
Abstract
Purpose
The present study aimed to determine the safety and efficacy of a drug-coated balloon inflated within a thin-strut self-expanding bare-metal stent in patients with severe and complex femoropopliteal occlusive disease.
Methods
This prospective study used the Pulsar-self-expanding stent and Passeo-18 Lux drug-coated balloon in patients with severe and complex femoropopliteal occlusive disease. The primary endpoint was the 12-month primary patency, and the secondary endpoints included 24-month primary patency, assisted primary patency, secondary patency, and clinically associated target lesion revascularisation.
Results
The study included 44 patients (51 limbs). The mean age of the patients was 67.6 ± 10.2 years, with 73% men. Chronic limb severity was classified as Rutherford Category III in 41% of the patients, stage IV in 31%, and stage V in 27%. Lesions were predominantly Trans-Atlantic Inter-Society Consensus (TASC 2007) D (51%) and C (45%), with 32 (63%) chronic total occlusions. Procedural success was obtained in all cases. The mean lesion length was 200 ± 74.55 mm (95% CI = 167.09–208.01) with a mean number of stents per limb used of 1.57 ± 0.70 (95% CI = 1.37–1.76). Distal embolisation occurred in two patients. The primary patency rates at the 12- and 24-month follow-up were 94% (95% CI = 82.9–98.1) and 88% (95% CI = 75.7–94.5), respectively. The assisted primary was 94% (95% CI = 82.9–98.1) and secondary patency was 96% (95% CI = 85.2–99.0) at 24-month follow-up. The cumulative stent fracture rate at the 24-month follow-up was 10%. Freedom from clinically driven target lesion revascularisation was 94% (95% CI = 83–98%) at 12-month follow-up and 88% (95% CI = 76–94%) at 24-month follow-up, with two patients requiring a bypass graft.
Conclusion
Our novel approach involving the combination of a thin-strut bare-metal stent and a drug-coated balloon may be safe and effective, with sustainable and promising clinical outcomes up to 24 months after treatment.
Introduction
There have been significant advancements in endovascular management options for atherosclerotic femoropopliteal disease over the last decade. 1 Maintenance of luminal patency might be challenged by negative vascular remodelling resulting from neointimal hyperplasia. 2 Percutaneous transluminal balloon angioplasty (PTA) alone has been shown to be associated with high restenosis rates. 3 The early elastic recoil and late lumen loss (LLL) associated with PTA have been treated effectively with self-expanding nitinol bare-metal stents (BMSs). 4
It is well described that PTA may damage the intima, particularly in complex Trans-Atlantic Inter-Society Consensus (TASC 2007) C and D lesions, often resulting in stent implantation. 5 A well-documented issue of stenting is a high rate of restenosis, as it can induce a foreign body reaction, leading to neointimal proliferation and in-stent stenosis.6,7
However, successful use of drug-eluting technology in coronary intervention has led to the implementation of drug-eluting stents (DESs) and drug-coated balloons (DCBs) for infrainguinal vessels. DESs provide sustained release of an antiproliferative medication such as paclitaxel (most commonly used in peripheral stents) into the arterial wall.8–11 However, for use in longer femoropopliteal lesions (≥120 cm), it requires multiple overlapping stents for adequate covering of the disease segment, that may result in-stent restenosis and fracture/dislodgement due to the continuous dynamic stresses.12,13 Conversely, DCBs allow rapid, homogenous delivery of an anti-proliferative drug to the vessel wall without leaving prosthetic material in the vessel.14–17 The 12-month primary patency has been shown to be superior and freedom from target lesion revascularisation (TLR) has been shown to be better with DCBs than with PTA.18,19 Ideally, a DCB should have minimal drug loss during insertion, tracking and inflation. A limited number of DCB trials have investigated relatively short lesions, with an average stent length of 70 mm.14,15 As such, a DCB alone may be insufficient for complex, calcified lesions and offers no scaffolding or resistance to early elastic recoil and LLL due to negative remodelling. BMSs have been shown to be ideal for adjunctive use.20–26 Coronary studies have found that the use of a thin-strut device could significantly reduce the angiographic and clinical restenosis rates after stenting.27,28
The present study aimed to determine the safety and efficacy of a DCB inflated within a thin-strut self-expanding BMS in patients with severe and complex femoropopliteal occlusive disease.
Methodology
Study design
DEBAS inclusion and exclusion criteria.
