
Abstract
To assess the biomechanical and clinical evidence available in use and efficacy of interspinous fusion devices and to explore indications for their application. MEDLINE search and Google Scholar were employed to find the relevant papers through the following key words: interspinous fusion, interspinous fixation, and posterior instrumentation. Based on their fixation modes and fused sites, the related classification for interspinous fusion devices will be established, and a systematic review of clinical and biomechanical studies was made. The results revealed that a total of 13 kinds of interspinous fusion devices were obtained, and they were classified into two main categories: (1) “interspinous fixation without situ fusion” type (or rigid interspinous fusion device) and (2) “interspinous fixation with situ fusion” type (or fused interspinous fusion device). Furthermore, a summary on its biomechanical and clinical study was given, which showed that interspinous fusion device could provide excellent biomechanical efficiency and promising clinical success. In conclusion, interspinous fusion device construct is a new potential fixation technique. However, further high-quality studies are still needed to clarify their long-term efficacy and indications for their use.
Introduction
Since the spinal fusion was initially introduced by Hibbs and Albee in 1911, the technique of fusion has been one of the most prevalent methods for treating conditions of the spine including deformity, trauma, degenerative disc disease (DDD), and spondylolisthesis. 1 The US population–based utilization rate of spinal fusion increased 2.1-fold from 64.5 discharges per 100,000 adults in 1998 to 135.5 in 2008. 2 Fusion is indicated to restore stability and prevent irritating intersegmental motion. Consequently rigid spinal instrumentation was utilized to acquire satisfactory fusion rates. 3 While pedicle screw/rod system remains providing sufficient stiffness for spinal fusion, pedicle screw insertion is a challenging technique with a steep learning curve. 4 It also has some unfavorable complications: paraspinal muscle dissection and retraction during instrumentation, screw malpositioning, neurologic risk, and lengthy operative time with blood loss. 5 Avoiding these current drawbacks, there has been a reappearance of past interspinous fusion constructs characteristic of minimal invasiveness and easing installation. 6 Varieties of emerging devices available in the market simultaneously come into being (e.g. SPIRE spinous process plate (SPP); Medtronic Sofamor Danek, Memphis, TN, USA and S-plate; Kisco DIR Co. Ltd, Osaka, Japan). Also, the patent for more similar product designs has been granted by the US Patent Office.
As a sort of emerging fusion devices, however, their safety and effectiveness (e.g. fusion rate, reconstructive stability, or complication) remain controversial, for whether there is enough biomechanical and clinical evidence is not known. Thus, it is necessary to systematically review the relevant evidence and efficacy of interspinous fusion devices (IFDs), which will provide a reliable foundation for the further design of IFDs.
To our knowledge, there is neither relevant category nor comprehensive synopsis of IFDs. This article incorporates the classification of these devices and simultaneously reviews related biomechanics and clinical applications involved.
Materials and methods
Inclusive criteria
Target population. Patients who suffered from deformity, trauma, DDD, and spondylolisthesis.
Types of studies. Clinical and biomechanical studies involving cadaveric test or finite element analysis.
Implants of interest. Inserted devices that use interspinous process as the site of the bone–implant interface for spinal fusion and segmental stabilization.
Evaluating factors. Outcome assessment of clinical studies was focused on operative time, blood loss, hospital length of stay (LOS), postoperative radiography, and validated patient-related questionnaires (e.g. Oswestry Disability Index (ODI) or Japanese Orthopaedic Association (JOA)). In the biomechanical studies, the main evaluating factors were to observe whether kinematic properties of spine and foraminal height were significantly influenced by the insertion of IFDs.
Exclusive criteria
Articles describing dynamic non-fusion technique (e.g. X-stop, Wallis, DIAM, and Coflex) or only pedicle screw system were excluded.
Search strategy
Papers of interest would be obtained, provided they met the aforementioned criteria through the following methods: (1) a MEDLINE search (1966–November 2013) and Google Scholar (http://scholar.google.com/) were employed, (2) the following key words were employed: interspinous fusion, interspinous fixation, posterior instrumentation, posterior fusion, SPP, and S-plate, and (3) other articles were acquired through reviewing the references from those identified papers.
