
Abstract
Although exostosis or osteochondroma is a common bone tumor, associated vascular complications are rare. Clinical and radiological diagnoses are sometimes challenging, and there is no codification for surgical management. We report two cases of popliteal arterial pseudoaneurysms due to osteochondroma of the distal femur. A review of the current literature about case series and case reports of patients affected by arterial pseudoaneurysm complicating osteochondroma was also performed.
Introduction
Osteochondroma or exostosis is a common benign bone tumor, usually affecting either lower or upper extremities during childhood and adolescence. 1 Osteochondroma usually causes local pain or swelling, but in extremely rare cases it may involve the nearby vascular structures leading to the development of venous and/or arterial complications. 2 Among these complications, false arterial aneurysm of the popliteal artery is the most represented. 3 Arterial pseudoaneurysm usually develops as soft and tender mass over weeks or months and may be sometimes misdiagnosed, 1 leading to a delay in proper treatment with possible consequences on the normal function of the affected limb. Furthermore, there is no codification of surgical management related to arterial pseudoaneurysm of the popliteal artery.
We report two cases of false arterial aneurysms of the popliteal artery caused by bone exostosis of the distal femur, along with a review of the current literature. For the literature review, the search was conducted on PubMed and Embase using the words “osteochondroma pseudoaneurysm” on August 31, 2021. All search results were restricted to English, Italian, and French languages. Studies included case series and case reports of patients affected by arterial pseudoaneurysm complicating osteochondroma. We collected data about the localization of the pseudoaneurysm, the clinical presentation, the diagnosis, the treatment, and the outcomes.
Case report 1
