
Abstract
Objective
The Wound, Ischemia, and foot Infection (WIfI) clinical stage has been thought to have a prognostic value in Chronic limb-threatening ischemia (CLTI) patients, and frailty and nutritional status appear to represent pivotal factor affecting prognosis among CLTI patients. The purpose of this study was to examine clinical factors (including frailty and nutritional status) relevant to WIfI clinical stage.
Methods
This retrospective study investigated 200 consecutive CLTI patients. We individually assessed WIfI clinical stage, frailty according to the Clinical Frailty Scale (CFS) score, and malnutrition according to Geriatric Nutritional Risk Index (GNRI). We then compared mortality after endovascular intervention between a WIfI stage 1, 2 group and a stage 3, 4 group, and investigated associations between baseline characteristics (including CFS and GNRI) and WIfI clinical stage.
Results
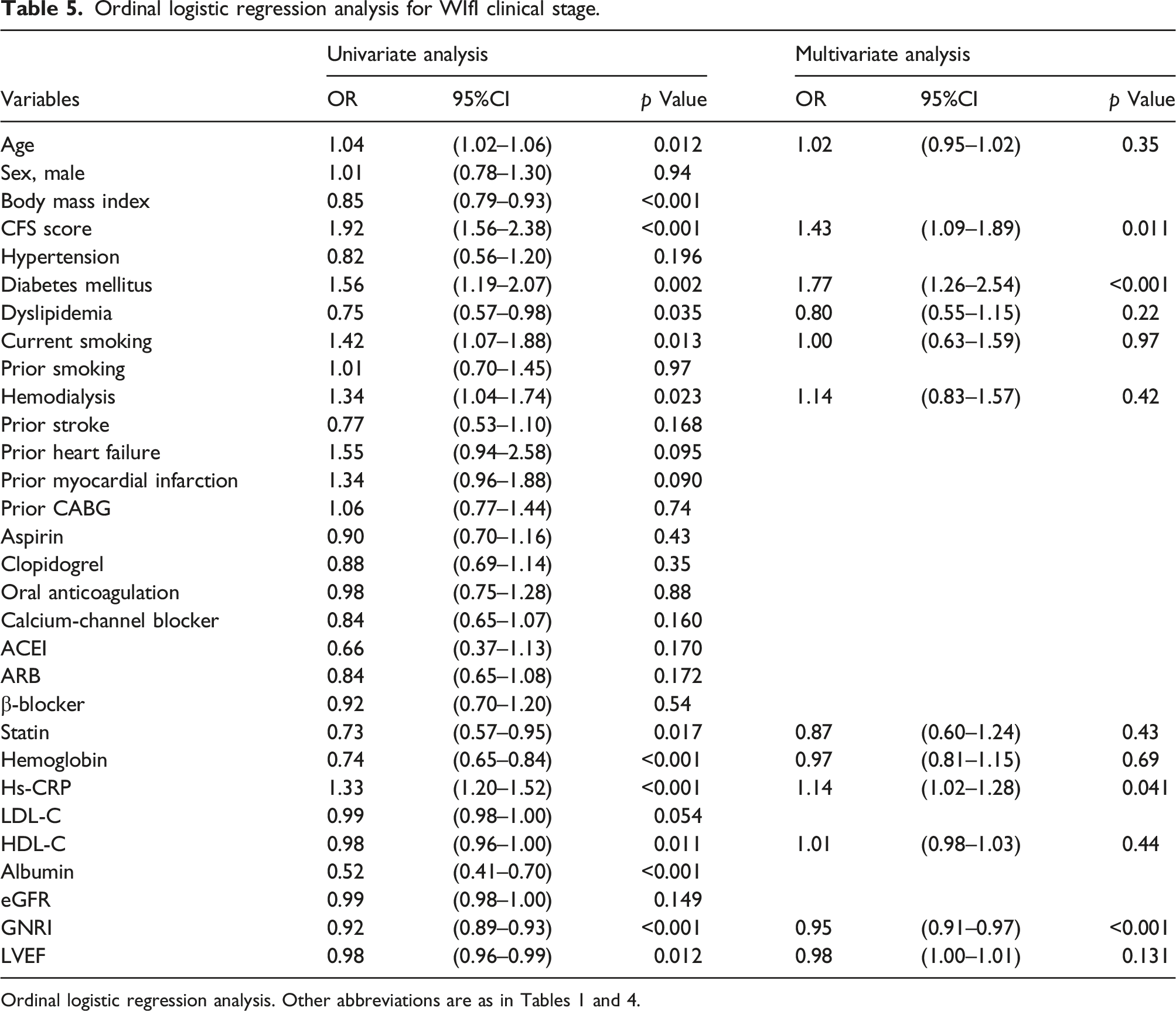
Among 200 patients, 123 patients (62%) showed WIfI stage 1 or 2, and the remaining 77 patients (38%) had WIfI stage 3 or 4. CFS score was significantly higher in the WIfI stage 3, 4 group [median 6.0, interquartile range (IQR) 5.5–7.0] compared with the WIfI stage 1, 2 group (median 5.0, IQR 4.0–6.0, p < 0.001), and GNRI was significantly lower in the WIfI stage 3, 4 group (median 88, IQR 80–97) than in the WIfI stage 1, 2 (median 103, IQR 94–111, p < 0.001). Forty patients (20%) died after endovascular intervention. Incidences of all-cause and cardiac deaths were higher in the WIfI stage 3, 4 group than in the WIfI stage 1, 2 group (27% vs. 15%, p = 0.047 and 12% vs. 3%, p = 0.040, respectively). Kaplan–Meier analysis showed a significantly lower survival rate in the WIfI stage 3, 4 group than in the WIfI stage 1, 2 group (p = 0.002 by log-rank test). Multivariate logistic regression analysis using relevant factors from univariate analysis showed CFS score [odds ratio (OR) 2.06, 95% confidence interval (CI) 1.41–3.13, p < 0.001), diabetes mellitus (OR 3.17, 95%CI 1.17–8.61, p = 0.023) and GNRI (OR 0.93, 95%CI 0.89–0.97, p = 0.002) significantly associated with WIfI stage 3 or 4. In addition, multivariate ordinal logistic regression analysis for WIfI clinical stage showed CFS score (OR 1.43, 95%CI 1.09–1.89, p = 0.011), diabetes mellitus (OR 1.77, 95%CI 1.26–2.54, p < 0.001), and high-sensitivity C-reactive protein (OR 1.14, 95%CI 1.02–1.28, p = 0.041) were positively associated with WIfI clinical stage, and GNRI correlated negatively with WIfI clinical stage (OR 0.95, 95%CI 0.91–0.97, p < 0.001).