Method of review
All related full texts available were analyzed and summarized after no significant exclusive criteria were found for those selected abstracts. In terms of IFDs’ feature, the related classification for devices was established to facilitate the analysis and review. For the biomechanical studies, stability at instrumented level and foraminal height was specially emphasized. While reviewing the clinical article, it was operative time, blood loss, hospital LOS, postoperative radiography, complications, and patient-related questionnaires (e.g. ODI, Visual Analog Scale (VAS), or JOA) that made up crucial evaluating factors.
Result
A MEDLINE search and Google Scholar by employing the key words generated 182 relevant articles. After each abstract was initially reviewed, there were relatively less studies according to inclusive criteria: only 26 papers were reserved. And then, eight more articles eligible were found by means of reviewing the references of those studies. There were 13 kinds of IFDs available in such clinical or biomechanical researches. To simplify the discussion of these devices, based on whether there exists interspinous situ fusion when IFDs instrument interbody or posterolateral fusion, we have classified them into two main categories: (1) “interspinous fixation without situ fusion” type (or rigid IFD) and (2) “interspinous fixation with situ fusion” type (or fused IFD) (Table 1, Figure 1). Relevant articles, from biomechanical or/and clinical perspective, were discussed for all different kinds of IFDs in the following sections.
Classification system of IFD device.

IFD: interspinous fusion device; CISB: ceramic interspinous block; SPP: SPIRE spinous process plate.
Prima LOK was a new interspinous fusion system product showed by OsteoMed Spine at the North American Spine Society (NASS) annual meeting, 23–27 October 2012, in Dallas, TX, USA. Any relevant article of this implant was not found.

Photographs of various existing IFD devices: (a) SPP, (b) S-plate, (c) Coflex-F, (d) Tadpole, (e) Aspen, (f) Affix., (g) Prima LOK, and (h) Axle.
Rigid IFD
Clinical evidence
SPP was approved for clinical application by Food and Drug Administration in 2003. There have been four studies with SPP: three comparative trials and one case report. Wang et al. 7 initially published the retrospective comparative study, in which 21 patients underwent anterior lumbar interbody fusion (ALIF) supplemented with SPP, and 11 patients received ALIF combined with bilateral pedicle screw (BPS). Also, pedicle screws were placed via either open approach (three cases) or a tubular retractor (eight cases). Patients aged from 27 to 70 years, with single-level lumbar DDD, presented with low-back pain (LBP) which derived from the target disc level based on physical examination and radiographic findings. Operative outcomes were reviewed to compare estimated blood loss (EBL), operative time (Op. time), and hospital LOS from the two groups. Findings suggested that the mean Op. time, EBL, and LOS in SPP group were all significantly less than that in open BPS group but was similar to that in tubular retractor BPS group. There were no surgery-related complications and higher fusion rates (100%) during mean follow-up periods of 7 months. 7 Thus, they argued that SPP fixation, which shortened operative time, decreased intraoperative blood loss, and reduced hospital LOS, could serve as a minimally invasive alternative to open BPS for many patients undergoing lumbar fusion. 7 However, this study had significant drawbacks. Sample size was significantly much smaller (e.g. open BPS group only had three cases), and follow-up periods were also not enough, which potentially caused bias or false negative errors. Although there were higher fusion rates, the symptomatic improvement of all patients was not too clear, lacking such functional scores for clinical outcomes such as VAS, JOA, and ODI (Table 2).
Comparison of Wang et al.’s and Kim et al.’s clinical study.
