
Abstract
Innovation lies at the heart of academia, and universities generate high-quality, intellectual property on a large scale. However, commercial translation of this intellectual property has traditionally been poor, particularly in the critical healthcare sector. It is critical that this situation is addressed to ensure that innovation from research institutes can fulfil its potential and progress to have a genuine impact on the outside world. In this article, we consider the nature of healthcare innovation in academia and ways in which commercial translation of intellectual property can be successfully realised. This is first analysed from an academic perspective, with a particular focus on how academic motivations and work practices can shape successful translation. We then switch perspective to examine the same process from an industry perspective, looking at the characteristics and expectations involved in the innovation life cycle. To place these analyses in context, we present a case study examining a project being undertaken to commercialise a novel surgical instrument, the intra-abdominal platform, from identification of clinical need, through the development life cycle, to commercialisation of the system. We reflect on the successes and challenges encountered during the intra-abdominal platform project, the broader lessons learned and in conclusion use these to emphasise how academia can adopt practices to better translate intellectual property in the future.
Keywords
Introduction: commercialising the intellectual property generated in universities
Innovation lies at the heart of academia, and universities generate intellectual property (IP) on a large scale. The standard of that IP is often high and that IP is of interest to the private sector, as demonstrated by the fact that start-ups spun out of universities are more successful than other start-ups.1,2 However, the rate at which spins-out companies are formed, or IP is successfully licensed, varies dramatically between universities. 3 While all universities generate lots of invention disclosures and patents, not all universities generate lots of licences and spin-outs. 4
Commercialising innovations, often called the translation of research, has not historically been seen as a strength of universities and other research organisations, with limited success and efficiency evident. 5 Only half of recommended healthcare practices are actually implemented,6,7 and it often takes upwards of 15 years for research findings to be fully translated into improved practice in the healthcare field. 8 The barriers to translation are various and interrelated and include inadequate design of research programs 9 (e.g. research not being designed to be easily adopted by the healthcare setting, or inadequate marketing of the idea to the setting so they do not quickly and easily see the benefits of the new idea), regulations being too onerous or policy dictating what interventions are adopted. 10 The word ‘translation’ hints at one of the problems, which is the difficulty of translating the innovative idea 11 from the language of the researcher to the language understood by the practitioner. 12
With these factors in mind, we now consider the nature of innovation in academia and what factors govern successful translation, first from an Academic perspective and second from an Industry perspective. We then present a case study of a project to commercialise a surgical support device, reflecting on the successes, challenges and lessons learned.
Translating academic innovation: an academic perspective
Some academics are wary of commercialisation and have reservations about the impact it may have on research, thinking it something which goes against their ideals of sharing knowledge with other researchers across the globe. The sharing of ideas, and joint innovation brought about by wide collaborations, ‘open innovation’, is a modern way to innovate. Large companies like Procter & Gamble are advocating the use of global innovation networks, saying, for example ‘Times have changed, and the world is more connected. In the areas in which we do business, there are millions of scientists, engineers and other companies globally. Why not collaborate with them?’ and even calling for new product ideas from the general public on their website. 13 It is generally accepted that, today, collaboration leads to better innovation. 14
Interestingly, the open innovation model is adopted by many large companies by means of forming networks of trusted research partners, rather than being absolutely open.14,15 It is important to be able to trust your partners, to be of the same mind-set and not be competitors. It is also important not to have such a large network that the research project becomes overly complex from an IP point of view; with every new research partner involved on a project, the complexity of the IP and contractual arrangements increases.
When it comes to commercialising innovations, university academics need to strike a balance between being open and sharing ideas, and protecting their ideas and IP, in order to exploit them commercially. The commercialisation of their ideas is important, as it is the pathway by which end-users actually get to enjoy the benefits of the innovations, but given that companies need to invest in the idea, often quite heavily, before they can take it to market, commercialisation of an idea requires an element of secrecy. The secrecy allows the company to obtain a patent, or other form of IP protection, and gain a period of at least a few years’ exclusivity before copycat products flood the market. Technology Transfer Offices in universities must reassure their academics that commercialisation can sit happily alongside research excellence and the sharing of knowledge. There is a need to reassure that patenting can sit alongside publishing provided the university provides the appropriate support mechanisms for timely and effective management of IP.
It takes time to commercialise ideas and many academic institutions now employ a Technology Transfer Office to help the academic hone their entrepreneurial skills and guide them through the various steps of the translation process. In particular, the market research, economics, IP assessment, and marketing are all critical in taking the idea to the stage where a company will invest in it.