Conclusions
These results indicate that CLTI patients with high WIfI clinical stage may be more frail and malnourished, and be associated with poor prognosis after endovascular intervention.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) represents the end-stage manifestation of peripheral artery disease. 1 A recent meta-analysis found that among untreated CLTI patients, all-cause mortality was 22% during a median follow-up of 12 months 2 In addition, even if CLTI patients undergo revascularization, they still exhibit poor prognosis with a high mortality rate due to cardiovascular and infectious diseases.3,4 Recently, the Society for Vascular Surgery established the Wound, Ischemia, and foot Infection (WIfI) classification system, focusing on disease severity rather than arterial lesion characteristics. 5 The WIfI classification, which is stratified into four clinical stages, is originally based on assessment of the 1-year risk of amputation in CLTI patients. 5 Recent studies have shown that higher WIfI clinical stages involved a high all-cause death rate.6,7 Thus, WIfI clinical stage has been thought to have a prognostic value in CLTI patients.
Based on the accumulated evidence, frailty and nutritional status are recognized as important factors that affect the prognosis of patients with cardiovascular disease.8,9 Recent studies have demonstrated that frailty as assessed by the Clinical Frailty Scale (CFS) 10 and malnutrition as assessed by Geriatric Nutritional Risk Index (GNRI) 11 were independently associated with overall survival rate among patients with CLTI.12,13 Therefore, as with WIfI clinical stage, frailty and malnutrition appear to represent pivotal factors affecting the prognosis of CLTI patients. However, few reports have addressed associations between WIfI clinical stage and frailty or malnutrition. The current study examined clinical factors (including frailty and malnutrition) relevant to WIfI clinical stage and investigated mortality of CLTI patients undergoing endovascular intervention based on WIfI clinical stage.