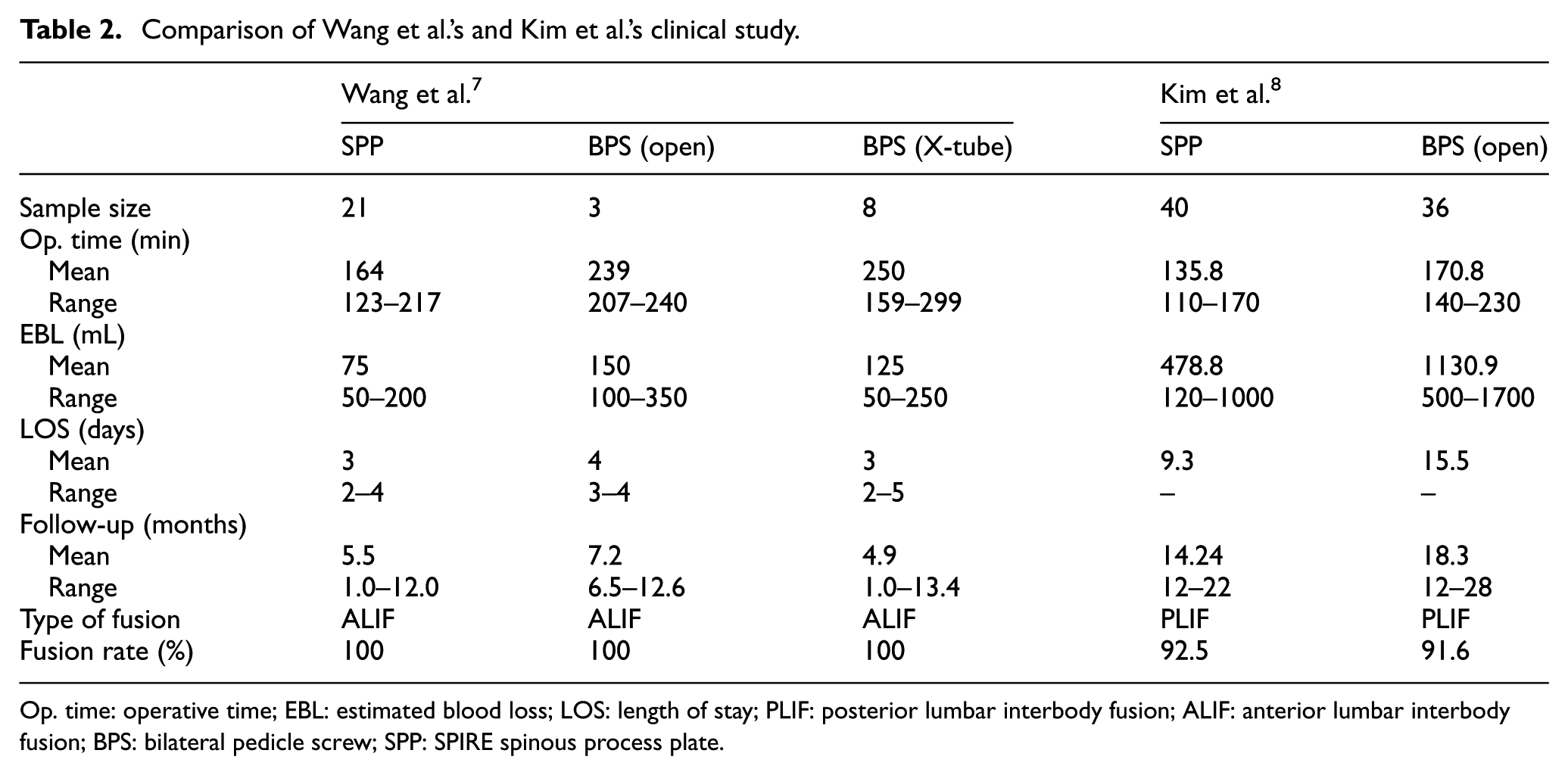
Op. time: operative time; EBL: estimated blood loss; LOS: length of stay; PLIF: posterior lumbar interbody fusion; ALIF: anterior lumbar interbody fusion; BPS: bilateral pedicle screw; SPP: SPIRE spinous process plate.
A case–control study was used on the clinical application of SPP combined with posterior lumbar interbody fusion (PLIF) by Kim et al. 8 This study included 76 cases with degenerative lumbar spinal diseases, who consecutively received either SPP instrumentation (40 patients as case group) or pedicle screws fixation (36 patients as control group). By comparison of EBL, operative time, and LOS between two groups, SPP had an advantage for minimally invasive treatment, equal to the conclusion from Wang et al. 7 (Table 2). Immediate postoperative and 1-year follow-up revealed that patients with SPP had more satisfactory clinical outcomes than that with pedicle screws by measurement using the VAS score. In contrast, the ODI was improved significantly in an equal amount in the patients with both fixations in 1 year postoperatively, with resemblance to the other comparative trial, 9 in which a 2-year follow-up showed that the change of JOA score was not significantly different between the SPP group (45 patients) and the pedicle screw group (85 patients). While SPP instrumentation achieved higher fusion rates (92.5%) than pedicle screws (91.6%), its complications had come to being fracture on articular process (one case) and retropulsion of interbody cage (two cases). 8 Relative contraindications they found were as follows: (1) pars interarticularis defects and (2) advanced degenerative spondylolisthesis (≥grade II). Regarding adjacent segment degeneration (ASD), Kaito et al. 9 compared SPP and pedicle screw, respectively, combined with PLIF at L4-5.The incidence of a second surgery because of ASD at L3-4 was significantly higher in the pedicle screw group (13%) compared to the SPP group (2%) during a minimum 2-year follow-up. Further studies should be obliged to evaluate the long-term efficacy of SPP in patients and its specific indications.