A five-year-old male child was admitted for a painful swelling of the posterior-medial side of the right thigh, which had occurred in the previous weeks. Medical history revealed a trauma during a football game two years before. Physical examination showed a tender pulsatile mass of the popliteal fossa without discoloration of the skin, and peripheral pulses were also present. Duplex ultrasound was performed, showing the presence of a pseudoaneurysm of the right femoral-popliteal artery junction measuring 45 x 66 mm, without any venous injury. Therefore, a Computed Tomography Angiography (CTA) and an X-ray were performed, confirming the presence of the pseudoaneurysm caused by a small posterior erosion in the vessel wall, which was close to a bone osteochondroma of the distal femoral diaphysis (Figure 1). Questioning revealed no family history of osteochondroma. The patient was then referred to open surgery repair with a combined orthopedic and vascular approach. After a surgical medial approach to the distal third of the thigh, proximal and distal arterial control of the pseudoaneurysm was obtained. The pseudoaneurysm was then opened and resected, and the artery was repaired using a small bovine pericardium patch. The bone exostosis was then excised and sent to histologic analysis, which confirmed the diagnosis of osteochondroma. The postoperative course was uneventful, and the patient was discharged after one week on a single antiplatelet therapy (Acetyl-Salicylic Acid 100 mg/daily) for 6 months. One year after surgery, the patient is having a normal school life with no limitation on his physical activity. Computed Tomography Angiography scan showing the pseudoaneurysm arising from a hole (yellow arrow) in the distal part of the superficial femoral artery and extending towards the popliteal fossa.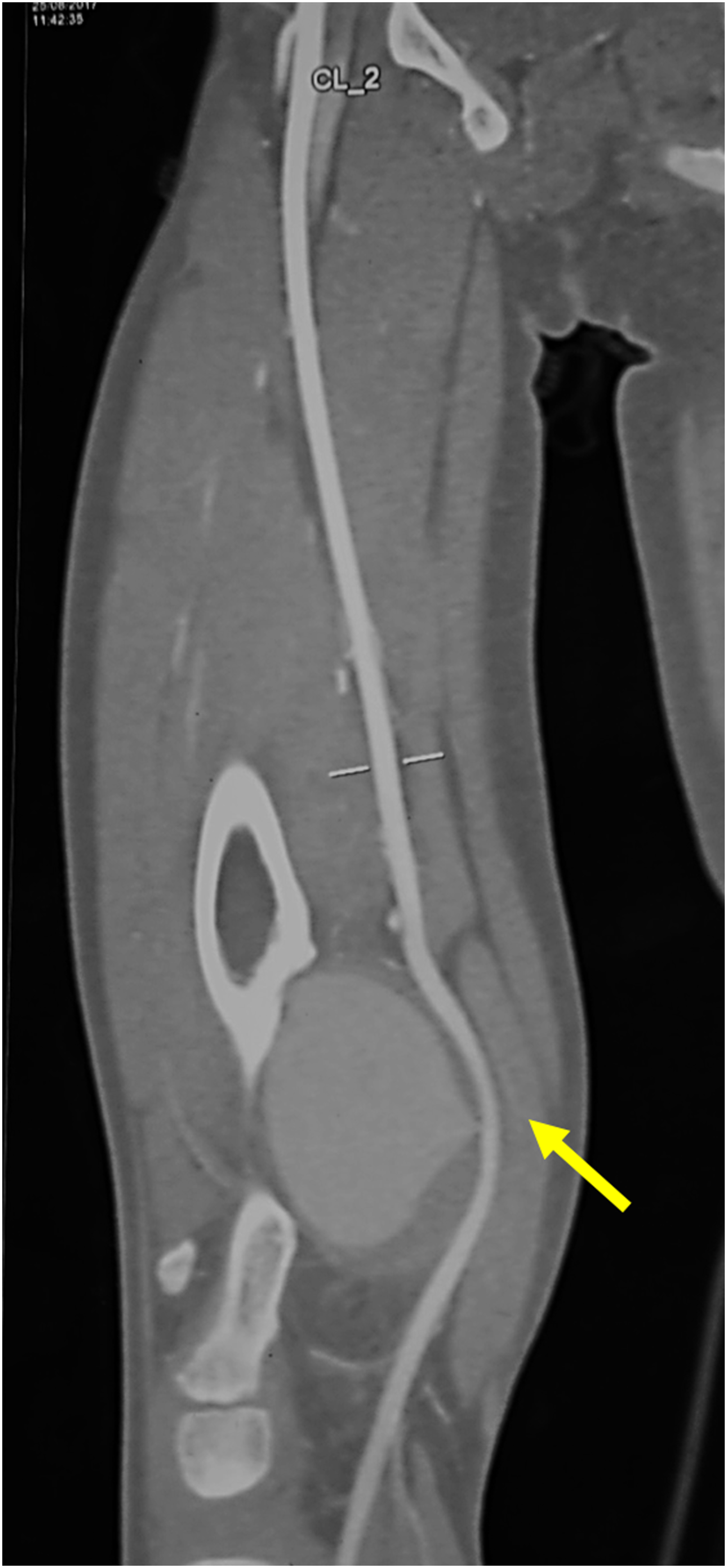
Case report 2