The modern ‘open innovation’ networking model can be adopted by universities, just as it is being by companies. The network should be as wide as possible without becoming unwieldy. On the scale of the individual research project, a good project team will be multidisciplinary, to cover all bases, and will include (in the healthcare field) academics, healthcare professionals (the end-users), companies (medical device companies and private sector product designers), IP professionals and an innovation manager to market the idea to companies. It is also important to include patients or patient groups, who will ensure that the device is something they would be happy having used on them. The research needs to be designed for the healthcare practitioners: that is, it must ensure that the product is easy for them to adopt, cost effective for them to adopt and its benefits need to be clearly explained to them in a way which they can quickly and easily understand. To achieve this mode of translation requires all the talents of a multidisciplinary team.6,14
Translating academic innovation: an industry perspective
Clearly, academia and universities are centres for learning, but they are also hubs for innovation. The innovation context can range from being highly exploratory, for example, cancer cell therapies, through to a more commercially aligned approach, for example, creating solutions to solve an immediate and specific clinical need.
Research academics may adopt different approaches to innovation. Some researchers may have no desire, or need, to work with industry while for others it is standard practice. In the case of the former, the researchers perhaps create an open innovation platform whereby their work is published and used by collaborating universities on pioneering, long-term innovation. Another category of academics are those who have a desire to commercialise their innovations but perhaps do not understand or appreciate the amount of resources or funds required in order to migrate their piece of academic research into a commercially viable proposition. In this context, there is a need to better communicate what is required and the amount of time and effort needed. Finally, a growing group of academics have a desire to commercialise their innovations and understand and appreciate the need for industry engagement. In this context, they are accepting of a holistic and collaborative approach with a team of stakeholders with different skills and experiences, all with the common desire and goal of migrating the innovation into industry.
Universities are becoming more focused on commercialising their innovations. There are various platforms in which this can be achieved. For example, some universities have commercialisation facilities whereby the employees are focused on engaging with industry in order to create working relationships to develop the commercialisation of university innovations. This can result in licensing technology or perhaps creating a spin-out company which has a commercial focus. A typical successful example of this is Xiros Ltd which is one of the 100 spin-out companies that has been produced by the University of Leeds since 1995. Currently, 44 of these spin-out companies are active in areas as diverse as oil exploration, cancer drug development, geological research, embryology and foetal development. 16 Other universities create a platform strategy by which they have an attitude towards open innovation. This can be a peer-to-peer collaborative approach between universities or university and industry. A prime example is Manchester University who developed and published their research on Graphene. They have subsequently capitalised by becoming an international centre for Graphene-related research. 17
In healthcare, the National Health Service (NHS) have identified a need for universities to be encouraged to commercialise innovations. There is a better opportunity for success if the university academics create a partnership with industry. The National Institute for Health Research (NIHR) was created to improve patient and service outcomes through research which may include creating and fostering relationships between universities and industry and subsequently offering assistance in managing the process. The NIHR also have the ability to fund collaborative projects whereby the migration to success is increased. One such example is the Invention for Innovation (i4i) programme which has been successfully applied to the IAP project.
What does innovation look like? The reality
Innovation, by its very nature, can be planned or unplanned and the success or failure can be attributed to many factors. The innovation process requires a holistic approach with an appropriate blend of stakeholders which include academics and industry. The Gartner Hype Cycle18–20 is a popular description of the innovation process, 21 plotting expectations against time (Figure 1). After the initial ‘Trigger’ in which a project is conceived, there follows a ‘Peak of Inflated Expectation’, Trough of disillusionment, Slope of enlightenment and finally a Plateau of Productivity. A familiar point of failure with a project is commonly known as the ‘Valley of Death’. This is the critical point within an academically driven project whereby engagement with industry can be misaligned, misunderstood or lost. There are many cases within Universities whereby this is commonplace, and it is the responsibility of industry-focused academics and University commercialisation departments to avoid these situations.