The earliest clinical study on the S-plate was found, in which Neo et al. 10 described the revision surgeries in using the S-plate as a salvage procedure for six patients subjected to failed anterior cervical fusion due to plate migration or nonunion at least 4 months after initial operation. A total of 100% bone union is attained in terms of radiographic criteria, when followed up for at least 18 months. A case report was published of intractable chronic LBP caused by lumbar ligamentopathia in the interspinous region by Iwatsuki et al. 11 Follow-up evidence indicated that VAS score and ODI were, respectively, improved from 8.0 and 80.0 preoperatively to 2.0 and 20.0 at the 12th postoperative month. In Tomii et al.’s 12 study, 15 patients with lumbar canal stenosis caused by spondylolisthesis, mean age: 73.1 (range: 55–83) years, underwent lumbar interbody fusion instrumented with S-plate instead of pedicle screw due to osteoporosis. During the follow-up period ranging from 1.5 to 4 years, average JOA score of those patients altered from 12.1/29 preoperatively to 21.9/29 at the final follow-up, and union was all achieved without complications associated with surgical invasion. However, it is worth noting that S-plate is not yet evidence-based due to its absence of comparative studies with other constructs, especially with pedicle screw.
Other less common rigid IFDs in the market include Tadpole system 13 and Vertical strut,14,15 described by recent sporadical case reports instead of comparative study. Kasai et al. 13 introduced Tadpole system as an anchor for lumbar interbody fusion. A total of 31 patients who underwent spinal fusion using the Tadpole system were followed up 2 years after the operation, and clinical evaluation was done analyzing operation time, time required for instrumentation, and EBL, which allowed for the minimally invasive superiority; the mean postoperative improvement rate of JOA score was 70.9%; bone fusion was confirmed in 29 of the 31 patients (93.5%) by X-ray images; there are no such complications as spinous process fracture, spinal fluid leakage, or neurogenic injury except the displacement of instrumentation arising in only one patient. Vertical strut, as an old method of the interspinous fixation in treating scoliosis, is occasionally used by surgeons due to its lower medical cost, 14 especially in the developing countries. But a recent study suggests that more emphasis must be placed on the severe complications in 10 cases (especially including graft extrusion in 1 case and death in 2 cases). 15 Admittedly, inadequate literature and absence of comparative trial make it difficult for both of the devices to draw some evidential clinical conclusions. But beyond that other rigid IFDs including Daab plate,16,17 Wilson plate, 18 and ceramic interspinous block (CISB),19,20 which were all obsolete, are also reviewed (Table 3), hopefully paving the way for the emergence of oncoming implants.
Clinical studies on obsolete IFD devices.
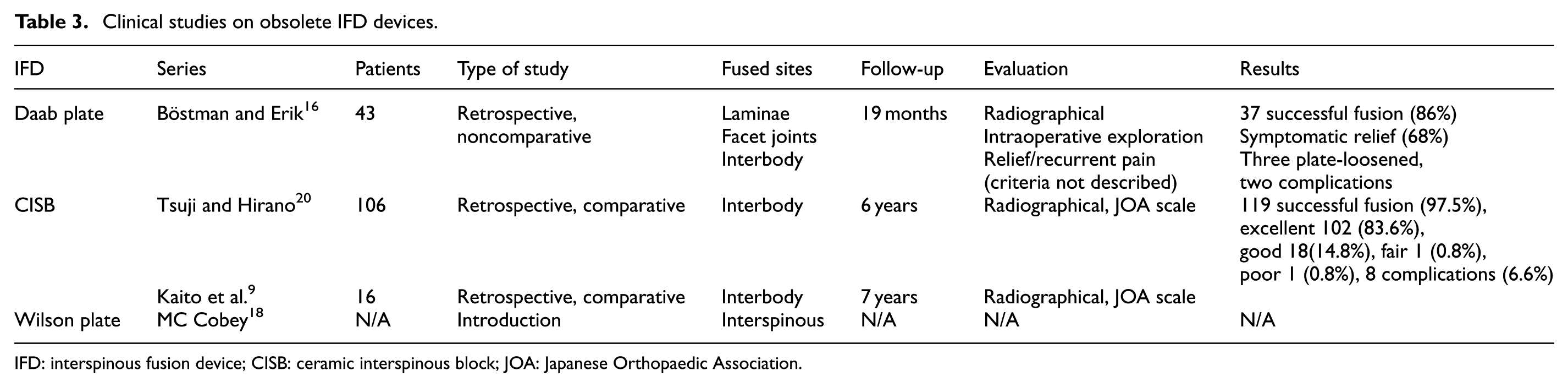
IFD: interspinous fusion device; CISB: ceramic interspinous block; JOA: Japanese Orthopaedic Association.