Methods
Patient population
This study was a retrospective cohort study at a single center, investigating 211 consecutive CLTI patients who underwent revascularization for peripheral artery disease by endovascular intervention between February 2015 and March 2019. CLTI was diagnosed according to European Society of Cardiology guidelines. 14 All patients underwent endovascular intervention using a standard technique with or without stenting, and successful endovascular intervention was defined as the establishment of at least one straight-line flow to the foot. Patients were followed-up at our hospital or by their physician. However, 11 patients were lost to follow-up. The final number of patients recruited to the study was thus 200. This study was approved by the Research and Ethics Committee of Kagoshima University Hospital and was carried out in accordance with the ethical principles stated in the 1975 Declaration of Helsinki. All patients provided written informed consent.
Measurements
Laboratory values were obtained at the time of admission before revascularization for CLTI. Levels of serum albumin, high-sensitivity C-reactive protein (hs-CRP), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), creatinine, and hemoglobin were measured, and the estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease equation with coefficients modified for Japanese patients as follows: eGFR (ml/min/1.73 m2) = 194 × serum creatinine (mg/dL)−1.094 × age (years)−0.287 (× 0.739 for female subjects). 15 In addition, left ventricular ejection fraction (LVEF) was obtained from echocardiography.
WIfI clinical stage, clinical frailty scale, and geriatric nutritional risk index
The WIfI classification system comprises three independent risk factors: wound, ischemia, and foot infection. 5 All three factors are individually graded on a scale from 0 (least severe) to 3 (most severe), then the three subscores are combined into a clinical risk score, ranging from stage 1 to stage 4 (1, very low risk; 2, low risk; 3, moderate risk; and 4, high risk) at the time of admission, as previously described. 5 Clinical frailty was also assessed at the time of admission by physicians according to the CFS derived from the Canadian Study of Health and Aging, ranging from 1 (very fit) to 9 (terminally ill). 10 Furthermore, we assessed nutritional status using the GNRI, calculated using the following equation: GNRI = 14.89 × serum albumin (g/dL) + 41.7 × (body weight/ideal body weight). 11 Body weight/ideal body weight was set to 1 when the body weight of the patient exceeded the ideal body weight. Ideal body weight was calculated based on a body mass index of 22 kg/m2. Body mass index was calculated as body weight in kilograms divided by height in meters squared.
Clinical outcomes
Clinical outcomes were retrospectively collected during follow-up. All-cause death was defined as any death after endovascular intervention. Cardiac death was defined as any death due to proximate cardiac death (myocardial infarction, heart failure, and fatal arrhythmia), and non-cardiac death was defined as any death not covered by the above definition.
The mortality after endovascular intervention was compared between a WIfI stage 1, 2 group (very low or low risk patients) and a WIfI stage 3, 4 group (moderate or high risk patients), and we then investigated the association between WIfI clinical stage and baseline characteristics, including CFS and GNRI.
Statistical analysis
Quantitative data are presented as mean ± standard deviation or median and interquartile range (IQR). Fisher’s exact test was used to compare the incidence of categorical variables, which were expressed as frequency and percentage. Continuous variables were compared between the WIfI stage 1, 2 group and the WIfI stage 3, 4 group using Student’s t-test (for values showing a normal distribution) or Mann–Whitney U test (for values showing a non-normal distribution). Cumulative survival rates for patients were estimated using a Kaplan–Meier curve evaluated by log-rank testing. Logistic regression analysis was used to analyze factors associated with WIfI stage 3 or 4, reporting odds ratios (ORs) and 95% confidence intervals (CIs). Furthermore, ordinal logistic regression analysis was also performed to analyze factors associated with WIfI clinical stage because WIfI clinical stage is an ordinal scale. Variables showing values of p < 0.05 on univariate analysis were entered into multivariate analysis. Values of p < 0.05 were considered to indicate statistical significance. Statistical analyses were performed using SAS software (JMP version 14.0).
Results
Baseline characteristics
Baseline patient characteristics.
