
Abstract
Spinal interbody fusion is the most common surgery for treatment of disc degeneration, but the increased stress and compensatory range of motion at adjacent level have been noted. The dynamic cage design becomes an alternative strategy for dealing with problem of disc degeneration while the bony fusion is eventually required. Concept from a commercial cervical cage product with a ‘Z’-shaped dynamic feature has been evaluated and compared with intact cervical spine and conventional cage design by finite element method. Physiological loadings have been applied for evaluating the effect of cage design on biomechanical performances including adjacent disc stress and segmental range of motion. Results revealed that dynamic characteristic of the dynamic cage design shall effectively reduce the stress and range of motion at the adjacent disc, compared with conventional solid cage design, by providing sufficient mobility by itself. Torsional mobility was constrained due to its geometrical restriction. The dynamic function of cervical cage design may protect the disc adjacent to treat level from over-stressed and excessive mobility in early stage after fusion surgery. Further clinical investigation is required to determine the efficacy of cervical fusion by certain cervical cage with ‘Z’-shaped dynamic feature.
Introduction
With the reported high fusion rate up to 95%, the anterior cervical decompression and fusion (ACDF) with cage has been widely accepted for treating general cervical disc degeneration.1,2 However, clinical evidences showed that lowered in situ mobility after cervical fusion may result in the accelerated adjacent disc degeneration.3,4 The reduced cervical lordosis after ACDF surgery would redistribute the dynamic load and concentrated at the anterior column of cervical spine.5,6 Due to the compensatory effect of cervical mobility, the increased intradiscal pressure, range of motion (ROM) and facet joint load were observed and were recognized as the general complication after ACDF surgery.5–8
General fusion cage designs for cervical spine are mostly made from titanium alloy or polyetheretherketone (PEEK) material, which has been demonstrated with high biocompatibility. But the mechanical strengths of the aforementioned biomaterials are too strong compared to the intact intervertebral disc. Insufficient capabilities for compressibility (flexibility) and shock absorption may be the major problem that leads to postoperative complications. It is assumed that adequate in situ mobility preservation would be helpful for reducing the occurrence of adjacent disc problem after ACDF surgery. The concept of ‘dynamic cervical cage’ has recently been considered in several commercial product designs that provide possible alternative strategies in treatment of the degenerated cervical discs. This study aimed to evaluate a dynamic cervical cage design in biomechanical perspective and compared the effect of cage design on the adjacent disc and in situ mobility with conventional concept of cage design by finite element method.
Materials and methods
A commercial product, Z-Brace Dynamic Fusion Cage for cervical spine (Baui Biotech, Co., Ltd., Taiwan) made from titanium alloy, has been enrolled in this study for representing a cervical cage with dynamic design feature (Figure 1). The spring-like mechanism of Z-Brace Dynamic Fusion Cage, a ‘Z’-shaped design in lateral view, permits axial displacement and forward/backward flexion under cervical physiological loads. If a great physiological load is encountered, the self-engagement of the cage can prevent the structural from excessive deformation to maintain an adequate structural stability. The central window of the cage provides a tunnel for possible bone fusion, while the porous coating on the superior/interior surface of the cage may enhance the biological fixation. The three-dimensional model for the Z-Brace Dynamic Fusion Cage (Z-cage) and a general conventional solid cage (c-cage, PEEK material) were reconstructed as shown in Figure 2.

Z-Brace Dynamic Fusion Cage (for cervical spine, Baui Biotech).

Reconstructed cage models. Left: Z-Brace dynamic cage; right: conventional solid cage.