Biomechanical properties
Four rigid IFDs with their biomechanical studies were found: SPP (three articles), Tadpole system (one article), Affix (one article), and Coflex rivet (two articles). The in vitro testing, 21 compared with pedicle screw instrumentation, revealed that SPP provided enough stiffness in flexion–extension that was similar to BPS constructs, either with or without ALIF, and that SPP and unilateral pedicle screw (UPS) constructs were equivalent in resisting lateral bending and axial rotation forces with or without ALIF, which were all inferior to BPS constructs. Regarding the flexion–extension stability of SPP-instrumented segments, however, a retrospective case–control study 8 demonstrated that its amount of decrease in postoperative residual sagittal range of motion (ROM) was not as much as observed in pedicle screw group during 1-year radiographic follow-up, although each group was also decreased significantly compared with the preoperative ROM. Another biomechanical conclusion on the Tadpole device was nearly identical with the presence of SPP 13 (Table 4).
Biomechanical studies on existing IFD devices.

BPS: bilateral pedicle screw; UPS: unilateral pedicle screw; ROM: range of motion; PLIF: posterior lumbar interbody fusion; ALIF: anterior lumbar interbody fusion; TLIF: transforaminal lumbar interbody fusion; ASD: adjacent segment degeneration; IFD: interspinous fusion device; SPP: SPIRE spinous process plate.
Affix and Coflex rivet are such novel devices that their biomechanical data are scanty. Of course, none of them were approved for clinical application. In a cadaveric study, comparison between Affix and pedicle screw (bilateral or unilateral instrumentation) combined with interlaminar fusion was conducted by Ben et al. 22 They drew the conclusions similar to SPP in limiting flexion, extension, and lateral bending, except that there was no difference between Affix and pedicle screw under axial rotation. Coflex rivet or Coflex-F is an interspinous stabilizer with rivets modified from the original Coflex device. A biomechanical in vitro study indicated that the stability provided by stand-alone Coflex-F is much higher than that of the original Coflex in all directions. 23 In 2011, published finite element results suggested that the Coflex-F device with ALIF surgery could provide stability similar to the pedicle screw fixation with transforaminal lumbar interbody fusion (TLIF) or ALIF surgery. 24 But, they also reflected the lower rigidity of Coflex-F in both directions of lateral bending and axial rotation from ROM and von Mises stress distribution.