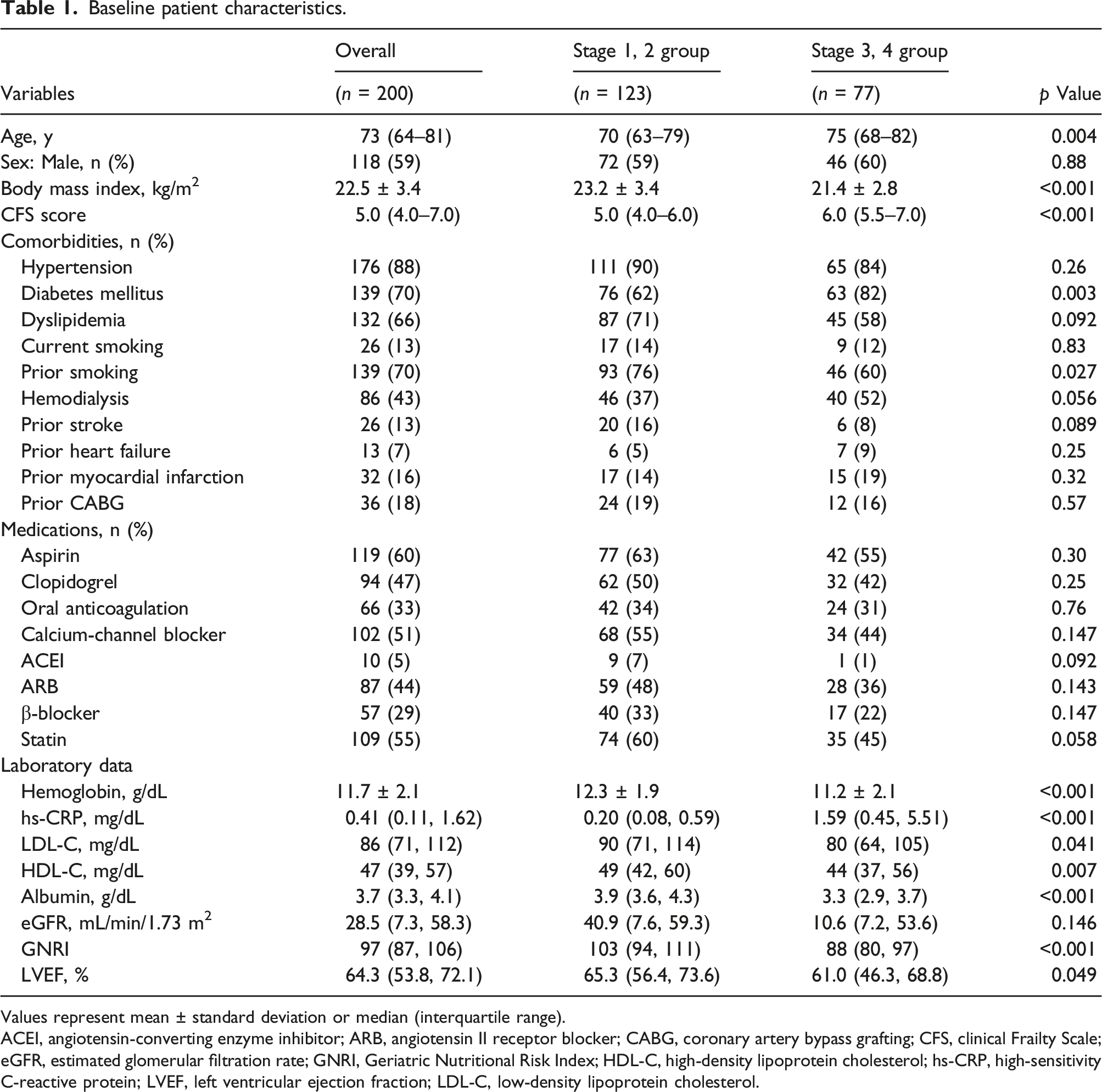
Values represent mean ± standard deviation or median (interquartile range).
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CABG, coronary artery bypass grafting; CFS, clinical Frailty Scale; eGFR, estimated glomerular filtration rate; GNRI, Geriatric Nutritional Risk Index; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; LDL-C, low-density lipoprotein cholesterol.