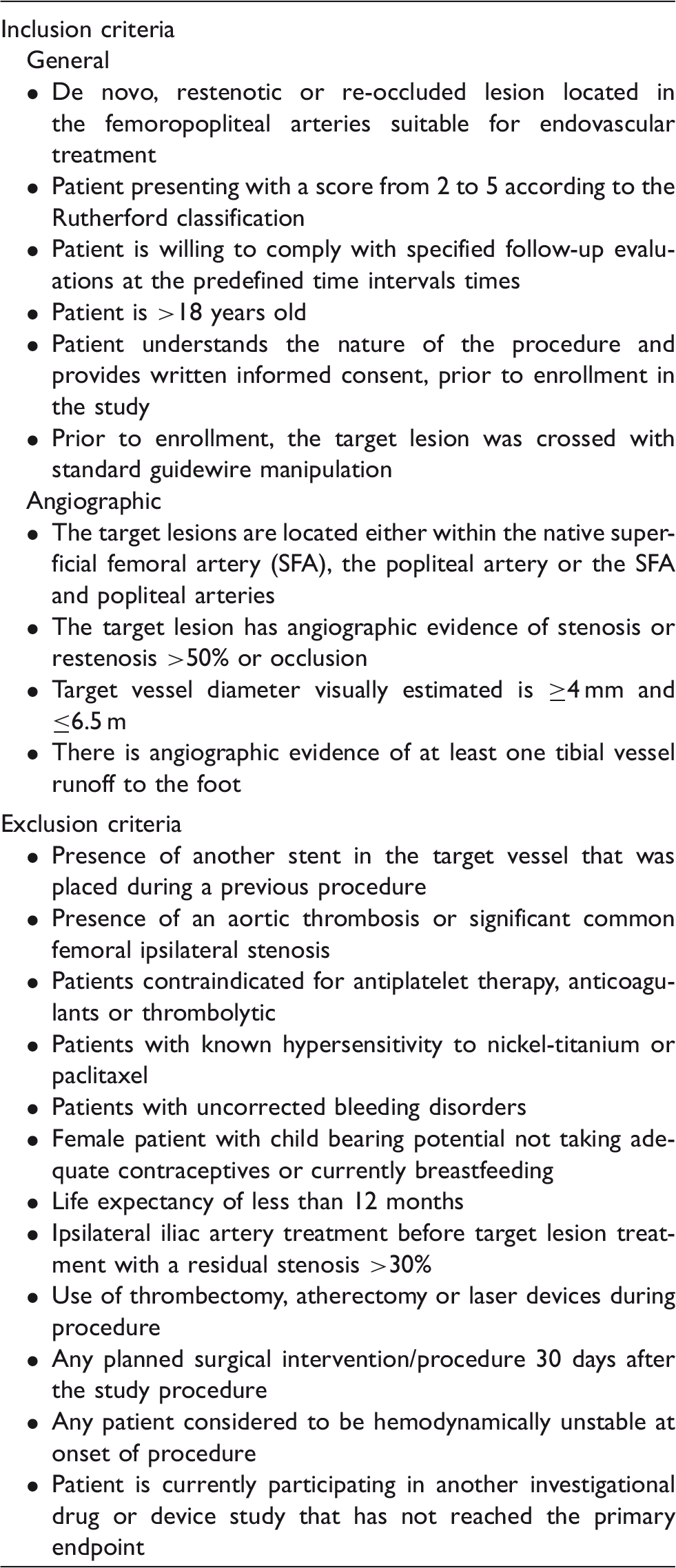
The treatment rationale was that in complex TASC C and D lesions, angioplasty alone would damage the intima, causing flow-limiting dissections often requiring stent implantation. Stent placement in long lesions has been associated with high rates of restenosis. However, inflating a DCB within the stent will ensure that the barotrauma is evenly spread across the stented length without substantially impeding drug transfer. The rationale for the use of thin-strut stents was that these stents decrease the distance between the DCB and the vessel wall owing to the low metal-to-artery ratio. This geometric principle of thin-struts reducing distance between drug coating and wall is independent of stent type or stent material. When the DCB is inflated within the stent, the scoring effect can cause plaque surface modification and may allow enhanced paclitaxel transfer, especially in calcified lesions.
Procedure
Vascular access was achieved using a 6F 45-cm Fortress sheath (Biotronik AG) for contralateral access and a 6F 11-cm Brite Tip® sheath (Cordis Corp., Miami, FL) for ipsilateral access. All inflow-limiting lesions were treated prior with either bare metal or covered stents.
It was mandatory for the guide-wire to cross the entire lesion before enrolment of the patient in the study. If several attempts at re-entry into the distal true lumen were unsuccessful using an antegrade approach, retrograde tibial (anterior tibial artery or posterior tibial artery) access was secured. This was achieved under direct ultrasound guidance using a micropuncture kit for placing a 4F sheath (Cook Medical, Bloomington, IN). According to the clinician’s discretion, the lesion could be treated with either direct primary stenting or predilation with a PTA balloon followed by BMS implantation. This was followed by the application of a DCB to the entire stented segment, extending 1 mm beyond the ends of the implanted stent, for a minimum of 90–120 s.
Systemic heparin was administered intravenously at 80–100 IU/kg prior to either PTA or stenting of the lesion. The study protocol mandated that patients subsequently commence clopidogrel (75 mg/day) for at least six months and lifelong aspirin (100–150 mg/day). Immediately after the procedure, a physical examination and ankle brachial index (ABI) assessment were performed. All complications and adverse events were recorded, along with the medications prescribed and the Rutherford Category at discharge.