Kaito et al. 9 published a retrospective study investigating the possible reasons of ASD above lumbosacral-instrumented fusion. A total of 130 consecutive patients undergoing posterior L4-5 interbody fusion were followed by fixation of the segments with pedicle screw (85 patients) or SPP (45 patients). After a minimum follow-up of 2 years, the radiological incidence of ASD was lower in SPP group compared to the pedicle screw group (13% vs 32%). Since radiological finding was that the distraction of the intervertebral space by cage insertion was decreased after operation (which was also found by Tomii et al. 12 ), they put forward a “distraction theory” interpreting the above biomechanical results. Also, Kim et al. 8 have recently published analogical results of at least 1-year follow-up of 76 patients (40 SPP; 36 pedicle screw). The number of patients with radiological ASD was, respectively, 5 (12.5%) and 13 (36.1%). Then, a cadaveric study on Affix device showed that ROM adjacent to Affix was typically lower than those adjacent to laminectomy with BPSs, which probably implied the lower incidence of ASD in Affix. 22
Fused IFD
Clinical evidence
The clinical study on the Aspen device was presented by Vokshoor et al. 29 at the Western Neurosurgical Society annual meeting held in Colorado Springs, CO, USA. They evaluated 85 patients who underwent lumbar fusion with the Aspen system mean 24 months after operation (range: 18–30 months). It was a positive finding that demonstrated a 94% fusion rate detected by computerized tomography (CT) and a significant improvement from an average score of 6.5/10 preoperatively to 2.9/10 by measurement using the VAS. A multi-center prospective randomized study comparable to pedicle screws, provided by its developer, 30 indicated that insertion with Aspen device might save over a half hour of surgery time, lower the intraoperative EBL by 52%, and reduce the radiation exposure (RE) by 81% due to its easy setup. Whereas, we seriously doubted the accuracy of these data provided by its developer because the trail is not yet completed but currently recruiting participants. Kim et al. 31 published their prospective observational study, in which 50 levels (38 L4-5, 12 L3-4) from 38 patients were treated with 42 X-stop and 8 Aspen. A 1-year follow-up using CT and Zurich Claudication Questionnaire (ZCQ) showed X-stop or Aspen placement potentially caused the occult spinous fracture (22%), and patients with fractures tended toward poorer outcomes by ZCQ scores. But incidence of spinous fracture with Aspen did not clearly come up. In Kim et al.’s 32 another prospective cohort study, of six patients with Aspen, there were two patients with spinous fracture (33.3%) during the maximum 1-year follow-up. Besides the association with its design, high fracture rate was believed to be attributed to the larger proportion of patients with spondylolisthesis or low bone mineral density (BMD) of adjacent spinous process. Additionally, although histological animal model (sheep) demonstrated that mature lamellar bone was formed within the hollow spacer bridging the spinous processes, 33 whether interspinous fusion was authentically provided has been clinically unknown, despite higher interbody fusion rate (Table 5).
Clinical studies on existing IFD devices.

Op. time: operative time; EBL: estimated blood loss; LOS: length of stay; VAS: visual analog scale; ODI: Oswestry Disability Index; ZCQ: Zurich Claudication Questionnaire; RE: radiation exposure; IFD: interspinous fusion device; RCT: randomized controlled trial; BPS: bilateral pedicle screw; ASD: adjacent segment degeneration; SPP: SPIRE spinous process plate.
Oppenheim and Mills 37 reported four consecutive patients with recurrent lumbar disc herniation after discectomy. Those patients received the repeated micro lumbar discectomy (MLD) combined with an interspinous process fusion through an interspinous process plate. Consequently, if patients experienced minimal EBL, mean hospital stay was only 1 day. Mean ODI score was improved from 83.5 preoperatively to 37.0 at a final follow-up (mean: 12.9 months after reoperation). Finally, the technique of interspinous graft and cerclage wire, first described by Chandler, 38 is rarely used. The most typical reconstructive technique is the H-graft plus cable construct described by Fidler, 24 which is probably still used in some developing countries and areas. And we felt it be a prototype of the present and forthcoming “fused IFD.” Thus, this construct was also analyzed (Table 1).
Biomechanical properties
Karahalios et al. 31 completed a cadaveric laboratory investigation, with comparison among Aspen, anterior screw/plate, and BPS in combination with ALIF. Biomechanical results showed that the Aspen was significantly stiffer (reduction in the ROM to 25% of intact) than anterior screw/plate and the BPS in the flexion–extension, which, however, was less effective in limiting lateral bending (71% of intact) and axial rotation (71% of intact). Furthermore, they argued that ALIF with an Aspen provided stability that was statistically similar to ALIF with the BPS. Kaibara et al. 26 conducted the other in vitro study investigating the biomechanics of Aspen plus TLIF as well. The stiffness of Aspen with TLIF in all the directions was equivalent to their previous test by comparison of Aspen, UPS, and BPS. Whereas, the Aspen was biomechanically superior in flexion–extension, and the UPS was superior in resisting lateral bending, the stability provided by Aspen with UPS in the flexion–extension and rotation was similar to that of the BPS. Interestingly, results 27 from a recent paper were not consistent with the study from Kaibara et al., 26 in which there was no significant difference in the ROM of flexion–extension among the Aspen, UPS, and BPS in combination with TLIF. Also, the rigidity of Aspen with TLIF was not different from the intact group during the lateral bending and axial rotation. There were probably many reasons for this discrepancy in findings between the two studies, for example, fusion type (ALIF vs TLIF), testing methodology (pulley cable vs robot), and loading moment (7.5 vs 5 N m). Anyhow, all their data from the above two tests suggested that Aspen with TLIF and UPS could offer more excellent stability in comparison with BPS. On the other hand, Karahalios et al. 25 and Kaibara et al. 26 found that Aspen construct, by creating a segmental kyphosis, increases foraminal height more than any other construct. When commenting on the study by Kaibara et al., however, Wu and Praveen 39 thought that a segmental kyphosis caused by Aspen might potentially prevent the loading of the interbody cage or bone graft, which could lead to cage migration or pseudarthrosis.
