
Abstract
This work deals with the complex mechanical design task of converting a large pneumatic rehabilitation robot into an electric and compact system for in-home post-stroke therapies without losing performance. It presents the new HomeRehab robot that supports rehabilitation therapies in three dimensions with an adaptive controller that optimizes patient recovery. A preliminary usability test is also conducted to show that its performance resembles that found in RoboTherapist 2D commercial system designed for hospitals. The mechanical design of a novel and smart two-dimensional force sensor at the end-effector is also described.
Introduction
According to the World Health Organization, by 2050, the number of persons over 65 years old will increase by 73% in the industrialized countries and by 207% worldwide. 1 This segment of population is particularly prone to suffer a cerebrovascular accident or stroke, since the relative incidence of stroke doubles every decade after age 55. Stroke survivors immediately experience hemiparesis, resulting in impairment of extremities associated with diminished health-related quality of life. 2 Rehabilitation can help hemiparetic patients to learn new ways of using and moving their weak arms and legs. It is also possible with immediate therapy that people who suffer from hemiparesis may eventually regain movement. However, reductions in healthcare reimbursement place constant demands on rehabilitation specialists to reduce the cost of care and improve productivity. 3 Service providers have responded by shortening the length of patient hospitalization.4,5 Additionally, early home supported discharge of subacute stroke patients has been proved to have a significant impact on motor recovery after stroke although it requires some level of innovation of methods and tools for service delivery to really become a sustainable solution for the healthcare system.6,7 All these reasons support the necessity of in-home rehabilitation systems as the one proposed in this work.
Socially, chronic stroke patients can highly benefit from innovative approaches based on home rehabilitation therapy. 8 Technological and scientifically, only a few commercial systems are currently available for in-home use (e.g. HandMentor™, 9 ReJoyce, 10 and ArmeoBoom from Hocoma), and their performances are not comparable to in-person therapies. 11 Key challenges not addressed properly for home systems include features such as affordability, autonomy, and high performance. Only if all requirements are satisfied, it will be possible to encourage national health systems, insurance companies, and patients to apply such platforms.
This work is part of an ongoing project called HomeRehab that will develop a new tele-rehabilitation robotic system for delivering therapy to stroke patients at home. Instead, Technologies has a robotic system called RoboTherapist 2D (Figure 1) developed to provide rehabilitation to patients who suffer from stroke and/or other neurological disorders. 12 Currently, the system, as the majority of commercial devices, is only designed to be used in hospitals and medical centers in collaboration with nurses and medical staff. 13

