
Abstract
Spinal interbody fusion is the most common surgery for treatment of disk degeneration, but the increased stress on adjacent level has been noted. Disk replacement has become an alternative strategy for dealing with problem of disk degeneration. Compressibility of an intact intervertebral disk is contributive to protect spinal structure, but certain mechanism has seldom been preserved in most of the commercial products of ball-and-socket-styled artificial disks. A novel compressible artificial disk design for cervical spine has been developed and compared the biomechanical behaviors with intact and incompressible models by finite element method. Physiological loadings have been applied for evaluating the biomechanical performances in different implant designs. Compressible mechanism represented a similar kinematic behavior to intact cervical spine model. Greater mobility and larger facet joint contact force were observed in incompressible disk model. Biomechanical performances of cervical artificial disk with compressible mechanism may be better reproduced to those of intact cervical spine under physiological loadings. With adequate assigned structural stiffness of the compressible mechanism in the artificial disk, the concept is worth considering for further cervical artificial disk designs.
Introduction
The purpose of artificial disk replacement in spine is to maintain segmental mobility and to reduce the risk of adjacent level problem resulted from spinal fusion.1–3 The utility of artificial disk replacement is comparatively more popular in treatment of cervical disk degeneration with high satisfaction compared with lumbar disk replacement surgery. Clinical performance of several commercial disk products, such as ProDisc-C and Bryan disks, has been frequently reported and widely discussed. The Bryan disk is a typical compressible disk design with complicated mechanism inside. A previous biomechanical study reported that greater mobility of Bryan disk than ProDisc-C has been observed, but larger contact stress on facet joint has also been caused by Bryan disk replacement. 4 The compressible mechanism for mimicking intact spine feature would be beneficial to preserve adequate biomechanical and kinematic behaviors of implanted and adjacent segments of spine, while the ball-and-socket mechanism may provide sufficient joint articulating performance. However, the two aforementioned mechanisms have not yet been combined in any commercial product ever, neither has the biomechanical behavior of this concept been evaluated. The purpose of this study was to introduce a novel compressible cervical artificial disk design and to perform the biomechanical evaluation using finite element method.
Materials and methods
A C4-C5 cervical model has been built from series of computed tomography scanning images (slice thickness: 1.25 mm) and assembled in SolidWorks 2009 (SolidWorks Corp., USA) with reconstruction of intervertebral disk referring to the advices from experienced clinicians. The model was then imported to ABAQUS 6.8.1 (SIMULIA, Inc., USA) for element mesh (tetrahedron elements) and reconstructing ligamentous structure using truss element (Figure 1). Table 1 represents the applied mechanical properties of the finite element model according to the reported information from the previous literature. 5

Finite element model of the C4-C5 structure.
Mechanical properties assigned in finite element model. 5