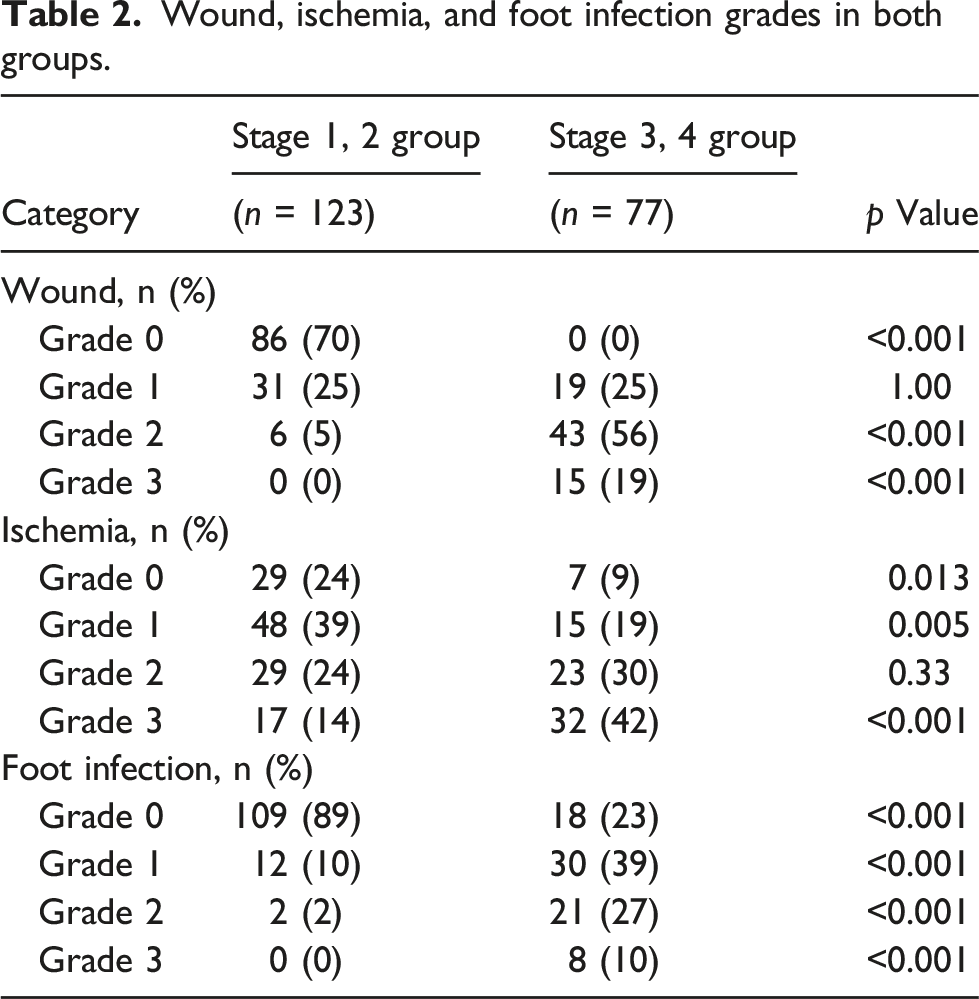
Wound, ischemia, and foot infection grades in both groups.
Mortality after endovascular intervention
Cumulative death after endovascular intervention.