An adapted graphical depiction of the Gartner Hype Cycle, showing different regions of the innovation process. 18
Clearly, all University-driven projects will have different challenges and opportunities when considering the commercialisation process. However, for successful translation, there needs to be a point within a project whereby the innovation migrates from a University push to an industry pull. There are many reasons why an otherwise potentially successful innovation can die in the ‘Valley of Death’. For example, the budget requirements required may not be sufficiently realised or could be inappropriately utilised; the stakeholders, managers and person resource may be inexperienced or lack the necessary focus; the technology could become compromised or obsoleted with the innovation process if protracted; new and emerging IP could circumvent the innovation; competing products could migrate to market quicker and if successfully marketed would reduce the commercial success of other subsequent innovation. It is worth highlighting that while it is easy to identify the characteristics and causes of the Valley of Death, it is not necessarily so easy to avoid. In the next section, we present our own experiences of this phenomenon and reflect that, in the context of the Gartner Hype Cycle, the activity of academic and industry partnerships is critical if projects are to move through the Trough of Disillusionment to a successful outcome.
Case study: commercial translation of the intra-abdominal platform surgical system
To illustrate the challenges inherent in translating healthcare innovation from academic to commercial impact, we present a case study on the intra-abdominal platform (IAP), a new surgical instrument for retraction in laparoscopy being developed by the authors.
The IAP system began as the result of discussions between colorectal surgeons and engineers at the University of Leeds, working together on a variety of projects under a Surgical Technologies research theme. A natural outcome of these close working relationships was identification of clinical needs in minimally invasive surgery (MIS) that could be addressed through engineering innovation.
Background
The advent of MIS has revolutionised clinical practice over the past decade with proven benefits in terms of less postoperative pain,22–24 shorter hospital stays,25–27 quicker return to normal function, fewer wound complications and improved cosmesis. 28 The continued implementation of this technique has resulted in predictions that 60%–90% of all general surgical procedures will be performed using this technology in the future. 29 However, the application of MIS presents significant challenges due to the fact that the surgeon’s hands are replaced by laparoscopic/endoscopic instruments to visualise and interact with tissues. These are manipulated from outside the body cavity and limit dexterous movements, visualisation and navigation, thus creating a significant learning curve for MIS which acts as a barrier, limiting adoption of MIS.
A key part of any operation is to ensure adequate exposure to the operating field by repositioning and retracting surrounding tissues, thus enabling the surgeon to effectively visualise and perform the intended procedure safely.30,31 In MIS, retraction is made difficult by the restrictive environment of the closed body cavity and a lack of suitable instrumentation. Typical practice involves an assistant holding and manipulating tissues under supervision of the lead surgeon but this is highly operator dependent. Other solutions have been proposed, ranging from the use of nylon sutures to retract tissues and organs,32,33 mechanical ‘hooking’ devices34,35 to more exploratory methods such as the use of externally controlled magnetic retractors. 30 However, current practice in MIS has seen minimal uptake of these approaches, and there is therefore a well-defined clinical need, and commercial opportunity, for the development of a retraction system for MIS.
The IAP development cycle
Development of the IAP is now considered using the Gartner Hype Cycle model, as the project moves from identification of clinical need through to the point of commercialisation, as illustrated in Figure 2.

Key points of IAP development mapped to the Gartner Hype Cycle.
Trigger: from clinical need to concept
The trigger for this research work was in identifying a clinical need for improved retraction in MIS. To better understand, and define, the clinical need, we developed a series of user needs, summarised below:
The retraction system should be ‘hands-free’ (thereby enabling a surgeon to concentrate on the operation in progress without dependency on an assistant).
The system should be able to quickly and reliably retract a variety of tissues in the abdominal cavity.
The device should support MIS principles (deployed and used with minimal trauma to the patient).
The system should not obstruct existing surgical processes or instrumentation.
This trigger phase is characterised by rapid development and an associated increase in expectations. This was particularly true for the IAP. A small team of engineers considered the user needs and a conceptual solution was developed in which a collapsible structure could be used to provide a ‘scaffold’ within the abdominal cavity, as summarised in Figure 4. From this concept, a series of functional prototypes were developed to explore key design parameters such as size and material selection. The team quickly arrived at a finalised conceptual design (Figure 3), for which a set of detailed design requirements were developed from the initial clinical user needs. These specifications encompassed considerations of size (its cross section must be comparable to existing MIS instrumentation for atraumatic insertion) and strength (it should be sufficiently strong, rigid and stable to retract a typical human liver). A full prototype design was then developed to meet the design requirements and a physical prototype fabricated through in-house workshop facilities, to positive feedback from our clinical advisors. Encouraged by these successes, a patent application was developed and filed to protect the IP (PCT/GB2011/051415, EP 2595548 A1) surrounding the concept and design.

The IAP concept: (a and b) The IAP is inserted through the abdominal wall in a collapse low-profile state, (c) after insertion the IAP is opened to provide a scaffold and clamped from above and (d) the clamped IAP arms provide a scaffold for tissue retraction using custom magnetised clips.