A 20-year-old male patient with no medical past history was admitted for a painful swelling of his right popliteal fossa. This swelling had been growing silently for two years, without any prior history of trauma, and had become painful during the last week. A huge pulsatile mass in the popliteal fossa was discovered during physical examination, and peripheral pulses were present. Doppler ultrasound was performed, showing a large pseudoaneurysm in the popliteal fossa. X-ray of the knee revealed a bony growth on the posterior part of the distal femoral metaphysis. CTA was then performed, showing an osteochondroma of the posterior face of the distal femoral metaphysis complicated with a popliteal pseudoaneurysm of 93 x 74 in diameters (Figure 2), which extended longitudinally for 150 mm. Surgery was then performed. Using a medial approach with a surgical incision at the distal third of the thigh, the pseudoaneurysm was decompressed. A reversed autologous saphenous vein graft interposition was performed for arterial reconstruction, since the artery had a huge damage and could not be repaired using a simple patch. The bone exostosis was then excised. The postoperative course was uneventful, and the patient was discharged after 5 days on a single antiplatelet therapy (Acetyl-Salicylic Acid 100 mg/daily) for 6 months. The bone biopsy indicated a Langerhans Histiocytosis. At one year’s follow-up, the patient is doing well. Computed Tomography Angiography scan showing the huge pseudoaneurysm (yellow arrow) and the osteochondroma of the posterior face of the distal femoral metaphysis (red arrow).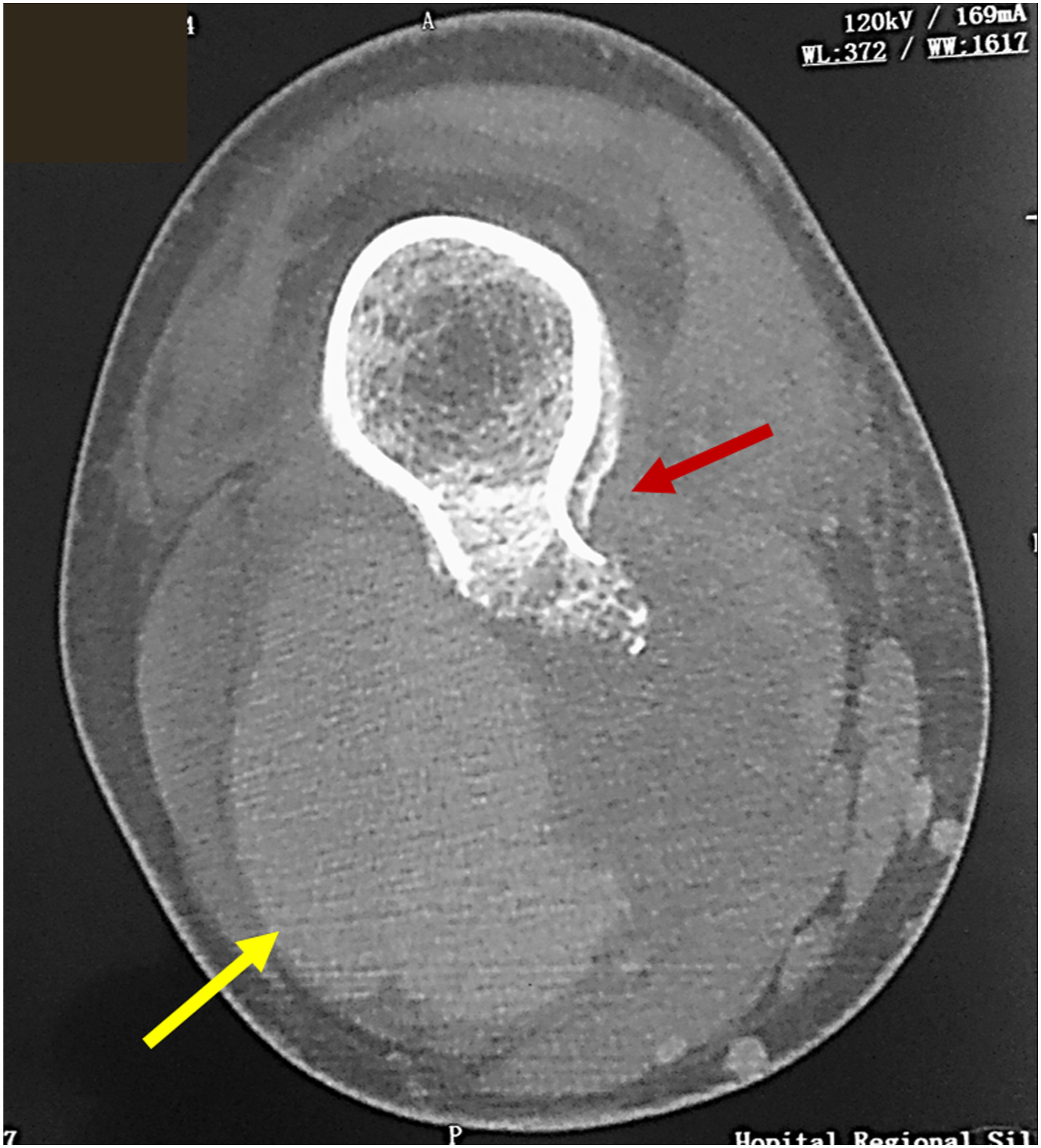
Discussion and literature review
A total of 87 arterial aneurysms in patients presenting osteochondroma were identified from 1963 to 2021. Patients were predominantly male (70.1%), with a mean age of 21.8 ± 11.5 years but ranging from 8 4 to 48 5 years old, and we described the case of the youngest patient in the literature having a pseudoaneurysm in osteochondroma, according to our results.
