
Abstract
Here we present three cases performed using a novel technique where aortic flow is compartmentalized proximal to the target vessels through a physician-modified endograft. The visceral segment is then further compartmentalized by the use of another physician modified endograft. By compartmentalizing the flow proximal to the visceral segment, both the true lumen and false lumen can be used as conduits for coextensive bridging stent grafts. Overall, patients have tolerated this procedure extremely well, and while further study and follow-up must be conducted, this procedure could offer a reasonable long-term solution to thoracoabdominal aortic aneurysms complicated by dissection.
Introduction
Thoracoabdominal aortic aneurysms (TAAA) complicated by chronic type B dissection with branch arteries coming from both the true and false lumen leave patients with very limited options for repair. Small true lumens and visceral arteries arising from either true or false lumen and dissection extending to branches have made endovascular repair sometimes near impossible. Here we describe how a new stent graft configuration and associated procedure that can be used to repair dissections.
Methods
This procedure makes use of a thoracic bifurcation and visceral manifold deployed in the descending thoracic aorta as described before. 1 After explaining the risks, complications, and benefits of surgery with a modified endograft and the challenges of repairing aneurysms complicated by dissection, informed consent was obtained.
Patient 1 was a 68-year-old man who had previously undergone open surgery to repair the thoracic and infrarenal aorta at another center. With his previous TAAA incision, he was left with a paralyzed left diaphragm and left flank diastasis and chronic pain. Through the visceral segment, the true lumen was significantly compressed. From the groin, we delivered our thoracic bifurcation and visceral manifold. They were deployed so that the most distal limbs of the visceral manifold were 2 cm proximal to the celiac artery. We then perforated the septum of the dissection at about the level of the celiac artery using a guide wire and dilated the septum with a 12-mm and 20-mm balloon creating a “neo fenestration.” We directed our wire into the descending aorta from the arm. We selected one of the limbs of the visceral manifold. Positioning the wire and sheath through the false lumen, we selected the right renal and then placed two iCasts. They were lined with self-expanding (SE) Protégés. Once back in true lumen, the process was repeated for the other visceral vessels. We went back to the groin where we had the wire that went from the distal true lumen to the false lumen aneurysm and back into the proximal true lumen. We extended the thoracic bifurcation to the previously placed infrarenal graft with an Endurant extension limbs (Figure 1(a)).
Drawing of the stent graft configuration including main body components and bridging stent components for (a) Patient 1, (b) Patient 2, and (c) Patient 3.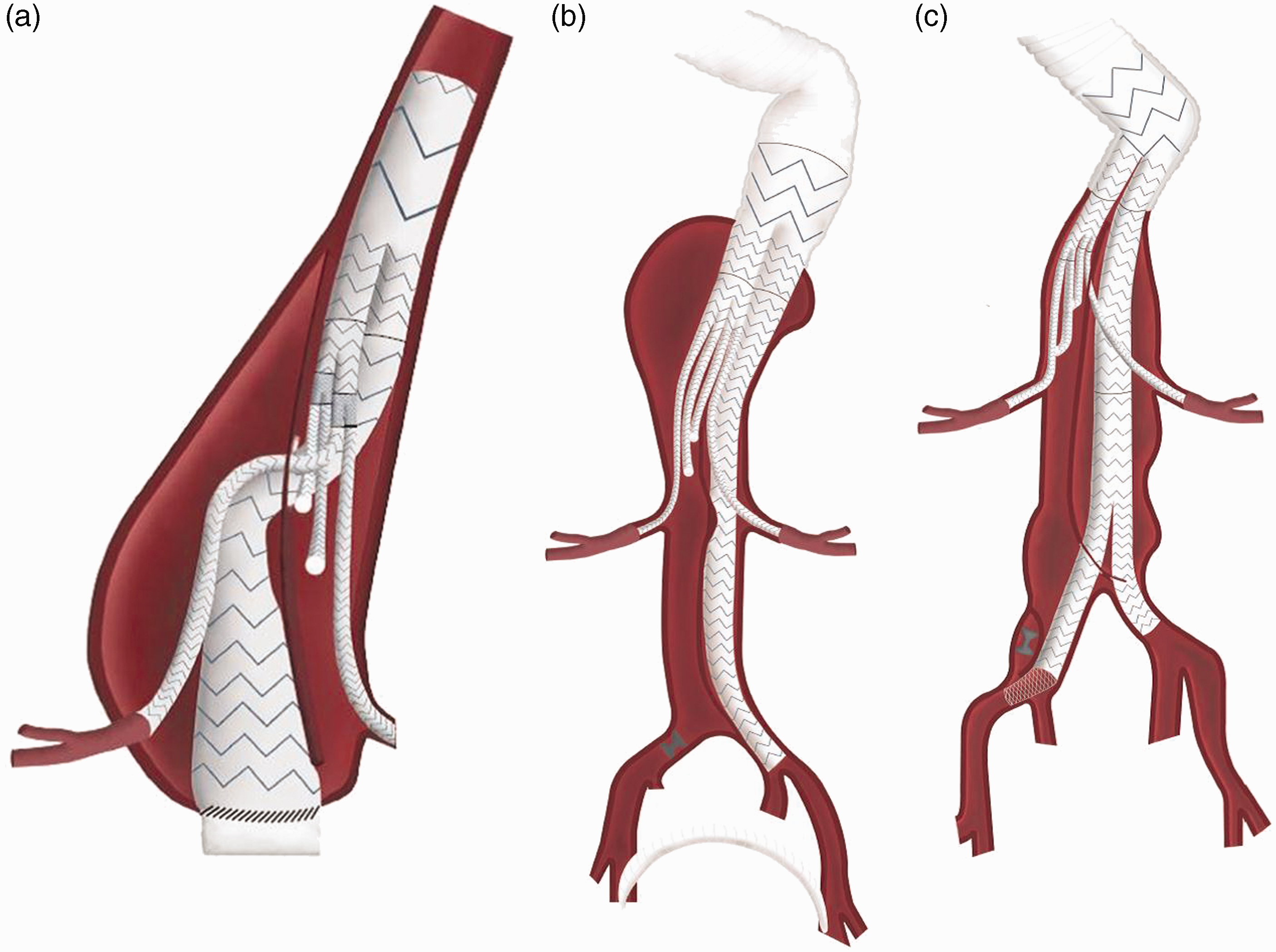
Patient 2 was a 70-year-old gentleman who previously underwent open repair of the ascending and descending aorta, though unfortunately he was left with a type B dissection in the visceral segment. Unfortunately, the left renal came off false lumen while the right renal, celiac, and superior mesenteric artery (SMA) came off true lumen. He also had a splenic artery aneurysm. The left common iliac was fed off of false lumen while the right common iliac was fed off true lumen. We first put up the thoracic bifurcation and landed it in the previously placed Dacron graft. We then put up the visceral manifold. From here, we advanced a sheath in