For the Axle device, only one relevant kinematical literature was found. 34 Its biomechanical finding revealed that stability provided by Axle with PLIF after unilateral laminotomy was still strongest in the sagittal plane and was equivalent to BPS with PLIF in the transversal plane. But this is a preliminary study on Axle. Validity will need further investigation in the laboratory.
Biomechanical rationale
Biomechanical rationale addressing the stabilization characteristics in the sagittal, coronal, and transverse plane will be reviewed below.
According to three-column concept of spinal anatomy introduced by Denis 40 and Ferguson and Allen, 41 the anterior column is formed by the anterior two-thirds of the vertebral body, the anterior two-thirds of the annulus fibrosus, and the anterior longitudinal ligament; the middle column comprises the posterior one-thirds of the vertebral body, the posterior one-thirds of the annulus fibrosus, and the posterior longitudinal ligament; the posterior column includes supra- and infra-spinous ligaments, ligamentum flavum, pedicle, laminae, spinous process, and joint capsules. The principal element resisting the massive compressive forces experienced by the spine is the anterior and middle column supporting 80% of the spinal load. 42 The posterior bony spine serves to induce and control motion in the column, with bearing the tensile force. 43 Evans drew an analogy between the reconstructed spinal motion segment and a flagpole supported by tension wires. The pole (interbody graft) transmits compressive loads, while the tension wires (soft connective tissues or fixator) bear tensile load. Also, the higher the tension in the wires, the higher the compression in the pole, and the greater the resistance to toppling under the influences of “wind loads,” in other words, the stiffer motion the segment is. Thus, Cloward 44 and Lin et al. 45 recommend preserving as much as possible of the posterior tissue. Augmented posterior tensioning by preservation or reconstruction of the posterior axial ligaments is advantageous. Of course, tension stabilizer such as cerclage wire is an alternative fixation, especially in case of the slack posterior ligaments. 43 In this sense, rigid IFD is a desirable adjunct to interbody fusion because anterior graft, with tensile force rendered by rigid IFD, is subjected to more compressive loads that enhance bony fusion, as predicted by Wolff’s law. 42
There probably exists a valid principle that the stability attained from the absence of excessive motion between adjacent vertebrae facilitates bone in growth and eventual fusion.16,46 Seemingly, MW Fidler 24 showed much more interest in “rocking movement” of vertebrae around the graft in the sagittal plane. The abnormal movement occurring in the fused levels may lie responsible for the failing fusion. 43 Flexion of the spine usually obliges the front edge of the grafts or cage to become a fulcrum. Conversely, posterior edge is accordingly reduced to other pivot during hyperextension. 24 The rotary motion analogous to “lever” is inhibited by inserting a bone graft between the spinous processes in addition to the wiring of the processes.24,43 Likewise, Bono et al. 47 used an analogy of a playground “teeter-totter” to understand such a rotary motion. Keeping it stable by means of grasping it at one end (compared to IFD or pedicle screw) is much easier than stabilizing it near its fulcrum (compared to interbody cage). IFD is farther away from interbody cage than BPS from it, which explains the stiffest construct in the sagittal plane.