Follow-up
Follow-up evaluations were mandated on day 1 and at 1, 6, 12, 18 and 24 months after the procedure. At each follow-up, a physical examination, ABI assessment, duplex ultrasound of the treated vessel and biplanar radiography were performed. For adequate interpretation of the biplanar radiographs, separate images were obtained for each stent in two planes, with maximal opacification and zoom. If there was evidence of restenosis, either computed tomography angiography or conventional angiography was performed to confirm the non-invasive findings.
Study devices
The Pulsar stent mounted on the Pulsar-18 or Pulsar-35 system is a self-expanding nitinol stent deployed using either a 4F (Pulsar-18) or 6F (Pulsar-35) introducer sheath. The Pulsar stent has a thin-strut design with high multi-axial flexibility that provides an optimised chronic outward force. This stent is available in different lengths (20, 40, 60, 80, 100, 120, 150, 170 and 200 mm) and diameters (4, 5, 6 and 7 mm). Standard PTA techniques were followed for balloon dilation before and after stent deployment.
The Passeo-18 Lux paclitaxel-coated balloon is available in diameters of 2–7 mm and lengths of 40–120 mm. Its design is based on that of the Passeo-18 uncoated balloon catheter, and it has a balloon coating containing a matrix of anti-proliferative paclitaxel and butyryl-trihexyl citrate, which is a biocompatible excipient for enabling optimal drug transfer to the target lesion tissue. The Passeo-18 Lux balloon also has a unique safeguard, which improves ease of handling and protects the user and balloon coating from contact and damage. After insertion into the introducer sheath, the safeguard can simply be peeled away.
Definitions and outcomes
The primary endpoint was 12-month primary patency defined as absence of >50% restenosis with an increase in the peak systolic velocity ratio (PSVR) ≥2.5 and no clinically associated re-intervention at the stented segment, within 5 mm of each side of the stented area.
The secondary endpoints were (1) technical success defined as the ability to cross and stent the lesion, and achieve angiographic residual stenosis <30% and residual stenosis <50% on duplex imaging; (2) sustained clinical success in follow-up defined as an improvement in the Rutherford Category by ≥1 level compared to the stage before the procedure, at the 6-, 12- and 24-month follow-up; (3) number and type of stent fractures at the 12- and 24-month follow-ups; (4) assisted primary patency and secondary patency at 12- and 24-month follow-up; (5) freedom from major adverse events at the 12- and 24-month follow-up; (6) freedom from TLR and target vessel revascularisation at 12- and 24-month follow-up; (7) freedom from major target limb amputation and death at the 12- and 24-month follow-up; and (8) secondary patency at 12- and 24-month follow-up.
Statistical analysis
Primary analysis of all baseline characteristics and study outcomes was based on the available data from all enrolled participants, unless otherwise indicated. Continuous data are presented as mean ± standard deviation (95% confidence interval (CI)) or median with interquartile range (IQR). Categorical data are presented as the number of patients and percentage. TASC (2007) II classification was used in this study. A patient with more than one event was counted only once towards the event rate based on the total number of participants with adverse events. Sub-group differences in rates of patency at 24 months were investigated using logistic regression. Kaplan–Meier analysis was used to evaluate time-to-event data, including the primary effectiveness endpoint. Further analysis was performed according to lesion length (lesion length <120 mm vs. lesion length ≥120 mm) and severity of calcification (mild or moderate vs. severe vessel calcification). When two legs from the same patient were enrolled in the study, it was necessary to recognise that the vessels were genetically identical and therefore the outcomes could be correlated. All analyses were therefore adjusted for potential intra-cluster correlation, using robust sandwich variance estimates, originally developed by Huber and White and later extended by Lin and Wei 29 to produce the adjusted log-rank P-value and perform the survival analyses.
All hypotheses tests were performed using two-sided tests, and the critical value for statistical significance was set at a value of p < 0.05. All analyses were performed using PASW 22 (SPSS, Chicago, IL), SAS 9.4 (SAS Institute, Inc., Cary, NC) and Stata 14 (StataCorp LP, College Station, TX) statistical software.
Results
Patient characteristics
Demographic, comorbidities and clinical characteristics of 44 patients at Baseline.