RoboTherapist 2D system from Instead Technologies.
HomeRehab aims to modify and adapt the system so it can be used at home by patients easily and supporting the premise of tele-rehabilitation. 14 This article describes in detail the mechanical design of the new HomeRehab system that adapts the RoboTherapist 2D for in-home use by making it smaller, lighter, and cheaper, but maintaining its high performance. Additionally, the system includes a third degree-of-freedom (DOF) plus a novel low-cost force sensor that were not considered for the original platform, but they are very interesting features for a complete in-home solution. Another key feature of the whole system is that it integrates patient monitoring techniques using wearable devices to monitor the physiological state of the patient and modify exercises based on that information.
The following section briefly summarizes the main requirements considered to develop a successful device, and afterward in section “Mechanical design,” the mechanical design of the new system is described in detail. Section “Robot controller” presents the controller of the robot as well as the adaptive controller implemented for the rehabilitation therapies. Section “Usability pilot study” carries out a validation phase by conducting several tests and surveys to compare the usability of RoboTherapist 2D with HomeRehab, and last section gathers main conclusions.
Requirements
The intended use of the device is to provide rehabilitation therapy to patients who suffer from stroke and/or other neurological disorders. Besides, the system will also enable objective assessment based on quantitative measurements (e.g. by position and force sensors embedded in the robot body). The system should aid in improving the range of motion (ROM) of the affected limb as well as its strength by personalized repetitive motion activities.
The robot should be easily placed on a home table, where the patient would interact with it sitting down in a chair or a wheelchair. As such, all the components (e.g. motors, power source, and controller) should be concentrated in a small box, easy to carry and operate, or at least in the minimum possible space. The system should also be low cost but maintaining performance as much as possible compared to current hospital robotic systems. Additionally, there are two main features that have been considered meaningful to include in the robot in order to have an outstanding solution: (1) an optional third DOF for vertical motion (perpendicular to the table) and (2) a low-cost force sensor at the end-effector for safety and control issues.
Regarding the third DOF, the range of exercises that the patients could perform at their homes would increase drastically; thus, therapy performance could be boosted. The drawbacks are that adding a third DOF makes the design more complex, more expensive, and that the final workspace needed is much larger for a home location.
A force sensor at the end-effector allows monitoring the user intentions and applying appropriate control algorithms and safety strategies. However, commercial systems tend to be very costly. This article also deals with the development of a low-cost solution.
Workspace
One of the first inputs for the design of the new rehabilitation robot is the workspace needed, which is directly related to the ROM of the user. First, a standard user is characterized, 15 for which reference is taken on the data from the 95th percentile of the average European: 16 shoulder–elbow length, 410 mm; elbow–finger length, 520 mm. Regarding normal ROM for the shoulder, the following values will be taken as target for optimal rehabilitation therapies: adduction/abduction, 90°; and shoulder flexion, 90°.
By combining these user arm lengths with target ROM rotations for the shoulder, the necessary maximum workspace obtained by projecting all possible points is as follows: sagittal workspace, 304 mm; and frontal workspace, 658 mm.
From these data, it was decided to target a planar workspace of 800 mm wide by 400 mm long, forming a half circle around the patient. In this way, it is assured that most therapy movements will lay inside the workspace without reaching its limits, where usually robot manipulability is degraded. Regarding the vertical movement (perpendicular to the plane), and bearing in mind that the patient will be sitting on a chair, a 400-mm-long workspace is selected. In that way, the final workspace can be seen as a quarter sphere of 400 mm radius.
Force actuation
Regarding the force actuation capabilities of the device in all three Cartesian axes, the maximum force specification is somehow a subjective value. Force feedback will be necessary for both assistive and resistive exercises. Objectively, by considering the weight of a standard arm (95th percentile arm), that is, 4.14 kg, and accelerations between 0 and 10 m/s2 (above gravity), the system should be able to apply a 41.4 N maximum force value. Subjectively, for a desktop, lightweight, in-home device, this value may be too large. Moreover, typical hand accelerations are much lower. Based on our previous experience with RoboTherapist 2D system, a 28 N peak force value is selected for high-performance home rehabilitation exercising.
Force actuation also considers another two very important features: position resolution and mechanical transmission. Regarding position resolution, the higher the better, but previous experience in haptic design and control as well as literature17,18 shows that a position resolution in the order of 0.01 mm should be enough.
Finally, the more back-drivable is the device, the better and more transparent will be the interaction experience with the system, mainly in free motion. To achieve this feature, cable transmission should be used with a pulley-type reduction mechanism. However, this may also yield to a very large system considering target force specifications described above. This is another mechanical challenge for the design of the system.
Other specifications
The system should be as lightweight as possible. For its construction, a combination of rapid prototyping materials and aluminum is considered. A trade-off among cost, weight, and robustness will be taken into account to select which type of material should be used for each element.
Communication with the robot controller should be wireless (e.g. WiFi) in order to be flexible when installing the robot and all its components at home.
Another interesting feature could be to have the ability to easily interchange end-effectors. In this way, multiple end-effectors could be used for different patients and exercises (e.g. by designing end-effectors with additional wrist rotation DOF).
Mechanical design
The following picture shows the final shape of the new HomeRehab robotic device (Figure 2).

HomeRehab robotic device.
Mechanical design, as stated before, has been optimized for a high planar workspace of 800 mm wide by 400 mm long, forming a half circle around the patient. To achieve this, a quadrilateral layout of bars has been made, obtaining maximum tip movement with minimum rotation movement on its base. This makes possible to implement cable transmission to generate the force feedback.
Figure 3 shows the two-dimensional (2D) workspace of the robot limited by pulley travels. Mechanical ends have been added to further limit movements and for safety. Finally, workspace can be limited by software (e.g. implementing virtual walls) to the desired half-circle workspace, also shown at the picture.

Real 2D workspace of the device (blue) and workspace used for the exercises (red) limited by software.
As an evolution of the previous model, three-dimensional (3D) movement has been implemented by adding a third hinge in the base of the robot (Figure 4). This last DOF makes possible to have a 600 mm high with the same 400-mm-long vertical workspace.