Inflated expectations
Following the promising outcomes of the trigger phase, the team secured 1 year’s funding from the EPSRC Medical Technologies Innovation and Knowledge Centre (IKC) to begin commercialisation of the IAP system. This involved accelerating development by expanding the core team to bring in dedicated expertise in medical device design (Pd-m International), fabrication (Sheffield Precision Medical Ltd) and innovation managers in the IKC. This expanded team worked to further refine the prototype, improving key aspects of functionality, for example introducing a low-profile clamping mechanism which helps minimise interference with other surgical tools.
At the culmination of the technical development process, an animal study was conducted to evaluate the surgical efficacy of the system. Here, a single porcine model was used in an MIS procedure with the IAP providing retraction for a range of tissues within the abdominal cavity, including gall bladder, small bowel and liver. The study was valuable in two respects: first, it highlighted a number of limitations that should be addressed in future developments (e.g. ensuring the operative field is sufficiently covered by the scaffold system); second, it demonstrated that the IAP concept has surgical utility.
The peak of expectation was reached when a second round of funding was secured to further develop the IAP. The funding was awarded by the UK NIHR through the ‘Invention for Innovation’ scheme (Ref: II-LA-0214-20003), designed to catalyse translation of healthcare technologies such as the IAP.
Trough of disillusionment
Commencing the NIHR-funded phase of IAP development represented a turning point in the project; the aims of the work were to develop a full commercial package for the IAP system. This required consideration of additional factors, notably Healthcare Economic Modelling, Design for Manufacture and supporting future regulatory approval. There was a corresponding need to expand the team to provide this expertise and undertake a critical assessment of the project in these domains. The outcome was a transition into the ‘Trough of Disillusionment’ as the process highlighted two significant challenges in realising a commercially viable product.
The challenges facing the IAP centred on assumptions made early in the development life cycle that it should be a reusable surgical instrument, as opposed to a disposable single-use device, based on informal analysis of trends in the world market. Healthcare Economic analysis highlighted that a reusable instance of the IAP might be commercially unviable for a manufacturer and retailer. In conjunction, a technical reappraisal of the system using rigorous Failure Mode and Effects Analysis ‘FMEA’ principles raised concerns around the multitude of small articulated joints in the system. These made it difficult to manufacture and assemble at tolerance, present a significant challenge for repeat cleaning and sterilisation and are vulnerable to corrosion and device failure.
This marked the nadir of our journey through the Hype Cycle; our system had demonstrated technical and clinical merit but was poorly suited for commercial translation into clinical use. It was evident that a new approach was required to deliver a single-use IAP system designed for manufacture.
Slope of enlightenment
To successfully progress from this critical point in the project, our team committed to an iterative collaborative design cycle. This included all the project’s key stakeholders in order to ensure that the resultant system was technically, clinically and commercially viable. Our approach is summarised in Figure 4.

A collaborative design cycle was used to take our (a) initial IAP design into (b) an iterative redesign with University of Leeds (UoL), design consultants (Pd-m) and clinicians (LTHT) to develop (c) the optimised telescopic IAP.
The redesign process was initiated by revisiting our User Needs and associated Design Requirements, from which a series of new concepts were produced by industry partners Pd-m. Crucially, these designs were conceived to consider aspects such as ease of manufacture and sterilisation from the outset. A collaborative design cycle was now followed to refine the designs, and key inputs included the following:
Mechanical analyses. Finite element modelling and experimental testing to ensure structural integrity.
Health economic modelling. Detailed analysis to understand market headroom constraints.
Clinical evaluation. Cadaveric models were used to ensure redesigns were clinically appropriate.
Design for manufacture. Designs were developed for plastic injection-moulding production.
The outcome of this process was a design which differed substantially from the original concept; the multitude of metallic articulated joints which formed the IAP expansion mechanism are replaced by a telescopic arm assembly and the entire assembly is manufactured using polymer injection moulding. The result is a low-cost, robust, clinically appropriate single-use system. In addition, our new approach has generated additional IP, free from prior art that may limit freedom to operate, and this has been protected through a UK patent filing. Overall, this provides a significantly improved package for commercial translation which is now our focus as we look towards commercial licensing deals in the Plateau of Productivity.
Discussion
The IAP case study presented above highlights that the realities of innovation and in particular the translation of healthcare technologies from academia to industry is rarely a straightforward process. However, with the benefit of hindsight, it is useful to reflect on the successes and challenges that have arisen during the IAP project.