Osteochondroma are usually asymptomatic and complications may occur in just 4% of cases. 2 These complications include neurologic compromise, malignant degeneration, growth abnormality and vascular damage. This latter in particular, in the form of arterial-venous fistula formation, false aneurysm development, vessel occlusion or stenosis, are extremely rare.
The most affected vessels were the popliteal artery (70.1%) and the distal superficial femoral artery (16%). Pseudoaneurysms of the common femoral artery were reported in three cases,1, 6, 7 and there was a unique case of deep femoral artery involvement. 8 The upper limb was also affected by this complication. In particular, brachial pseudoaneurysms were reported in seven cases, while the subclavian artery was involved in one case. 9
Summary of the results of the literature review.
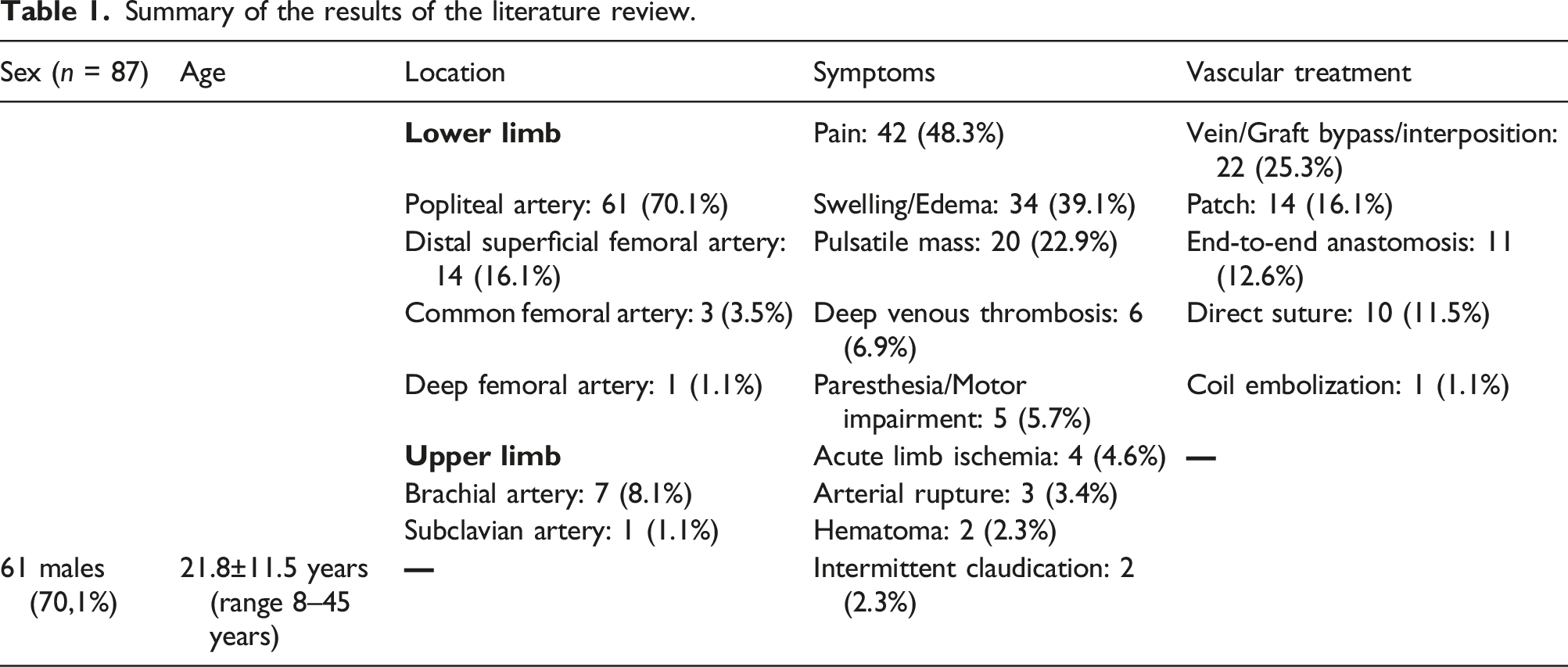
The venous system was involved in about 7% of cases, especially in the form of deep venous thrombosis by external compression.18-23
Peripheral nerve compression with neurologic symptoms of paresthesia/dysesthesia or even motor impairment was also described in five cases.20, 24-27 In such cases, complete recovery of neurologic functions after surgical treatment required a longer time and usually involved adjunctive physical therapy.