HomeRehab pulleys and cable transmission system.
Mechanical transmission has been designed using cable that offers very good properties. Among all, the most important are its high back-drivability and low coefficient of friction. In this kind of transmission, size is key and has a direct relation with the amount of reduction it can achieve. To avoid exceeding size and weight, a combination of cable transmission reduction and planetary gear reduction has been applied. Specifically, a combination of 4:1 planetary gear reduction and 20:1 cable transmission reduction has been designed allowing to achieve a total of 80:1 reduction with good back-drivability while obtaining a high torque in the center hinge. All three motor-reductor pairs are equal, Maxon DCX32L-GPX32, with 128 mN m nominal motor torque. Maximum torque can be obtained with double the nominal current of the motor as defined by the manufacturer. This can be possible within five times the thermic constant, approximately 3.5 min. The whole mechanical transmission allows implementing a minimum force of 28 N in any configuration inside the workspace. Position sensing is obtained by three optical encoders (Maxon ENX16 1024 ppr) coupled to the motor axes. They allow a minimum resolution of 6 µm at the end-effector in any configuration inside the workspace.
The complete transmission setup has been calculated so that the three motors needed to actuate the robot are the same, making the final solution cheaper and simpler. For the planar actuation, two motors are needed. They share the same cable so that the design is simpler and less machined pieces are necessary. Cable tensioners have been implemented for easy setup and maintenance of the device, and end-stops to avoid cable transmission over-run. From the purely mechanical point of view, every potentially dangerous part of the robot has been placed on the back so that the patient cannot reach them from its sited position. This also allows placing the center of gravity near the tilting point, minimizing the apparent weight of the robot, but always at the front so that the robot remains stable when is not in operation.
Lightness is also a key factor in the design. To achieve this, aluminum 7075-T6 is considered for manufacturing. This aluminum is a perfect example of strength and lightness equilibrium, easy machining, and widely available in the market. The main pieces, the two pulleys, are designed to manufacture them by casting, with a finish machining in concrete place where tolerances are important (Figure 4).
For the bars, carbon fiber has been selected. This material has an incomparable ratio of weight and rigidity, and it is available in many shapes with competitive prices. The other pieces have been manufactured in Alumida, a new material as a result of combining polyamida and a 20% aluminum. This new material has a better resistance than the usual plastic materials used for additive manufacturing while lowering the deformation under load.
A detachable end-effector has been implemented for a high freedom of tip changing with two passive DOFs (Figure 5). Operation is simple, a custom nut releases the whole end-effector so that this can be changed rapidly. Interface is designed to avoid unwanted turns at the end while maintaining a simple design for future tip changes. The locking mechanism allows cable pass-through to connect different sensors inside the tip.

Detachable end-effector with two passive DOF.
The designed end-effector includes a big diameter handle for great comfort and easy user grip, a resting surface for seriously disabled patients who need support in early stages of recovery and a lever to activate or deactivate the last DOF necessary for a longitudinal actuation. The resting surface can be turned 180° for those patients who do not need this aid and for 3D movements, or it can also be detached. In 2D motion, the end-effector remains always vertical, and only one passive movement is allowed, blocking the tilt with the black lever. Note that 3D movements are only conceived for patients in the last phase of recovery that can manage the end-effector without the resting surface.
In this end-effector, a cheap force sensor has been implemented only for the 2D motion (Figure 6). It consists of a flexural system formed by four lever opposed couples distributed at 90°. With the same principle as a precision balance plate, each lever can be flexed in a radial direction so that a local deformation of the material occurs. When a rigid supported beam is flexed by a displacement on one of its supports, a strain is generated in the material, which leads to a moment diagram along the beam.

Low-cost force sensor based on a flexural system formed by four lever opposed couples distributed at 90° (left). Detail of strain gauges placement on one lever (right).
This basic flexural system has two advantages comparing with other solutions: on one hand, the relationship between the force applied and the strain produced is linear; on the other hand, it is a very simple mechanical system that derives in a cheap and reliable solution. To read this local deformation, strain gauges are used in full bridge configuration, with four strain gauges opposed in strain by pairs. Levers are designed in couples opposed vertically and also distributed 90° to its central axis. This way, 180° opposed couples are obtained for the two planar axis, obtaining four levers (with a strain gauge on each lever) for both axes of movement. Levers can be precisely designed to fulfill range and precision while choosing an overall rigidity for the end-effector. This ensures enough liberty in the design so that different sensors can be made depending on the range and the precision required.
Signal conditioning and acquisition is made through a HX711 24-bit analog-to-digital converter. The whole system is able to measure forces in the range of −30 to 30 N.
Table 1 shows the final specifications of the system that successfully fulfill target requirements listed in section “Requirements.”
HomeRehab specifications.