Interspinous dynamic stabilization systems such as X-stop and Wallis have gotten prevalence due to similar physiological load transmission and satisfactory clinical outcome. IFD and interspinous dynamic devices are all interspinous implants. To some extent, there exists greater similarity in stress transmission between them. 23 Stress distribution on the cage–bone interface and facets was always evaluated from finite element analysis or vitro cadaveric studies. As is opposed to interspinous dynamic spacers, most of the loadings were shared by the intervertebral space after implantation. Apophyseal joints, however, become unloaded or load-dropped due to posterior distraction,29,48–50 which was identical to those dynamic spacers. Thus, with a fused IFD as an adjunct to interbody fusion, compressive stress produced by the gravity is mostly distributed between cage–bone interface and interspinous graft, which is beneficial for the formation of interbody and interspinous bony union, as well as free from stress shielding. 23 On the other hand, Tsuji and Hirano’s 20 findings showed that compressive stress could probably spread more evenly on the graft–vertebra interface when IFD supplements interbody fusion, which favors fusion.
Discussion
Spinal fusion is a common surgical procedure for consolidating instable segments with the purpose of eliminating symptomatic back pain through decreasing or preventing intersegmental motion. Recently, posterior pedicle screw fixation combined with fusion is probably the most prevalent surgical approach and provides much higher fusion rates and promising clinical outcomes. Nevertheless, there are some disadvantages including paraspinal muscle dissection and retraction during instrumentation, screw malpositioning, neurologic risk and lengthy operative time with blood loss, and increased risk of infection. 16 Thus, these disadvantages give rise to the development of minimally invasive techniques which includes interspinous fixation in combination with spinal fusion. Furthermore, both biomechanical study and preliminary clinical evaluation have identified their efficiency.
It is worthwhile to mention that both IFD and interspinous dynamic device are among the interspinous fixation implants that share similar characteristics, for example, structures or shapes. Even Coflex-F spacer is an interspinous process device with rivets modified from the original Coflex device. IFD also has considerable merit of what interspinous dynamic device (e.g. X-stop, Coflex, or Wallis) characterizes: a lower EBL, shorter operative time, not significantly different hospital LOS, and the same complication rate as that of PLIF, which are confirmed in Cai’s meta-analysis indicating that clinical outcomes of interspinous spacers are equivalent to or even superior to PLIF. 51 Apart from the advantages on minimally invasive surgery, biomechanical study on Aspen confirms that IFD can provide an increase in foraminal height, which is the same mechanism of treating neurogenic symptom to dynamic device.25,26 However, IFD provides a stiffer reconstruct of motion segments for the purpose of obtaining stiffer bony fusion. In this sense, it probably has dual partial characteristics of rigid and dynamic techniques.
Even though IFD devices avoid some drawbacks that pedicle screw system is encountering, they come across hard nuts to crack. One concern regarding this technique is occult spinous process fractures due to relative structural weakness of the spinous process. Postoperative spinous process fractures have been reported in 1%–5.8% of patients in previous series based on routine biplanar radiographic evaluation. 31 Moreover, osteoporosis or osteopenia, which is probably a potential contraindication, is attributed to the erosion of the spinous processes. 31 In addition, IFD is likely to lead to breakage of arch due to conduction of stress in the isthmus of the neural arch. Tsuji and colleagues19,20 reported that two patients were caught in spondylolysis identified by radiography in 106 cases accepting interbody fusion supplemented by CISB. More importantly, there is authentic biomechanical fact that most of previous IFD devices provide relatively rigid stability in all the directions, other than in the lateral bending or axial rotation. 52 But surprising finding from recent research shows that similar favorable biomechanics to the pedicle screw system mercifully occurs in some novel IFD devices just like SPP and Aspen, which suggests that IFD could act as an alternative instrumentation promoting intersegmental fusion.25–27
The classification of IFD devices implies that fused IFD type gradually becomes a new trend for development of IFD device. All such novel IFD devices available in the market are belonging to the fused IFD type. Our speculation about this tendency is potential biomechanical superiority of fused IFD type in contrast to rigid IFD. With the resemblance in the early postoperative period, they all establish immediate stability for the bony union. But fused type may be inclined to provide more stability and strength of eventual fusion due to its extra interspinous fusion. Besides, an overall view of all researches on the IFDs reveals that there is a paucity of literature regarding the evaluation of clinical outcomes and reconstructive stability (including both surgical and adjacent segments) with long-term follow-up, and the specific indications and contraindications of these devices are also undefined in spinal degenerative diseases, on which emphasis of the further study should be laid.
Conclusion
In conclusion, IFD is a new potential fixation technique. However, further high-quality studies are needed to clarify their long-term efficacy and indications for their use.
Footnotes
Academic Editor: Henrique Almeida
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.