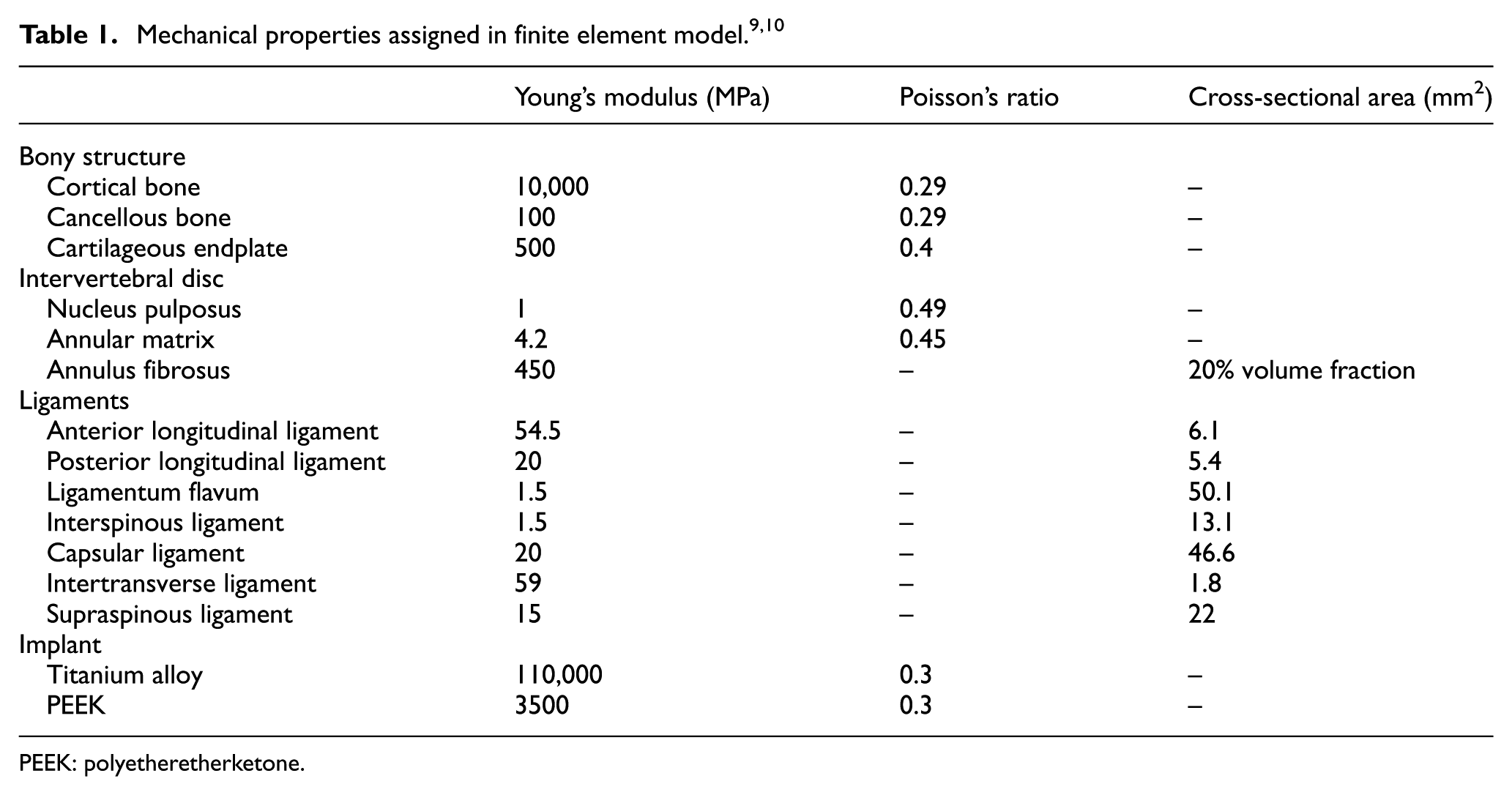
A validated cervical spine (C3-5) finite element model 9 has been used in this study (INT model). The two cage models were virtually inserted into the C4-5 intervertebral space at centre–centre location after the removal of intervertebral disc structure (Figure 3). Tetrahedron elements were applied for all solid parts in the finite element models, while the ligamentous structures were reconstructed using truss element. Table 1 represents the applied mechanical properties of the finite element models according to the previous literatures.9,10
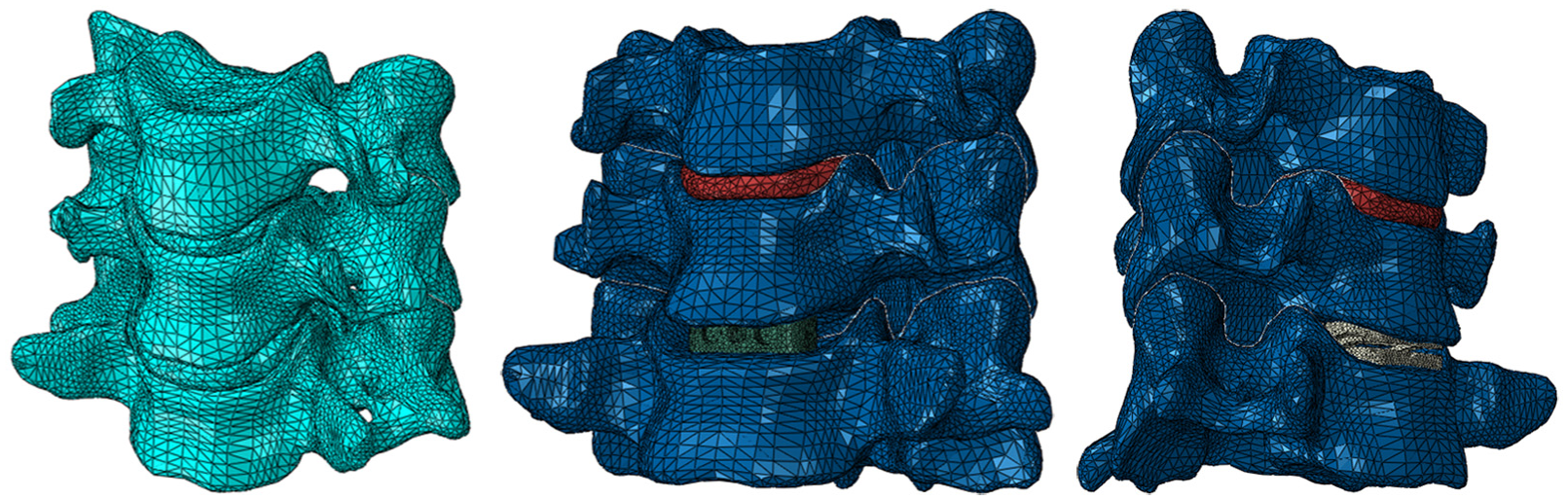
Left: intact C3-5 (INT) model; middle: the c-cage model; right: the z-cage model.
PEEK: polyetheretherketone.
The coefficients of friction at contact pairs are assigned by 0.5 at bone-cage interface, 0.1 between facet joints 11 and frictionless while the self-engagement of the Z-Brace Dynamic Fusion Cage occurs. Physiological environment of cervical spine models was applied by exerting an axial load of 73.6 N at the top of C3 superior endplate, while the bottom of C5 inferior endplate was fixed.9,10 Functional activities of cervical spine that 12° of flexion, 7° of extension, 8° of lateral bending and 4° of axial rotation were simulated for all models. The motion was defined by the final position and angular movement of C3 vertebral body, with a general concept of displacement control method for spinal