the left subclavian over the through wire where we selected one of the longer legs of the visceral manifold. We were able to select the left renal by passing a wire within the false lumen. We stented to the right renal, SMA, and celiac through the true lumen. We stented the celiac from the common hepatic back to the visceral manifold to exclude the previously mentioned splenic and proximal celiac aneurysm. Then from the left groin, we selected the contralateral limb of the thoracic bifurcation. We extended this down sealing in the left common iliac with an aorto uni-iliac stent graft. We completed this case with a fem-fem bypass from left to right (Figure 1(b)).
Patient 3 was a 64-year-old woman who had undergone previous open surgical repair of an ascending aortic dissection with valve replacement. She also had previously undergone open repair of the descending thoracic aorta. She was found to have a multi-lumen dissection with the left renal artery coming off false lumen. The right renal, celiac, and SMA all came off a very small true lumen. The internal iliacs came off both true and false lumen bilaterally. After placing the thoracic bifurcation and visceral manifold, we selected a limb of the manifold. With a 0.9-mm laser, we fenestrated the septum between the true and false lumen. With catheter direction, we were able to select the left renal artery. After dilating this tract, we placed the iCast bridging stents and lined them with self-expanding Medtronic SEs. A similar process was repeated for the right renal, celiac, and SMA through the true lumen. We then went back to the groin to access the true lumen. We again used the laser to enter the false lumen. The track was dilated. We extended the limb of the thoracic bifurcation with an Endurant limb and a bifurcated Endurant. We then captured the contralateral gate and sealed in the right common iliac. There was a chronic dissection plane that created a false lumen into the right common iliac artery. We coil embolized the false lumen and then we covered the intimal tear with a Protégé which allowed for continued flow to the internal iliac artery (Figure 1(c)).
Results
Patient 1 had a relatively uneventful recovery other than a c-diff infection which was believed to have not been fully cleared from a previous infection. He was in the hospital for four days total. He is currently 19 months out. He has not had any noteworthy complications, and he has seen some remodeling of the aneurysm sac. The patient has since returned to his occupation as a farmer and is doing quite well.
Patient 2 was seen back six weeks post operatively. Unfortunately, he appeared pale in appearance with generalized weakness and fatigue. We discovered that he had a proximal hepatic artery aneurysm with dissection through the SMA and the celiac. We admitted him the next day and performed a mesenteric angiogram. We placed a Protégé stent in the SMA and did not angioplasty for fear of extending the dissection. We then gained access to the celiac artery but were unable to advance the wire into the hepatic artery because of the dissection. An Amplatz plug was used to embolize the proximal hepatic artery and the celiac limb of the manifold. Flow was maintained in the distal common hepatic as well as throughout the SMA. Four months later, the patient presented to his local emergency department with a significant intracranial bleed which he expired from about a month later. Throughout the course, he showed no evidence of aneurysm growth.
Patient 3 is currently seven months post op and is doing quite well with no evidence of false lumen growth or end organ ischemia. All branches continue to remain patent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.