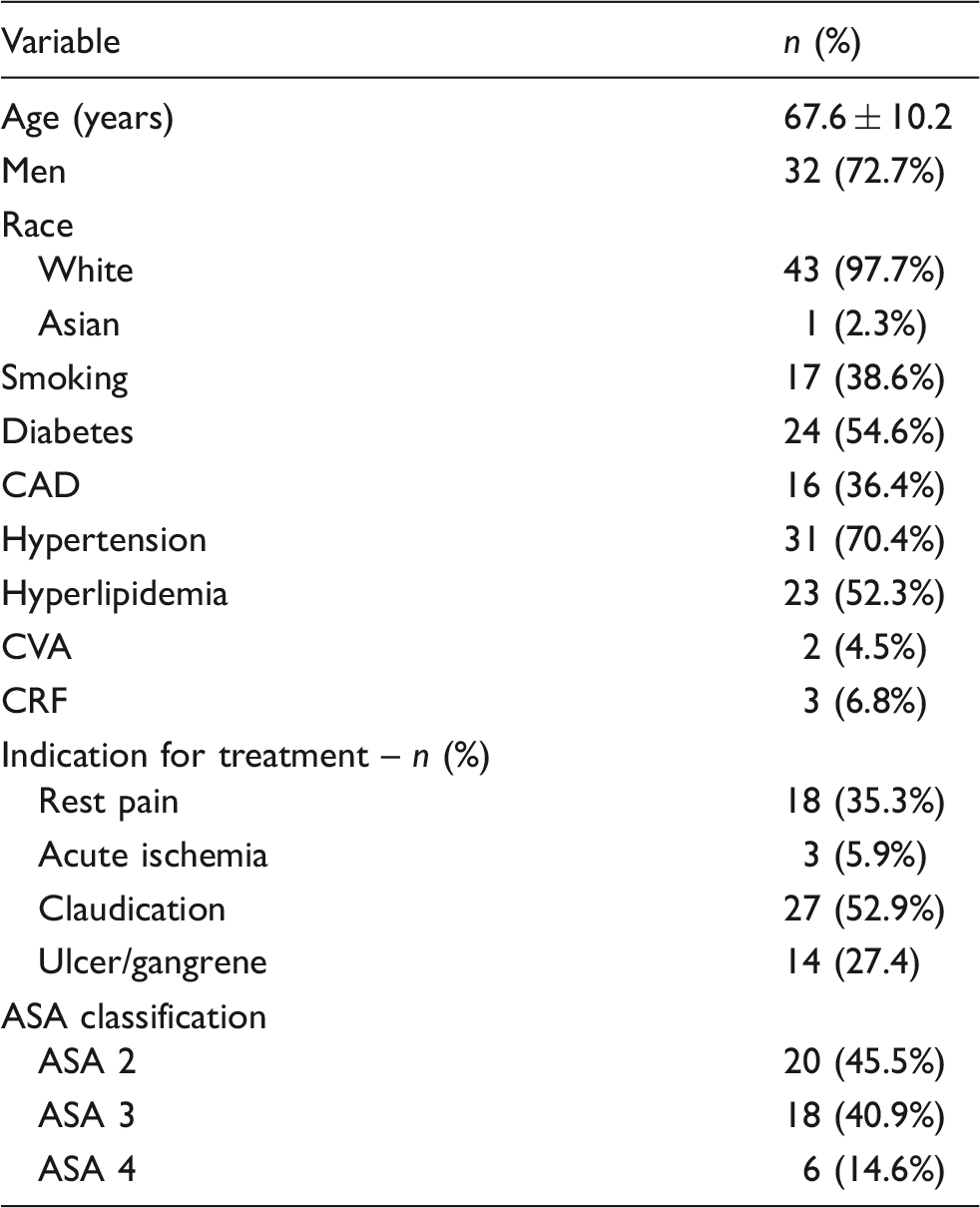
CAD: coronary artery disease; CVA: cerebral vascular disease; CRF: chronic renal failure; ASA: American Society of Anesthesiologists.
Note: Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Lesion and clinical characteristics at baseline.
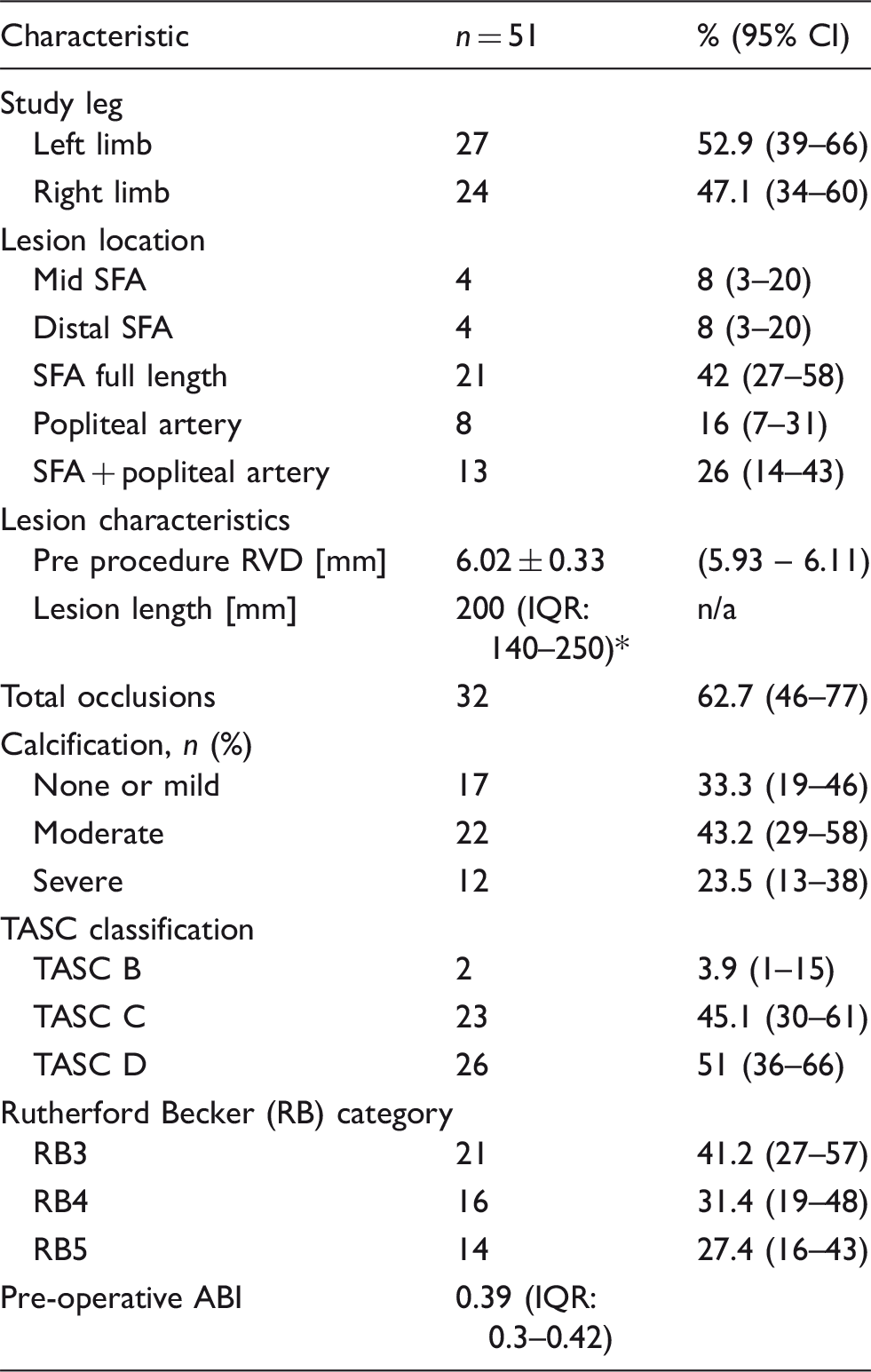
n: number of limbs; IQR: interquartile range; SFA: superficial femoral artery; RVD: reference vessel diameter; TASC: trans-Atlantic inter-society consensus; ABI: ankle brachial index; n/a: non-applicable.
Note: Continuous data are presented as the means ± standard deviation or median (interquartile range); categorical data are given as the counts (percentage).
Procedural results
Baseline angiographic and interventional data.
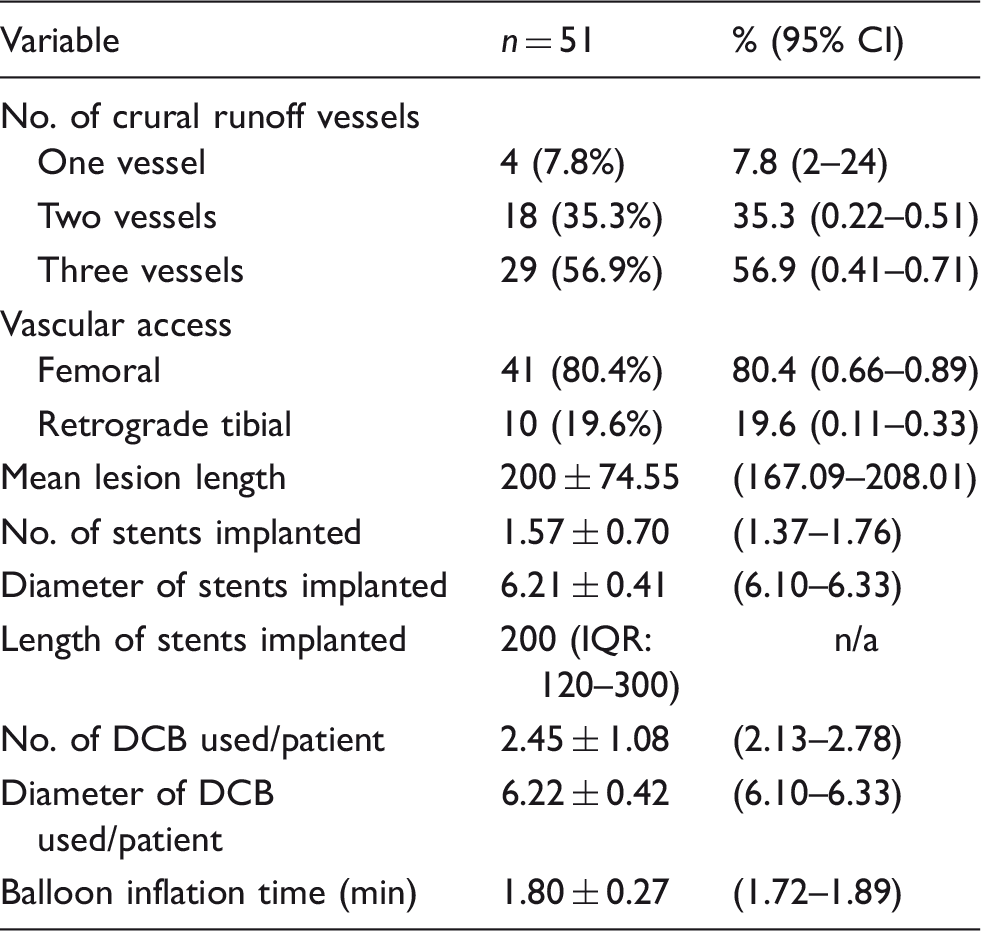
DCB: drug coated balloon; n: number of limbs; IQR: interquartile range.