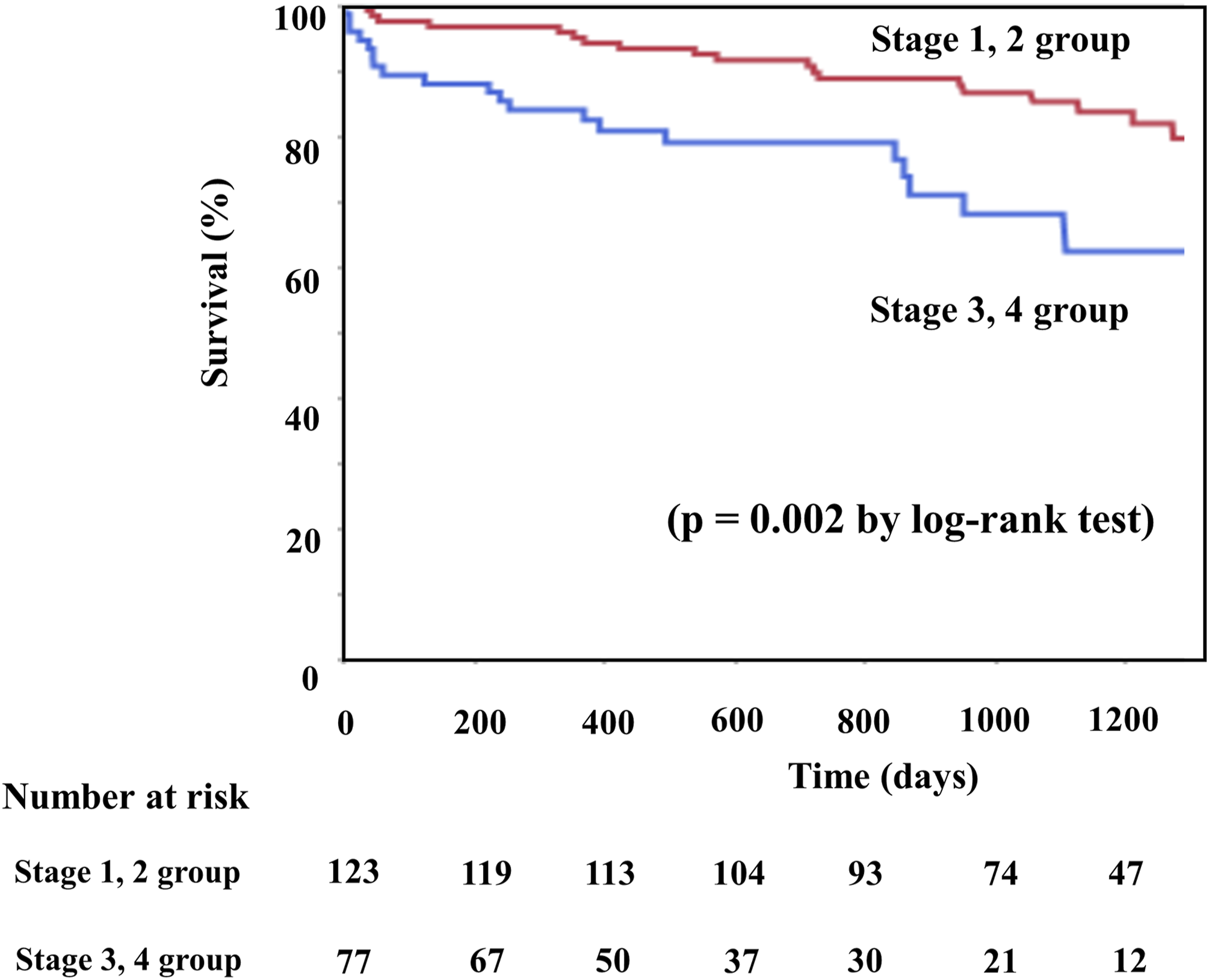
Kaplan-Meier analysis for survival rate after endovascular intervention.
Association of baseline systemic factors with WIfI clinical stage
Logistic regression analysis for WIfI clinical stage 3 or 4.
