non-inferiority of the prosthetic conduit versus the ASV in above-the-knee femoropopliteal bypasses.
18
In their under-treatment analysis, 5-year secondary patency rates were comparable in both groups, with percentages of 96.2% versus 90.5% in the prosthetic and vein groups, respectively. The meta-analyses of the remaining four studies that reported on secondary patency are shown in Figure 6(a) and (b). The 1-year secondary patency rates did not significantly differ between the two treatment groups (OR 1.32, 95% CI 0.74–2.32). At 5-year follow-up, the use of the ASV resulted in significantly better results with an OR of 2.48 (95% CI 1.50–4.09). Secondary patency of prosthetic conduit versus autogenous vein at 1-year follow-up–mixed population 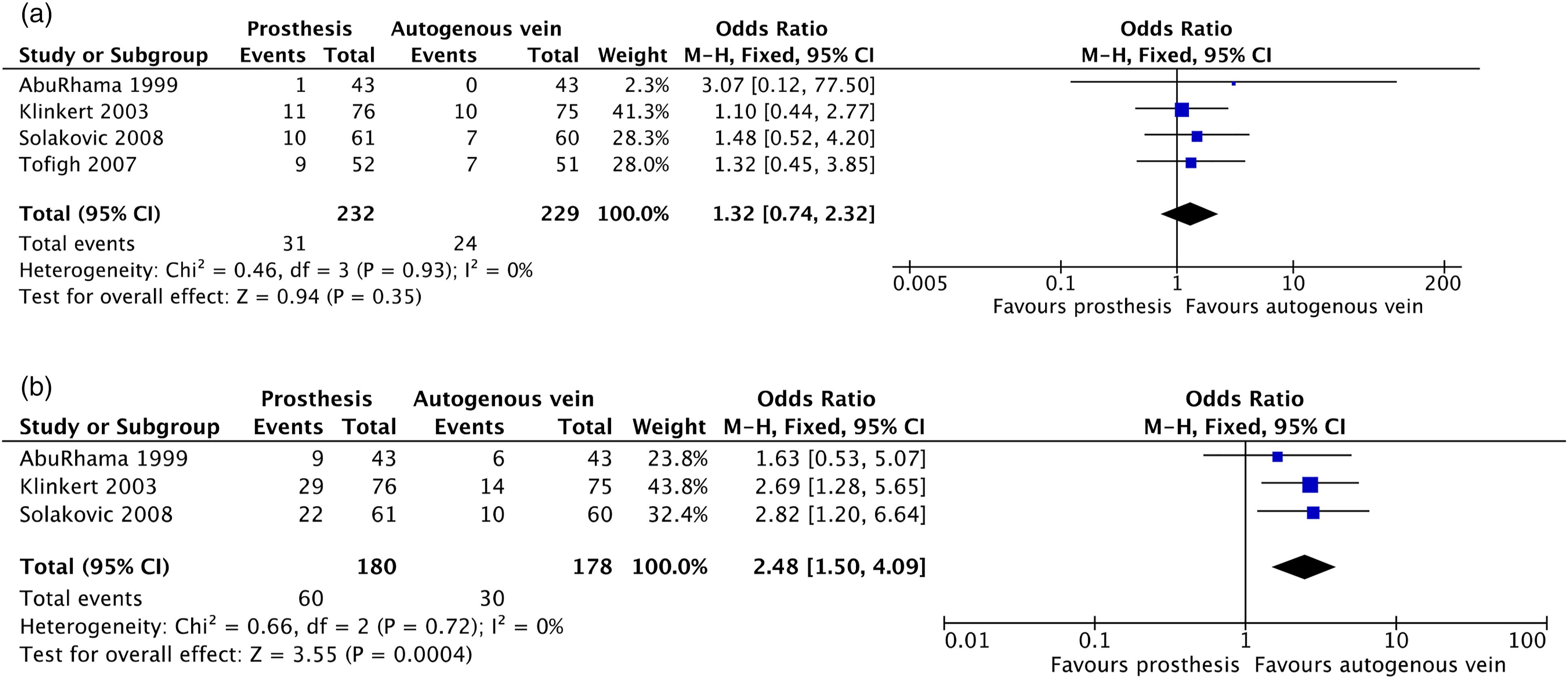
Limb salvage
Limb salvage.