Note: Continuous data are presented as the means ± standard deviation or median (interquartile range); categorical data are given as the counts (percentage).
Primary endpoint
The primary patency rates at the 12 and 24-month follow-up were 94% (95% CI = 82.9–98.1) and 88% (95% CI = 75.7–94.5), respectively (Figure 1(a)). Logistic regression analyses according to lesion length demonstrate that there was no statistical difference between the two groups of patients (OR = 2.5; 95% CI = 0.29–21.24; p = 0.40).
Kaplan–Meir curves representing primary patency (a), assisted primary patency (b) and secondary patency (c). Curve shows patency up to 24 months after combined stenting and drug-coated balloon angioplasty. The grey shadow indicates 95% confidence interval. Standard error did not exceed 10% at any time of follow-up. Figure 1(a) and (b) are courtesy of BIOTRONIK AG.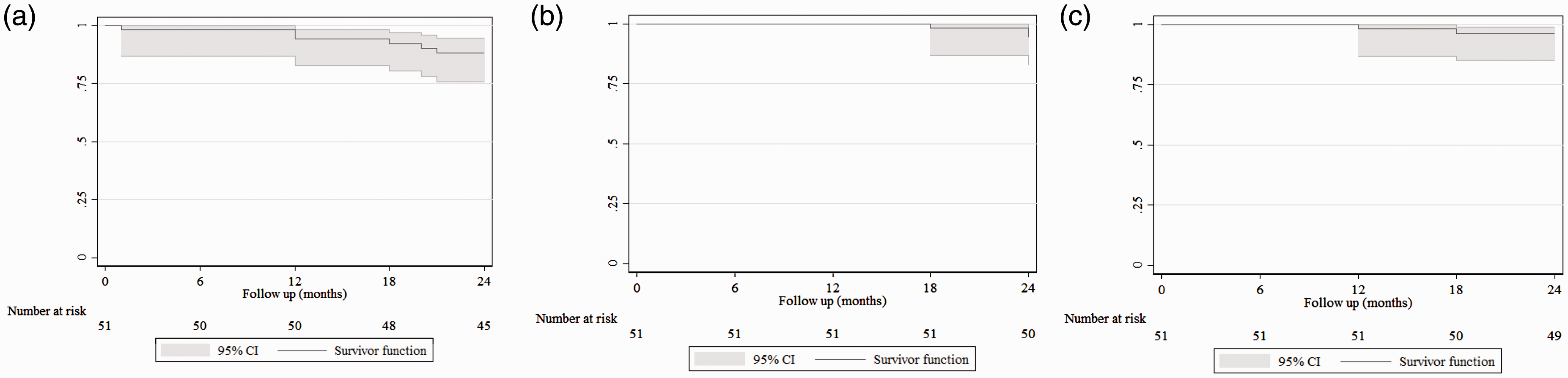
Secondary endpoints
Freedom from clinically driven TLR (Figure 2) was 94% (95% CI = 83–98%) at 12-month follow-up and 88% (95% CI = 76–94%) at 24-month follow-up, with two patients requiring a bypass graft, and the rate of freedom from cumulative major amputation was 98% (Table 5). Analysis of freedom from TLR according to lesion length was 94% (95% CI = 63–99%) for lesions less than 120 mm length versus 86% (95% CI = 69–94%) for lesions ≥120 mm length at 24-month follow-up and this was not statistically significant (P = 0.44). The stent fracture rate at the 12-month follow-up was only 2%, and the cumulative stent fracture rate at the 24-month follow-up was 10% (Table 5). Type I stent fracture occurred in one patient at the 12-month follow-up, type II stent fracture occurred in three patients at the 18-month follow-up and type III stent fracture occurred in one patient at the 24-month follow-up. Only the type III stent fracture was associated with restenosis that required re-intervention.