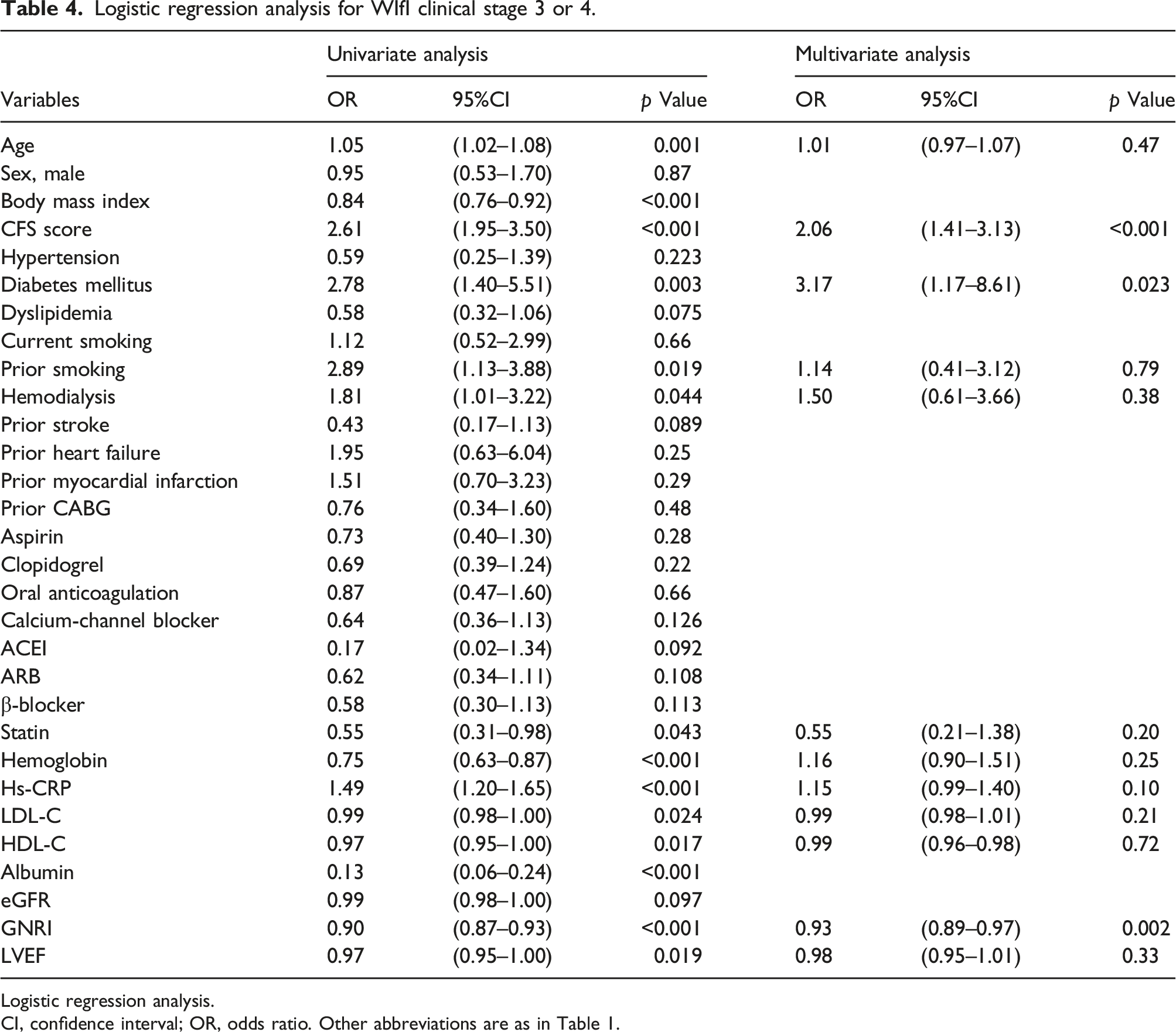
Logistic regression analysis.
CI, confidence interval; OR, odds ratio. Other abbreviations are as in Table 1.
Ordinal logistic regression analysis for WIfI clinical stage.
Discussion
The current study demonstrated that CFS score, diabetes mellitus, hs-CRP and GNRI were independently associated with WIfI clinical stage, and CLTI patients with WIfI clinical stage 3 or 4 showed a high frequency of all-cause death after endovascular intervention compared to those with WIfI stage 1 or 2.
The WIfI classification was introduced by the Society for Vascular Surgery Association. 5 Although WIfI classification was originally based on assessment of the 1-year risk of amputation in CLTI patients, 5 various studies have investigated the association between WIfI clinical stage and mortality in patients with CLTI.3,4,6,7,16 In those studies, inclusion criteria of subjects differed, such as non-diabetic patients 16 or medical therapy without revascularization. 7 However, the results consistently indicated a similar tendency, in that patients with high WIfI stage showed high mortality compared to those with low WIfI stage. The main causes of death in CLTI patients are cardiovascular and infectious disease such as pneumonia and sepsis.3,4,17 In our study, infectious disease and cardiac death were also main cause of death. In addition, the WIfI stage 3, 4 group had higher mortality after endovascular intervention compared with the WIfI stage 1, 2 group. These results are consistent with the aforementioned previous studies.