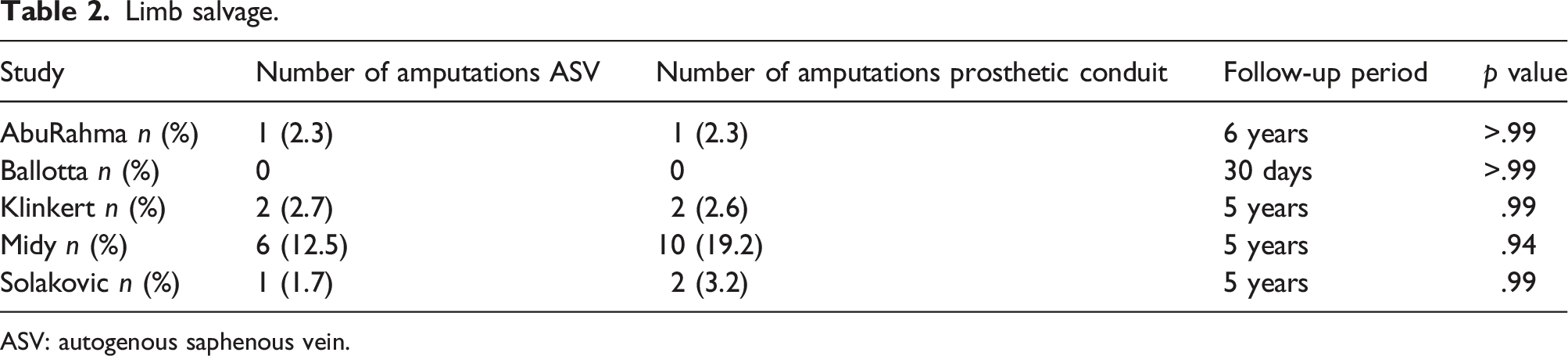
ASV: autogenous saphenous vein.
Complications
Complications.
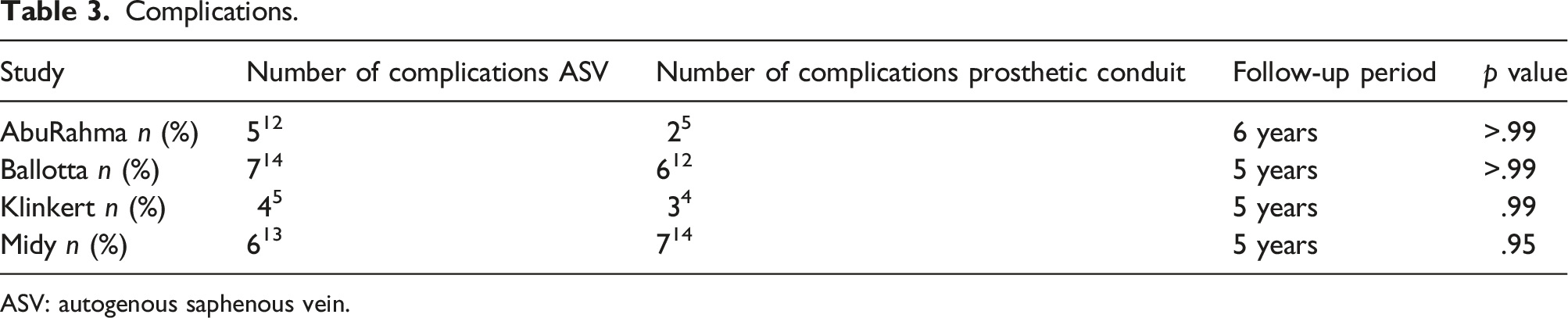
ASV: autogenous saphenous vein.
Mortality
Five studies investigated the incidence of mortality.11,16–19 Three studies reported that they had no 30-day perioperative deaths.11,16,17 In the study by Klinkert et al., a non-significant difference was found for mortality; 24 patients in the ASV group and 18 in the PTFE group had died by the time of 5-year follow-up (p > .99). 17 Midy reported a lower mortality rate in the ASV group than in the prosthetic group at 5-year follow-up, although this was not significantly different between the two groups (11 vs 14 patients, respectively, p = .92). 18 Solakovic et al., reported no deaths during their 5-year follow-up. 19 Mortality rates from the studies of AbuRahma and Ballotta were not distinguishable per intervention group due to their study designs.11,16 Nevertheless, they reported no perioperative (i.e., 30-day) deaths. However, four and five late deaths were reported, all resulting from myocardial infarctions or cancer. The mortality data of three studies were pooled and resulted in no significant difference between the groups (OR 0.84; 95% CI 0.48–1.47).17–19
Discussion
Summary of evidence
The aim of this study was to investigate the outcome of using either the ASV or a prosthetic graft as a conduit for femoropopliteal bypass surgery in patients with IC. Our systematic search revealed only two studies that solely reported on patients with IC. The pooled data of these two controlled trials of low to moderate quality showed no significant difference in either short- or long-term outcome between the two types of conduits. However, the pooled analysis of a mixed population of patients with IC and CLI, with a proportion of 84% IC patients, showed comparable results on short-term outcome, but a favorable outcome for the ASV starting at 3 years of follow-up. Based on these findings, the ASV remains the conduit of choice, but a prosthetic conduit can be used as a good alternative in patients with IC, especially if the ASV is absent or of questionable quality.