movement simulation. Element numbers are, respectively, 170, 401; 175, 825; and 187,255 for the INT, c-cage and z-cage models determined by convergence test. Sizes of elements applied in the finite element model were 1.8, 0.8 and 0.4 mm, respectively, for bony structure, intervertebral disc and implants. For evaluating the effect of cage designs on the biomechanical performance of adjacent level and structural mobility, the C3-4 intervertebral disc stresses and the proportion for segmental ROMs were compared among all models.
Results
C3-4 intervertebral disc stress
The von Mises stress on C3-4 intervertebral disc adjacent to the treated level (C4-5) has been compared. Greatest disc stresses were revealed in c-cage model under all given cervical activities (flexion: 5.68 MPa; extension: 6.11 MPa; lateral bending: 6.41 MPa; axial rotation: 9.01 MPa). For the z-cage model, lowest stresses were found in flexion (1.16 MPa), extension (1.25 MPa) and lateral bending (1.94 MPa) compared to the other two models. However, it is observed that the z-cage represented similar mechanical response like c-cage model under axial rotation activity (9.00 MPa). Stress distributions and the magnitudes of disc stress are shown in Figure 4. Locations of high-stress concentrations were correlated to the corresponding motion applied to the model (i.e. motion direction corresponded).

Stress distributions and stress values of the simulated models.