Kaplan–Meier curve representing freedom from revascularisation (TLR. Curve shows freedom from TLR up to 24 months follow-up. The grey shadow indicates 95% confidence interval. Standard error did not exceed 10% at any time of follow-up. Two-years clinical and outcome safety data. CD-TLR: clinically driven target lesion revascularisation. Stent fracture was confirmed on plain X-ray screening of the implanted stents. Type I stent fracture. Type II stent fracture. Type III stent fracture.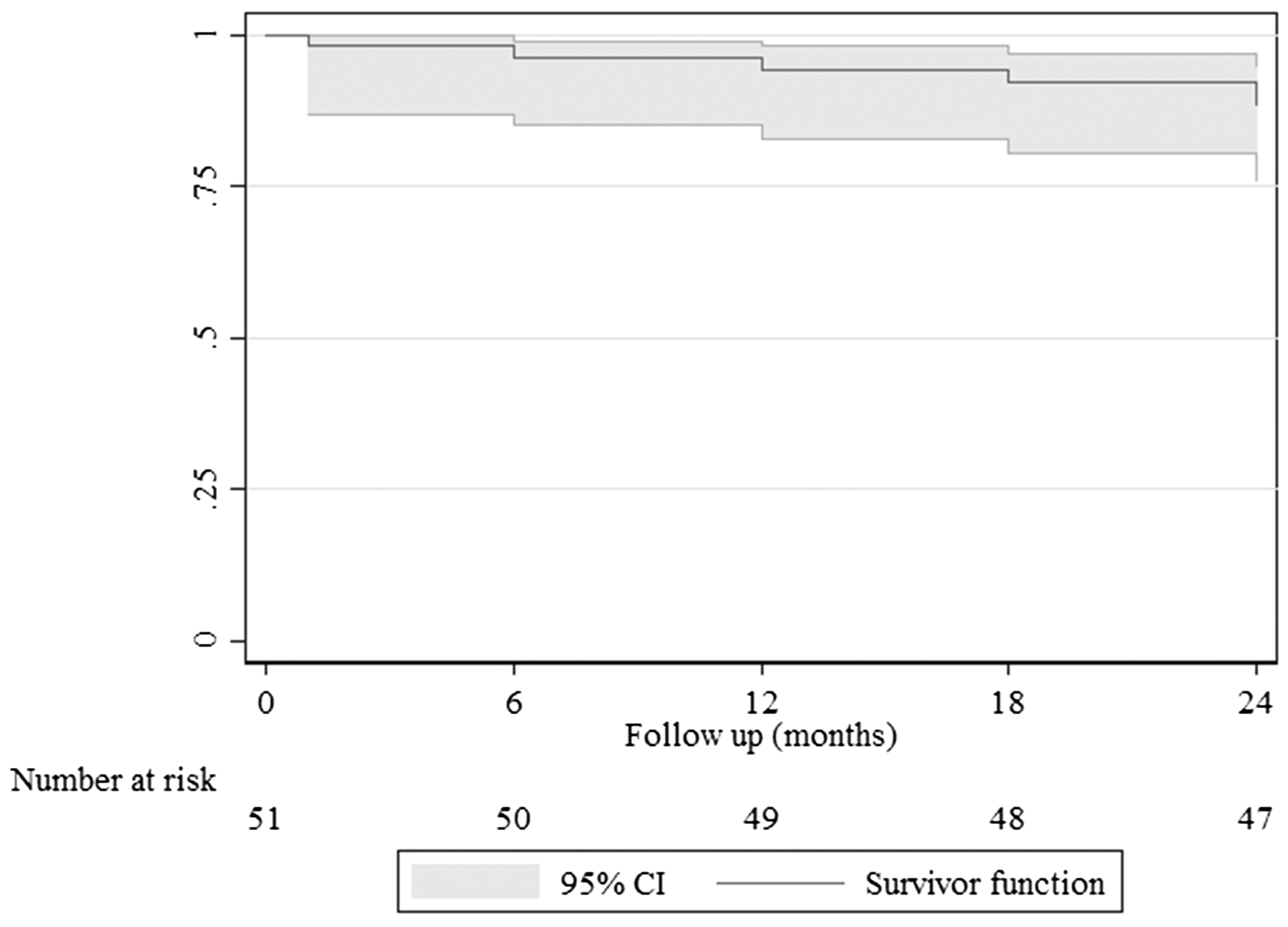

The assisted primary patency rates (Figure 1(b)), at the 12- and 24-month follow-up were 98% (95% CI = 86.9–99.7) and 94% (95% CI = 82.9–98.1), respectively, and the secondary patency rates at the 12- and 24-month follow-up were 100% (95% CI = 86.9–100) and 96% (95% CI = 85.2–99.0), respectively (Figure 1(c)). The mean ABI improved immediately after treatment (with mean ABI at baseline was 0.39 ± 0.02, 95% CI = 0.36–0.42) and improvement was sustained up to 24-month follow up (mean ABI was 1.06 ± 0.02, 95% CI = 1.02–1.09). There was a satisfactory improvement among the patients, with 76% of the patients at the 12-month follow-up and 86% of the patients at the 24-month follow-up showing clinical improvement to Rutherford Category 0/I.
Procedure-related complications were identified in five patients (10%). Of the five patients, two had distal embolisation in the peroneal arteries that was managed conservatively, one had retroperitoneal bleeding requiring surgery, one had a false aneurysm requiring thrombin injection, and one had a haematoma that did not require any treatment or blood product transfusion. The overall median length of hospital stay was 2 days (IQR: 2–3).