Although several studies have published results on the use of a prosthetic versus venous bypass, there is still controversy concerning which conduit should ideally be used for the individual patient, especially if the ipsi- or contralateral ASV is of questionable quality. To our knowledge, we are the first systematic review to look at indication for surgery rather than location of anastomosis. Most studies publish results stratified by location of distal anastomosis, for example, above-the-knee and below-the-knee bypasses, instead of based on indication for surgery such as IC of CLI.20–23 It is widely acknowledged that in femoropopliteal bypass surgery a vein bypass is preferable to a prosthetic graft.22–24 Interestingly, however, a recent Cochrane review underlines the lack of available evidence on graft type in below-the-knee bypass surgery. 22 Daily practice in these patients is thus driven by common sense and clinical experience instead of driven by high quality evidence.
In this review, our goal was to specifically explore results of patients with a mild form of peripheral artery disease: IC. Compared with patients with CLI, patients with claudication have a more benign disease prognosis and usually a better distal outflow trajectory. Earlier results showing the advantage of the ASV over a prosthetic graft might be less pronounced in this specific patient category. We identified only two studies that only included patients with claudication. All patients underwent above-the-knee bypasses and all patients had a good distal outflow with 2–3 vessel runoff, which implies a high-flow bypass. In the analysis of the mixed population of patients with both IC and CLI, results for the prosthetic graft were comparable up to 3-year follow-up. This applies to both primary patency and secondary patency rates. Complication and amputation rates did not differ significantly between the two groups. It is possible that the long-term success of the vein graft has been overestimated due to the inclusion of patients with CLI in these studies. Unfortunately, we were not able to extract data from patients with only claudication to support this hypothesis.
The main advantage of a prosthetic bypass compared with the ASV, is the less extensive surgery and shorter procedure time, which might subsequently lead to lower complication rates. Only four studies reported on complication rates. None of the studies reported on the occurrence of a prosthetic graft infection. A prosthetic graft infection is a very undesirable condition that has been described in 1%–6% of patients undergoing prosthetic bypass surgery.25,26 This complication could well lead to removal of the entire bypass. However, an important limitation of these earlier described prevalence data is that they are derived from studies that incorporated both patients with IC and CLI in their analyses. As a secondary outcome of our analysis, we aimed to investigate functional outcome in patients who underwent ASV surgery and patients who underwent prosthetic bypass surgery. Although patient-reported outcome measures (PROMs) are increasingly being recognized as important outcome variables when evaluating vascular treatments, we found no studies that incorporated these outcomes into their analyses. 27 Patients with IC, in particular, might benefit from such an analysis, as the therapeutic goal is to improve their functional status. An evaluation of functional outcome is more in line with the indication for surgery, and can aid in the treatment decision process for this specific group of patients.
Limitations
Inherent to a meta-analysis with a variety of studies, some limitations exist. Therefore, our results should be interpreted with caution. Firstly, the quality of the studies was low to moderate. Secondly, a type II statistical error might be present, meaning that we incorrectly assumed that both conduits show comparable results in patients with intermittent claudication. A significant difference might become apparent when larger trials are performed in this specific group of patients. Thirdly, this systematic review comprises studies carried out between 1992 and 2005. The therapeutic approach to patients with IC has changed over time. Nowadays, guidelines advocate starting with a conservative approach, including supervised exercise training, and reserving invasive interventions for patients with severe IC in whom conservative management has not been successful. It is possible that in the modern surgical era patients with IC who are found to be eligible for bypass surgery, are a selected group of patients with a more severe form of IC when compared with the patients that were included in the studies. Fourthly, we included both studies with both PTFE and polyester/Dacron grafts. Previous studies have shown comparable results for both conduits, although there is some evidence to suggest a slightly better outcome in favor of polyester grafts in femoropopliteal bypass surgery.23,28–30 In our study, we were not able to extrapolate any results of the different prosthetic conduits. Lastly, outcome measures were not always consistent. Although AbuRahma reported on primary, primary assisted, and secondary patency, Ballotta only reported on primary “assisted” patency. Moreover, their definition of primary assisted patency is slightly different. AbuRahma defined primary assisted patency as patency assisted by simple measures such as angioplasty, but Ballotta et al., states that remedial surgery for late bypass stenosis was not considered a patency failure. In their study, secondary patency was not considered to be an endpoint. We combined these variables as overall patency rates, in order to achieve the best possible estimate of post-intervention patency.
Conclusion
This systematic review shows that there is no high-quality literature that specifically reports on patients with intermittent claudication undergoing femoropopliteal bypass surgery. The ASV remains the conduit of choice for femoro-popliteal bypass surgery. However, the prosthetic conduit seems a feasible alternative for patients with intermittent claudication in whom the ASV is not present or unsuitable. Additional good quality research, which ideally also incorporates functional outcomes, is needed to further empower these conclusions.
Footnotes
Acknowledgements
The authors wish to thank S. Priester-Vink, OLVG Hospital Amsterdam, and F.S. van Etten-Jamaludin, Amsterdam UMC, for providing help with the literature search.
Contributions of the authors
Concept by R.J.V. and A.C.V. Study search and selection by R.J.V. and T.M.F. Writing of the article by R.J.V. All authors discuss the results and commented on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.