Proportion of segmental ROMs
The INT model, without cage insertion, represented a balanced proportion in whole structural ROM (flexion–extension: C3-4 = 53%, C4-5 = 47%; lateral bending: C3-4 = 43%, C4-5 = 57%; axial rotation: C3-4 = 46%, C4-5 = 54%). Both cage-inserted models showed greatly influenced result. Obvious increases in C3-4 ROM proportion in the c-cage model have been found in all loading modes (flexion–extension: C3-4 = 83%, C4-5 = 17%; lateral bending: C3-4 = 76%, C4-5 = 24%; axial rotation: C3-4 = 80%, C4-5 = 20%). For the z-cage model, performances opposite to the c-cage model were found in flexion–extension (C3-4: 17%, C4-5: 83%) and lateral bending (C3-4: 23%, C4-5: 77%). Performance of z-cage model in axial rotation (axial rotation: C3-4 = 80%, C4-5 = 20%) was similar to c-cage model. Bar charts for better visualized representations are shown in Figure 5.
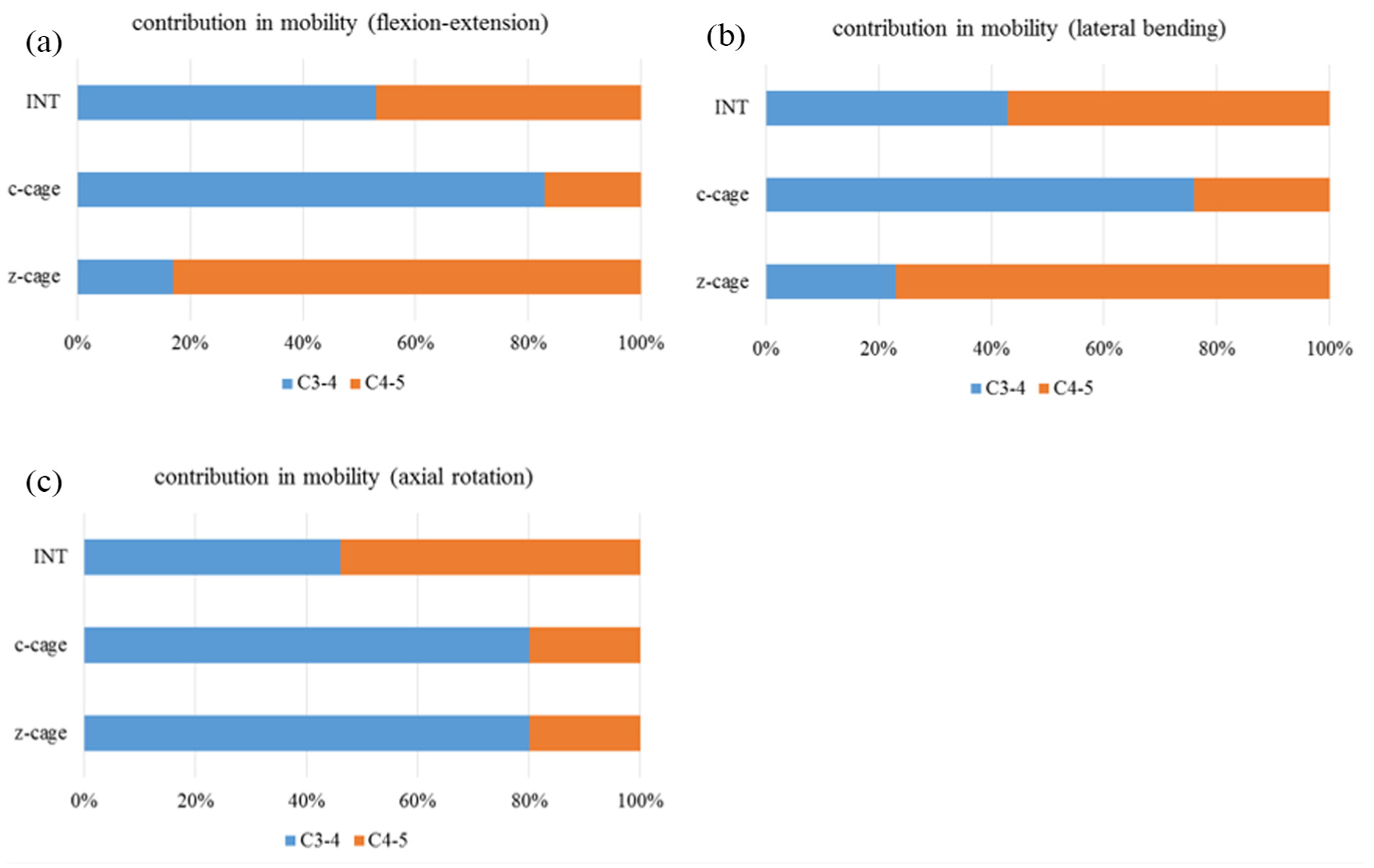
Proportion in segmental ROM for all models in various loading modes (a) flexion-extension, (b) lateral bending, and (c) axial rotation.