In about a quarter of the cases, a previous blunt trauma was present in the patient’s medical history. Nasr et al. , 3 in their review of 57 cases from 1965 to 2013, showed that repetitive microtraumas by the bone spike lead to the perforation of the artery wall, and trauma was the trigger in 39% of cases. Popliteal artery flexibility explains the frequency of false aneurysm occurrence at its proximal and distal segments. 28
Diagnosis of osteochondroma and the suspicion of complication were based on medical history and clinical examination, but multimodality imaging with duplex ultrasound, CTA, and bone X-ray were mandatory for a proper preoperative assessment, as described in the proposed algorithm (Figure 3). Angiography was also performed in some patients,8, 10, 24, 29 but it was most used during the past years. A proposed algorithm for the diagnosis and management of vascular complications associated with osteochondroma. CT: Computed Tomography; MR: Magnetic Resonance.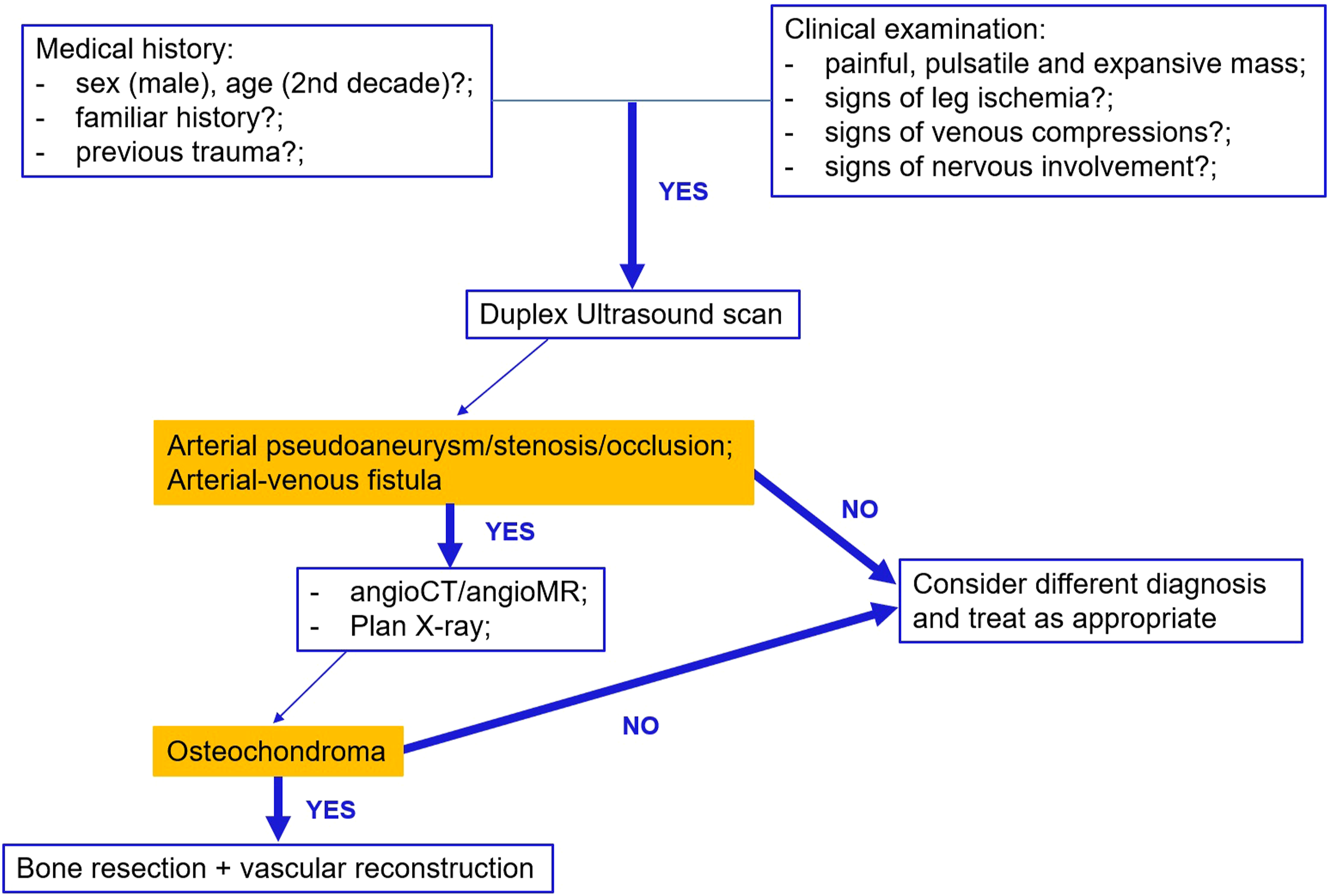
Surgical treatment was required in all cases to ensure the resection of the exostosis and of the ligation/resection of the aneurysmal mass.
In most cases, an open approach was chosen. Open surgery allowed the treatment of the pseudoaneurysm and bone exostosis resection at the same time. Particularly, in about a quarter of cases, the arterial reconstruction was performed using a graft interposition, typically of the autologous saphenous vein. When feasible, pseudoaneurysm resection and arterial reconstruction with end-to-end anastomosis was also a treatment option. In the remaining cases, a venous patch or even direct suture were performed (Table 1). Raherinantenaina et al. 30 reported that the most common surgical repair performed for vascular complications of osteochondromas were, respectively, vein bypass grafting in 40% of cases, lateral suture in 39% of cases, and resection with end-to-end anastomosis in 14% of cases.