Discussion
Our results suggest that the hybrid approach of DCB inflation following BMS implantation is safe, with good mid-term clinical results at 24 months after the procedure. Complex TASC C and D lesions were found to have a good primary patency at 24 months after the procedure. The improved mid-term luminal patency translated into low rates of TLR and amputations. The health care costs with this hybrid approach might be lower than the costs with the BMS only approach reported previously owing to the lower TLR rates with the hybrid approach than with the BMS only approach.
Scheinert et al. 30 performed an international multicentre randomised control trial (BIOLUX P-1) to investigate the safety and efficacy of the Passeo-18 Lux DCB, which was used in our series. The authors found that the 6-month rates of TLR and binary restenosis were lower with this approach than with PTA, and these findings are comparable to the findings in our study. However, at the 12-month follow-up, the TLR rate was 16% in the as-treated population in this previous study, a rate four times higher than that observed in the present study. Furthermore, 57% of the cases developed post-procedure vessel dissections in the BIOLUX P-I study. It is unclear whether these outcomes were clinically significant; however, a BMS scaffold might help avoid such negative outcomes.
Multiple studies have compared DCB with PTA (LEVANT-1, THUNDER Pacifier, FemPac and BIOLUX P-116,30–32); however, most of these studies appear to be limited by the relatively short lesion length (57–81 mm). The authors of the previous studies might have been reluctant to randomise patients with longer lesions owing to the perceived inadequacy of dilation alone. The platform provided by the BMS in our series allowed for uniform application of paclitaxel along a reasonably long lesion.
In the Drug-Eluting Balloon in Peripheral Intervention for the Superficial Femoral Artery (DEBATE-SFA) trial, Liistro et al. 17 randomised 104 patients presenting with critical limb ischaemia or claudication to either a drug-eluting balloon (DEB) and BMS group or a PTA and BMS group. 17 All lesions underwent predilation with an uncoated balloon, and thereafter, the DEB and BMS group underwent further dilation with a paclitaxel-coated balloon (In.Pact Admiral, Invatec/Medtronic, Santa Rosa, CA) and subsequently received a self-expanding nitinol stent (Maris, Invatec/Medtronic). At the 12-month follow-up, the rate of freedom from TLR was 83.0%, which is lower than the rate noted in the present study. DCB inflation without stent presence may cause irregular distribution of paclitaxel. We used a thin-strut Pulsar-18 stent; however, Liistro et al. used the Maris stent (Invatec/Medtronic), which has slightly thicker struts, and this might have inhibited drug delivery to the arterial wall owing to the small paclitaxel footprint at the lesion and vessel wall.
Previous coronary studies found that the use of a thin-strut device was responsible for a significant reduction in angiographic and clinical restenosis rates after stenting.27,28 This concept has generated interest in combining DCB with thin-strut stents in order to reduce the distance between the drug coating and the vessel wall, with a well-established reduction of barotrauma on the vessel wall.
We did not find any difference in the primary patency rates between patients with lesions ≥120 mm in length and those with lesions <120 mm in length that is comparable to the findings of the VIPER study. 33 The VIPER study was a single-arm study of 119 patients with long SFA lesions (mean length = 19 cm), and 56% of the lesions had chronic total occlusions and 61.0% had moderate-to-severe calcification. In this previous study, the GORE® Viabahn® endoprosthesis (WL Gore & Associates, Inc., Flagstaff, AZ) with a heparin bioactive surface exhibited 73% primary patency in long SFA lesions. Additionally, the patency rate was independent of lesion length, with equivalent results for long lesions (>20 cm) and medium lesions (5–20 cm) at 1 year. The VIASTAR study compared the GORE® Viabahn® endoprosthesis to a BMS for the treatment of complex, long lesions and noted similar results. 34
Similar to our study, the BIOLUX 4EVER trial, currently at early phase, is evaluating the combination of a Pulsar-18 stent and Passeo-18 Lux Balloon in a multicentre, international study. However, in contrast to our practice of inflating the DCB within the BMS, the authors of this trial are attempting to initially treat the lesion with a DCB, followed by BMS implantation. It will be interesting to note the differences in the results between these two treatment strategies.
Limitations
This study included a very small study sample. Therefore, selection bias may exist and may have affected the conclusion and restricted the achievement of robust results. However, this is the first time this combination of therapeutic modalities has been used in complex femoropopliteal lesions (long lesions with or without major calcification). Type II error may occur due to the small sample size. The outcome of this study would have been boosted if it were compared with DCB angioplasty and bail out spot stenting; however, this constitutes complicatedly a different study that our institution will pursue in the near future.
Conclusion
Our novel approach involving the combination of a thin-strut BMS and a DCB may be safe and effective, with sustainable and promising clinical outcomes up to 24 months after treatment. This approach may be considered as a part of routine practice mainly in patients with complex and long occlusive lesions.
Footnotes
Acknowledgements
Figure 1(a) and 1(![]() ) are courtesy of BIOTRONIK AG.
) are courtesy of BIOTRONIK AG.
Patient consent
Patient understands the nature of the procedure and provides written informed consent, prior to enrollment in the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Mwipatayi has received research support from Biotronik AG.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.