Other mechanical performances
This study cannot provide the mechanical data (such as force-deflection, moment-deflection and stiffness) directly because the displacement control method was used rather than force for moment control methods. But still, the general mechanical performance can be explained by the represented results. Lower disc stress indicates that comparative lower load (i.e. the required moment for achieving designate ROMs) was applied to the structure. That is, greater moments were needed to achieve designate flexion, extension and lateral bending for c-cage model, followed by INT model and then z-cage model. Same idea can also be discovered from the proportion of disc ROM in each model. Therefore, order of structural stiffness under flexion, extension and lateral bending can be confirmed as c-cage model > INT model > z-cage model. As for axial rotation, the greater stress and proportion of segmental motion of C3-4 in both c-cage and z-cage models clearly represented that low flexibility can be provided by both cages; thus, greater structural rotational stiffness can be confirmed for both c-cage and z-cage models than INT model.
Discussion
The finite element analyses were conducted to evaluate the effect of different cervical cage designs on biomechanical performances compared to the intact cervical model in this study. Results of these simulated models may provide quantified information for further references in cervical cage design to identify whether the dynamic mechanism is essential and beneficial. The compressibility and mobility of the dynamic cage design can possibly be considered as the function of shock absorption and may also avoid the over constraint at the early stage after surgery. Therefore, the occurrence of adjacent-level degeneration may possibly be eased compared to conventional ACDF surgery with firm/solid cage.
Previous in vitro study by Jacob et al. assumed that increase in intradiscal pressure at disc adjacent to the ACDF level is the major cause of the accelerated disc degeneration. 11 A 20-year clinical follow-up research by Gore et al. 7 reported that 16% of their patients underwent ACDF surgeries have suffered from severe adjacent-level degeneration and required reoperations. High prevalence of adjacent-level degeneration, which would eventually lead to structural instability after ACDF surgery, has been reported in several studies.6,8 The other possible issue is that an over-rigid fusion cage may result in cage subsidence and reduce the lordotic curve of cervical spine, which is also a risk factor to accelerate the adjacent disc degeneration. 5 The c-cage model represents the conventional solid-cage concept and has echoed the statement of previous studies that a strong cage construct can increase the intradiscal pressure at disc adjacent to the treated level. Significant increase in disc stress by around 56%–77% compared with the intact cervical (INT) model in various loading modes can cause the disc structure in jeopardy of the accelerated degeneration. As for the z-cage model, greatly lowered stress by around 46%–68% in flexion, extension and lateral bending can be helpful to reduce the risk of adjacent disc degeneration. An even lower stress compared to intact model can also be considered as a protection before the treated segment is finally fused. However, it should be noted that raised disc stress at C3-4 was found in z-cage model under axial torsion. Reason for this phenomenon is that the compressible feature of the spring-like ‘Z’ geometry can be applicable in axial compression, flexion, extension and partially in lateral bending. The structural may not be able to provide sufficient mobility in axial torsion due to geometrical restriction. Compared to thoracic and lumbar spine, the cervical spine is comparatively unstable in axial torsion. A confined ROM in axial torsion can possibly be helpful to maintain a stable environment for further bony fusion. Still, the simulated results supported that a spring-like structure of dynamic cage design shall be beneficial to reduce the stress at adjacent level.