Endovascular techniques with coil embolization were used in two cases only, in which the pseudoaneurysm was located in the deep femoral artery 8 and the superficial femoral artery, 31 respectively. Endovascular treatment in fact would not be ideal in young patients, especially in popliteal area. Furthermore, the adjacent osteochondroma needs to be excised anyway with a surgical approach.
A regular postoperative course with neither complications nor recurrence was described in all cases during follow-up, which was reported to be up to five years. 5
Preventive treatment of asymptomatic forms is discussed. 32 Vascular examination and monitoring by Doppler ultrasound have been mentioned by some authors, but most authors recommend preventive removal of a solitary exostosis when adjacent to neurovascular structures, especially in the femoro-popliteal junction.28, 33
Conclusion
False aneurysms should be considered in young patients presenting painful swelling or pulsatile masses in the extremities whether or not medical history reveals the presence of an osteochondroma. Usually a multimodality imaging approach can be helpful in differential diagnosis to exclude malignancies. Surgical treatment is mandatory and must combine the osteochondroma excision with the pseudoaneurysm repair.
Footnotes
Author contributions
RM
Study design, data collection, data analysis, writing of the manuscript, critical revision, and final approval
DM
Study design, data collection, data analysis, writing of the manuscript, critical revision, and final approval
BD
data collection, critical revision, and final approval
ZD
data collection, critical revision, and final approval
IBM
data collection, critical revision, and final approval
MBM
data collection, critical revision, and final approval
JZ
data collection, data analysis, and final approval
PR
critical revision and final approval
MG
critical revision and final approval
GN
critical revision and final approval
RD
critical revision and final approval
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patients’ consent
The patients gave consent to the anonymous publication of their medical records for research purposes.