Moving along the innovation pathway, from idea towards commercial product, is a complex process. In the context of medical devices, this requires development in areas spanning technical development and manufacture, clinical efficacy, regulatory approval and commercial viability. Accordingly, effective healthcare innovation requires a team with a multidisciplinary skillset able to address these varied areas of development. It is evident that few academic institutions, let alone individual researchers, possess all these skillsets. Thus, rather than adopting a unilateral approach, a more efficient model is to adopt a collaborative multidisciplinary approach that encompasses academia, industry and clinical inputs. Our work on the IAP project highlights the virtues of this multidisciplinary, multi-partner approach in which we adopted a collaborative design cycle to enable responsive, adaptive development, but arguably a more efficient approach would be to have employed the collaborative design cycle from the start of the project as summarised in Figure 4. No single member of the group could have conducted this breadth of work individually, the combined effort of the team was therefore critical to our success.
It should be noted that a multi-partner approach also brings its own particular challenges, as compared to working individually. The team must be managed to ensure their endeavour is coordinated, constructive and clearly defined. Central to this is effective communication, in particular ensuring that the role of each stakeholder is clearly defined and equally that they appreciate the skills, experience and roles of the other stakeholders in the team. In the context of the IAP project, this was manifest in linking our design-cycle activities (Figure 4); conceptual designs from industry designers were critically evaluated by university researchers and then passed for end-user appraisal with patients and clinicians. This requires the outputs from each stage of work to be clearly defined (e.g. does ‘prototype’ mean a computer-aided design (CAD) model or functional physical prototype?), delivered in a timely fashion (to ensure critical deadlines are met) and communicated effectively. Communication is particularly relevant in the context of healthcare innovation because it depends on close engagement of end-users, both patient and healthcare professionals. An inherent advantage of the multi-partner approach is that it promotes communication between these stakeholders and end-users, helping to ensure all parties are involved in the process.
An interesting consequence of using a collaborative model for innovation is that the academic(s) who originally conceived and developed an idea must necessarily play a smaller role as part of a larger multidisciplinary team. The size of this role is also likely to decrease as the project moves through the life cycle towards commercialisation. For a long-term project like the IAP, this also necessitates funding to not just build but maintain a team for the entirety of the project (which may span multiple funding rounds). This may conflict with traditional academic models of research practice in which the lead researcher remains in close control of their research, rather than ‘handing it on’. However, if academia is to improve its record of translating healthcare innovation, this seems a very necessary step and one which will bring benefits to all partners, from academic, through industry and ultimately benefit healthcare. In our experience, this requires trust among the team and recognition that the skills, experiences and motivations of academic and industry stakeholders differ, but are complementary. Academics are typically driven by the conception of new ideas while industry stakeholders are by definition more commercially driven. It is the combination of these entities, sustained over time, which promotes effective innovation, as highlighted in Figure 5.