Robot controller
The robot controller is inside an electronic box that consists mainly of a NI MyRIO system for control and signal acquisition/commanding, 3 Maxon ESCON 50/5 drivers to control the motors, a 240 W power supply, and safety components such as switches and an emergency button. It runs a control loop at a frequency rate of 1 kHz that displays assistant forces to the user depending on the position and forces applied at the end-effector and the executed virtual task.
The main HomeRehab tele-rehabilitation application is conceived to run into a standard PC. It consists of a user interface with several virtual rehabilitation exercises and games. Communication with the robot controller is established over a wireless WiFi network, and alternatively via USB connection, sending and receiving User Datagram Protocol (UDP) messages with different configuration and position information. Wearable devices are connected directly to the PC by USB to monitor the physiological state of the user. At the beginning and ending of each therapy, session information can be exchanged with the therapist through the cloud using Microsoft Azure platform. Figure 7 shows a schematic of the dataflow among all HomeRehab subsystems.

Dataflow among all HomeRehab subsystems.
HomeRehab aims to develop an adaptive rehabilitation controller to select the right exercises to provoke motor plasticity on the patient and therefore improve motor recovery. It considers different strategies depending on the objectives of the therapy session: assisting the patient when the objective is to recover ROM or challenging the user when the goal is to improve muscle strength. Assistance controllers help the users move their impaired limbs through a predefined workspace, similar to a therapist moving the affected limb of the patient. There are multiple assistance controllers in the literature that differ in the strategy or assistance level provided to the user.19,20 Challenge or resistive controllers provide force feedback in the opposite direction toward the target point. The aim of these exercises is to promote muscle strength.
The assistive controller implemented in HomeRehab is based on the assist-as-needed approach, where the robot assists the user only as much as needed to accomplish the task. The idea behind this strategy is to encourage participant effort and self-initiated movements. Five discrete difficulty levels are defined. These levels are directly related to the ROM demanded to the users in the exercises (as percentage over the maximum workspace), and they are modified based on a performance indicator
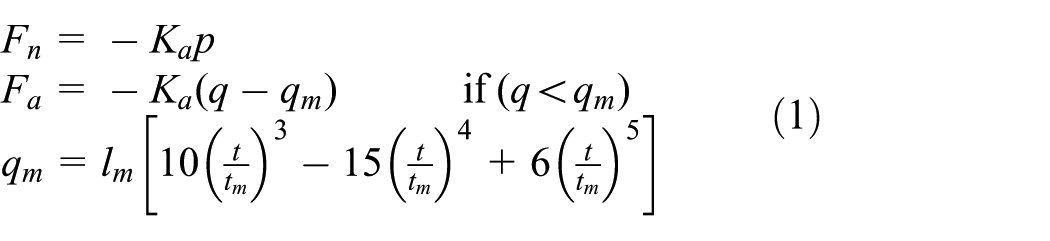
where the final robotic actuation is computed as the sum of an assistance force
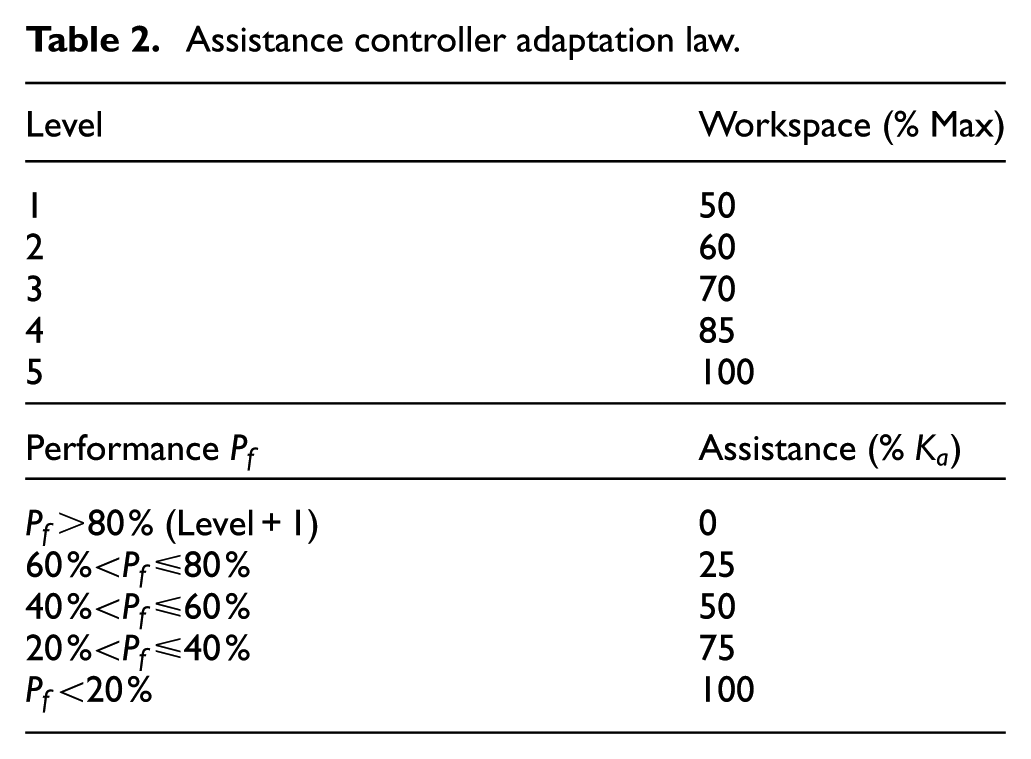
Table 2 shows the relationship among difficulty levels, exercise workspace (percentage over maximum workspace), assistance level (percentage over
Assistance controller adaptation law.
For muscle strength improvement, the user will be challenged by applying opposite forces to the target movement direction. There are also five levels of difficulty. An impedance-type force controller is implemented with a virtual spring whose stiffness