As mentioned above, WIfI clinical stage was associated with all-cause and cardiac deaths. Therefore, it is pivotal to clarify the clinical features relevant to WIfI clinical stage. We performed ordinal logistic regression analysis for WIfI clinical stage, and showed that with rises in WIfI clinical stage, CFS score rises and GNRI decreases. These results indicate that CLTI patients with high WIfI clinical stage have higher risks of frailty and malnutrition. Sarcopenia is the main cause of physical frailty and is influenced by nutritional status.18,19 Physical activity is decreased in CLTI patients with high WIfI stage due to severe wound and foot infection, and decreases in physical activity lead to reduced skeletal muscle and the risk of sarcopenia. Furthermore, lasting foot infection is more susceptible to progressive malnutrition. Consequently, CLTI patients with high WIfI stage may have a higher risk of frailty and malnutrition. Previous studies have revealed that CFS score was independently associated with 2-year overall survival in CLTI patients, 12 and that frailty as assessed by modified frailty index was associated with an increased risk of adverse cardiac events in patients with stable claudication. 20 Furthermore, GNRI was associated with overall survival after endovascular intervention in CLTI patients 13 and with overall survival and cardiovascular events in patients with peripheral artery disease. 21 Those previous studies support the results of this study that high WIfI clinical stage closely related to malnutrition and high frailty.
Diabetes mellitus and inflammation are widely known to be factors that promote atherosclerosis.22,23 In this study, diabetes mellites and hs-CRP significantly differed between WIfI stage 1, 2 and 3, 4 groups and were independent risk factors for WIfI clinical stage in multivariate ordinal logistics regression analysis. The association between hs-CRP and WIfI clinical grade is thought to be derived from differences in wound and foot infection grades, because the frequency of grade 2 or 3 wound and foot infection is higher in patients with high WIfI stage than in those with low WIfI stage. Another possibility should be considered, however. Atherosclerosis is a widely accepted inflammatory disease 23 and CRP is associated with an increased risk of future coronary heart disease. 24 CLTI is the most advanced form of peripheral artery disease, 1 and CRP has been independently associated with overall survival and cardiovascular events. 21 Furthermore, even in the general population, hs-CRP is associated with incident peripheral artery disease and CLTI. 25 Thus, elevated hs-CRP among patients with high WIfI stage in our study may have expressed a state of systemic atherosclerosis as a surrogate maker in addition to the severity of wound and foot infection. Diabetes mellitus is an established risk factor associated with the development of coronary artery26,27 and peripheral artery disease. 28 In addition, patients with diabetes mellitus are widely recognized to be at higher risk of amputation, 29 and diabetes mellitus is independently associated with cardiovascular events in CLTI patients. 21 This seems consistent with previous studies that diabetes mellitus correlates positively with WIfI clinical stage in this study.
A few limitations need to be considered for this study. First, the present study was a retrospective study, and WIfI clinical stage was assessed retrospectively using pretreatment photographs taken from multiple angles in some patients. Second, this study contained a relatively small number of patients, and the mortality rate after endovascular intervention was lower than that in the previous studies. We thus compared mortality between two groups (WIfI stage 1, 2 group and WIfI stage 3, 4 group). Third, while we were able to demonstrate a correlation between WIfI clinical stage and CFS score, the CFS is a semiquantitative scale of frailty, and we were unable to investigate the relationship between mortality and other frailty factors such as muscular strength.
Conclusion
The current study demonstrated that WIfI clinical stage correlated independently with CFS score and GNRI, and CLTI patients with WIfI clinical stage 3 or 4 had a high mortality after endovascular intervention compared to those with WIfI stage 1 or 2. This study suggests that CLTI patients with high WIfI clinical stage may be more frail and malnourished, and be associated with poor prognosis after endovascular intervention.
Footnotes
Acknowledgments
We thank the staff of the Department of Cardiovascular Medicine and Hypertension at the Graduate School of Medical and Dental Sciences, Kagoshima University for their assistance with data processing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Japan Society for the Promotion of Science KAKENHI (grant no. 16H070890).