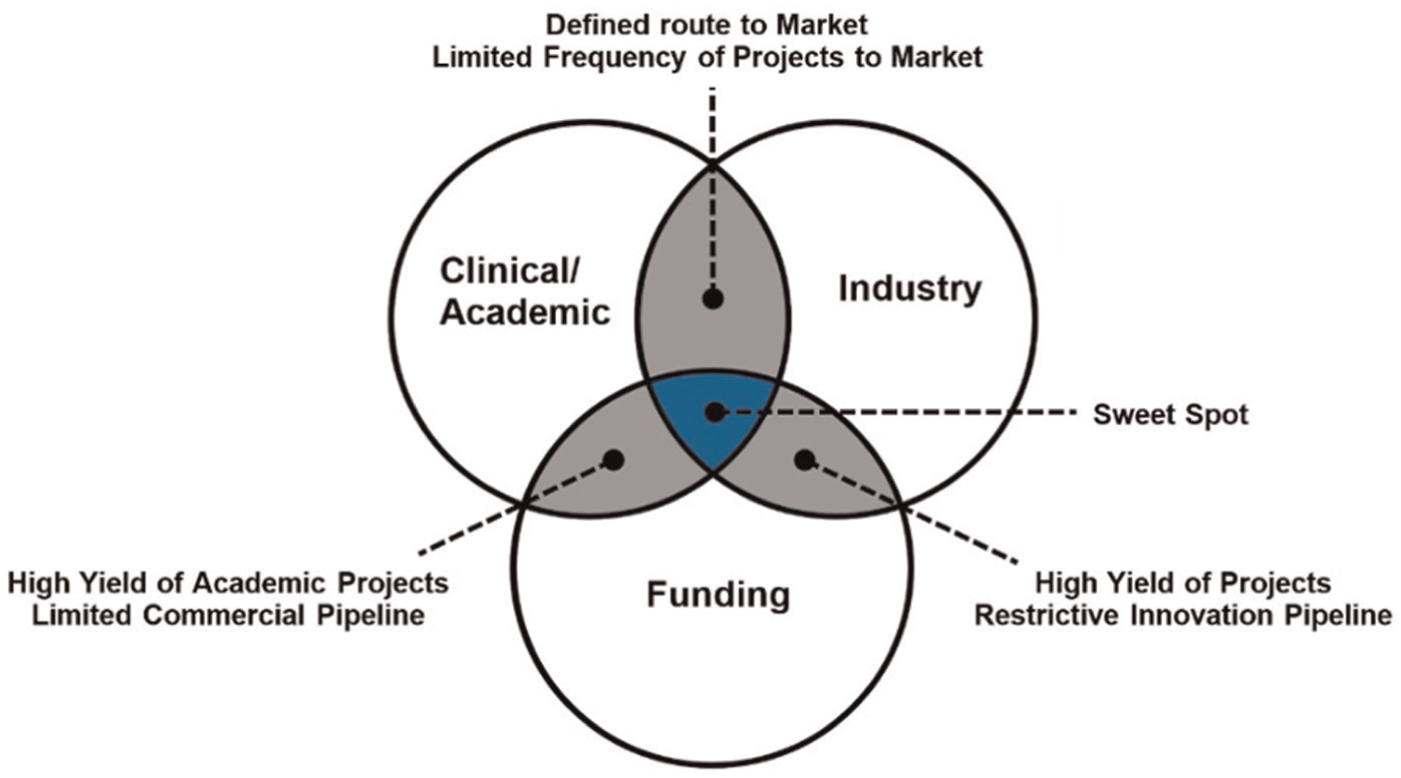
Identifying the combination of people, processes and product for successful innovation.
In our case study, we detail the innovation pathway of the IAP system in reference to stages of the Gartner Hype Cycle which provides an interesting framework to consider the evolution of a technology, in particular helping to reflect on periods of challenge and ways in which these may be overcome in the future. Early progress in our project was rapid, moving quickly from identification of the clinical need through conceptual design to a functional prototype. The resultant design provided a working solution which demonstrated the efficacy of using a device for tissue retraction in MIS. However, there was little consideration of future commercialisation in this process which ultimately forced us to redesign the IAP system. This highlights two important aspects for effective translation. First, in this instance, we were fortunate to have the resource and expertise available to perform a redesign, but arguably a more efficient approach would be to have employed the collaborative design cycle far earlier in the project. Second, technology can only be developed successfully if the team are receptive to change, reacting to the needs of the project without prejudice from their personal attachment to particular concepts or ideas. In both these aspects, our experience has shown that a collaborative multidisciplinary approach can help identify and avoid potential barriers to innovation, helping move the project through ‘valley of death’ towards commercial success.
Conclusion
In this article, we have examined the relationship between academia and innovation. Traditionally, researchers at universities have not been strong at translating their research towards commercial impact, a result of many factors including professional motivations, knowledge of the innovation process and expectations of outcomes. However, it is encouraging to note that this trend is shifting through the promotion of academic–industry partnerships and improved academic support systems to facilitate innovation translation.
The Gartner Hype Cycle provides a useful framework with which to critically analyse the process and highlighted those periods of particular challenge for the project were classic hurdles to innovation. While these can be readily identified post hoc, it is less easy to identify and overcome these challenges during the course of a project, which may lead to projects failing in the so-called innovation ‘valley of death’. It is therefore crucial to adopt appropriate working practices which help mitigate these risks to successful technology translation. Our experience with the IAP project has shown that using a multidisciplinary collaborative approach, harnessing the expertise of industry, academic researchers and clinicians, is a powerful means to achieve this and can help facilitate improved translation of healthcare technologies from academia to industry.
Footnotes
Academic Editor: Henrique Almeida
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Medical Technologies Innovation and Knowledge Centre (IKC) funded by the EPSRC grant numbers EP/G032483/1, EP/I019103/1 and EP/J017620/1; and the National Institute for Health Research (NIHR) i4i Scheme, II-LA-0214-20003. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. It has received support from the NIHR Healthcare Technology Cooperative in Colorectal Therapies.