Cervical model validation has been conducted in a physiological loading by exerting an axial load of 73.6 N at the top of C4 superior endplate, while the bottom of C5 inferior endplate was fixed. Functional moment of 1.8 N m for simulating flexion, extension, lateral bending, and axial rotation for the intact (INT) model was applied. Information in Table 2 represents the comparative information of current model validation to those from the previous literatures.
Finite element model validation in range of motion under physiological loads (unit: °).
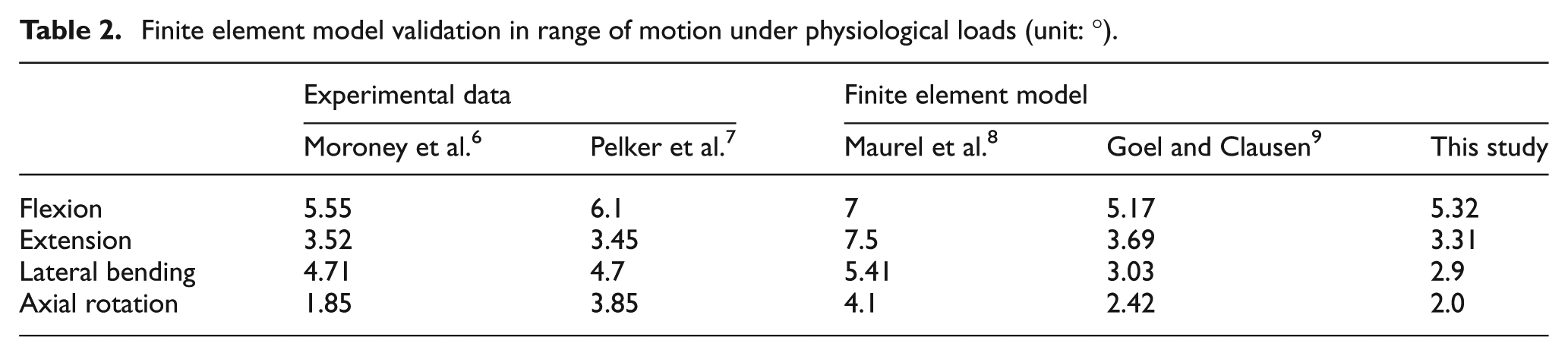
A compressible cervical artificial disk model and a conventional incompressible cervical artificial disk model were constructed referring to the geometry of ProDisc-C. Total height of these two models is identically 4.5 mm. Dual flexible spiral structure (outer spiral diameter: 5 mm; inner spiral diameter: 2.7 mm) is created in the compressible disk model with a film thickness of 1 mm and a assigned compressible space of 2.8 mm (Figure 2). The dual spring structure can be more resistive to lateral force which may lead to possible excessive range of motion (ROM) in lateral bending. To simplify the analysis, all components in the artificial disk models were assigned by the property of cobalt–chrome alloy. The compressible (CPS) and incompressible (ICPS) artificial disk models were separately inserted into the cervical model after removal of the original intervertebral disk structure (Figure 3) and were placed at the center–center location of the intervertebral space. Contact interfaces between the disk implants and bony structures were fully tied (fixed), while the coefficient of friction for the articulating surface of the artificial disks and C4-C5 facet joints were 0.1. 10 The simulated physiological loadings were identical to those utilized in model validation (axial load of 73.6 N and functional moments of 1.8 N m). 5 Axial displacement, segmental ROM, and facet contact force C4-C5 were evaluated.
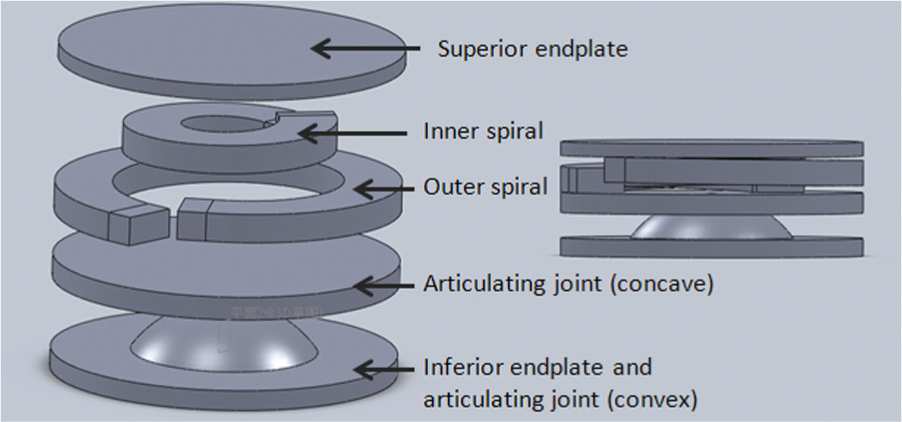
Structure of novel compressible cervical artificial disk.