The performance of segmental ROM has generally been considered as a referable factor to determine the stability of spine. 12 Dmitriev et al. 13 conducted an in vitro biomechanical study which demonstrated that decreased in situ ROM after anterior spinal fusion would cause compensatory increase in ROM at adjacent level, and also raises its intradiscal pressure. Clinical studies with radiographs or magnetic resonance (MR) images have provided sufficient practical evidences for support.6,14–16 This study also represented similar outcome that conventional cage (c-cage model) for ACDF surgery greatly reduces the in situ ROM that increased compensatory ROM would be found at adjacent level to accomplish the designated activities. In the c-cage model, larger proportion of ROM was transferred to C3-4 disc compared to the INT model in all loading modes. The raised ROM at intervertebral disc causes the disc structure to over-compress or over-distort, which is the major reason that raises the intradiscal pressure that echoes the aforementioned discussion for the increase in disc stress. As for the performance of z-cage model, the dynamic characteristic of cage design has been represented in flexion/extension and lateral-bending loads. The spring-like mechanism of z-cage model is capable to deform referring to the direction of exerted physiological load. Therefore, lower ROM is required for the adjacent level (C3-4) to reach the designated functional activities. Because of the aforementioned cause of the raised disc stress under axial torsion, this ‘Z’ geometry is stiff in axial torsion direction that compensatory increase in ROM can still be transferred to the adjacent level. Although that both disc stress and ROM at the intervertebral disc adjacent to the treat level were comparatively reduced in the z-cage model of this study (which can possibly be the statement that this design shall reduce the prevalence of adjacent level problem in early stage after ACDF surgery), it is essential to concern whether the cervical fusion can be successfully accomplished in clinical practice because the spinal cage is eventually an implant for bony fusion.
Some limitation of this finite element study should be noted:
The material properties of all components in current finite element model were assigned as homogenous, isotropic and linear elastic. This study focused on the effect of different designs of cages. The influence of simplified material properties of bony structure on simulated results can be comparatively minor.
We did not take the degenerated intervertebral disc into consideration. It is difficult to define the mechanical properties of a degenerated disc due to several complicated reason such as dehydration, reduced disc height and uneven structural hardening. In addition, the spike/serrated feature of the cage surface are simplified by applying a great coefficient of friction in substitution, which is generally used in similar finite element study.
Only centre–centre location of cage insertion in intervertebral space has been considered in this study. The different locations of cage placement would possibly be influential to segmental mobility after implantation.
Due to the limited resource in radiographs/computerized tomography images, the reconstructed cervical spine model ranged from C3 to C5 only. Therefore, only superior adjacent level (C3-4) before/after cage insertion at C4-5 level was evaluated. Although the previous clinical reports supported that greater incidence of accelerated disc degeneration generally occurred at the superior adjacent level in cervical fusion surgery, biomechanical effect on the inferior level may worth investigating for a more comprehensive understanding of the comparison between solid and dynamic fusion techniques.
Our plan for future study is first to obtain sufficient medical images to reconstruct a longer cervical model with more motion segments. Biomechanical performances on both discs superiorly and inferiorly adjacent to the cage-inserted level will be considered. The aforementioned variations such as disc properties (intact or degenerated) and cage inserting locations can then be adequately applied to complete the simulating work. If the implant specimen is available, mechanical test should be conducted to clearly confirm the performance of implant design. Finally, the simulated and practical tested data should be validated with realistic application in clinical practice if possible.
Conclusion
The major goal of ACDF surgery is to restore the segmental stability by intervertebral fusion, and a cage insertion is essential for sufficient strength in axial support. But conventional solid cage would be risky to induce adjacent-level degeneration. The concept of a commercial product, the Z-Brace Dynamic Fusion Cage, for cervical spine evaluated in this study can be protective to the adjacent disc from over-stressed and excessive mobility in early stage after fusion surgery. Further investigation on clinical follow-up will be essential for determining whether this dynamic cage concept would be influential to cervical fusion.
Footnotes
Acknowledgements
The authors thank Dr Chang-Hung Huang from Mackay Memorial Hospital, Taipei, for his technical support in finite element analyses.
Academic Editor: Rui Ruben
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.