where
Resistance controller adaptation law.

HomeRehab has the distinctive capacity of being able to measure the physiological state of the user even in a home environment. 22 This is very important since it can be used to infer the stress level of the user prior to exercising. Stroke patients are often stressed while performing rehabilitation exercises, which affects performance. Three stress levels are considered: relax, medium, and stress. Depending on the state of the user, the game controller is adapted as follows: In relax mode, nothing changes from the adaptation laws described above; in medium level, the assistance level of the user is shifted to a higher value; and for a stress state, the difficulty level of the game is lowered one unit from previous session.
Usability pilot study
The objective of HomeRehab is to develop a robotic rehabilitation system with at least the same performance as RoboTherapist 2D but for in-home usage. Maintaining performance means that users are able to conduct the same exercises as with RoboTherapist 2D in hospitals, with similar ergonomic conditions, transparent movements, ROM, and force feedback capability and perception.
In order to validate the new system described in this work, a set of exercises is displayed to four patients at the Hospital Vega Baja (Spain), with both systems (Figure 8). The exercises displayed to patients are the same in both systems (game type, workspace, difficulty, and force feedback range). Afterward, patients are required to fulfill a questionnaire regarding five different aspects, including overall rate, satisfaction, ease of use, comfortableness, and security. The subjective rating covers a 7-point Likert scale, from 1 (worst) to 7 (best) for each of the adjectives proposed. The results for both devices were very similar in most of the aspects. Participants were very enthusiastic with the new approach and enjoyed the new system.

Validation and evaluation of usability issues of HomeRehab device at Hospital Vega Baja. HomeRehab device (left) and RoboTherapist 2D (right).
Conclusion
This article presents the mechanical design of the new HomeRehab robot that supports rehabilitation therapies in 3D with an adaptive controller that optimizes patient recovery. The aim was to develop a rehabilitation system for in-home use with similar performance to those systems found in hospitals, but with reduced size, weight, and price.
First, workspace, force, and other requirements are specified. Then, the mechanical solution proposed is presented in detail. The system is based on a quadrilateral layout of bars that obtains maximum tip movement with minimum rotation on its base. Back-drivability, transparency, and compactness of the solution are achieved by a careful combination of motor and pulley reduction driven through cable transmission. A third DOF has been added to allow 3D motions on demand, plus a low-cost 2D force sensor at the end-effector for control and safety issues.
The robot controller is also described. A novel adaptive controller for virtual rehabilitation exercising has also been implemented.
A preliminary usability test has also been carried out to compare HomeRehab performance with Robotherapist 2D. Results show that the system can resemble as well as the latter.
Future work will focus on improving and validating the adaptive controller to include additional performance metrics, such as user jerk measure, and conducting extensive clinical tests with patients to validate the whole system.
Footnotes
Handling Editor: Tadeusz Mikolajczyk
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by the European Commission through the project HOMEREHAB: Development of Robotic Technology for Post-Stroke Home Tele-Rehabilitation—Echord++ (Grant agreement no 601116).