Compressible (CPS, left) and incompressible (ICPS, right) models.
Results
Axial displacement
The observed axial compressive displacement under a compressive load of 73.6 N is shown in Figure 4. The CPS model represented greatest compressive distance (0.15 mm), while that of the ICPS model was hardly observed (0.03 mm).
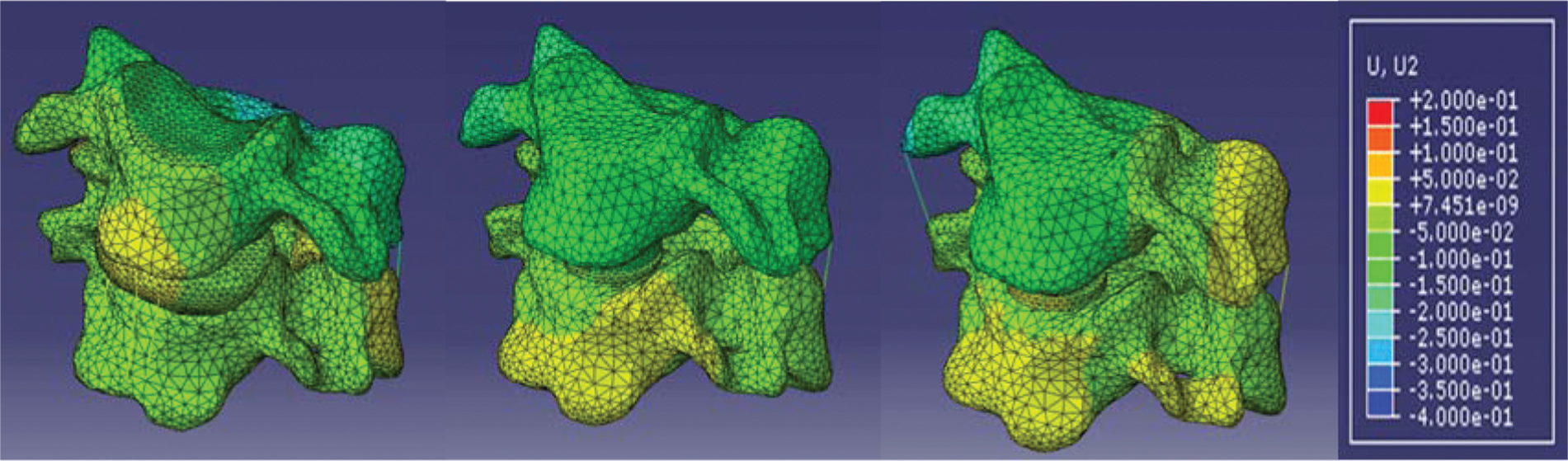
Axial compressive displacement of INT (left), CPS (middle), and ICPS (right) models.
ROM
Under functional moments of 1.8 N m, the ICPS model showed greatest ROMs for all motions except for flexion. The kinematic information is represented in Table 3.
Kinematic performance of simulated models (unit: °).

INT: intact; CPS: compressible; ICPS: incompressible.
Facet contact force
No contact has been detected under flexion in all models. The maximal contact force in each physiological load of INT, CPS, and ICPS models is listed in Table 4.
Maximal C4-C5 facet joint contact force (unit: N).

INT: intact; CPS: compressible; ICPS: incompressible.
Discussion
The finite element analyses were conducted to evaluate the effect of different cervical artificial disk designs on biomechanical performances compared to the intact cervical model. Results of these simulated models may provide quantified information for further references in cervical artificial disk design to identify whether the compressible mechanism is essential and beneficial. The compressibility of the artificial disk can possibly be considered as the function of shock absorption. LeHuec et al. 11 have conducted an in vitro biomechanical study to investigate two lumbar artificial disk designs (ProDisc-L and Maverick) by impact test, but no apparent capability of shock absorption has been revealed referring to the reported transmission ratio. The ICPS model, a conventional ball-and-socket joint design, showed less capability in axial displacement (0.03 mm) under an axial compressive load of 73.6 N in this study. Compared to the INT model (0.11 mm), the CPS model represented greatest compressive displacement (0.15 mm) in all simulated models. It is expected that certain cushion effect may be beneficial to prevent the damages of implants or bony structure due to sudden impact.
The performance of segmental ROM has generally been considered as a referable factor to determine the stability of spine. 12 Also, biomechanical study has demonstrated that increase in in situ ROM is expected after total disk replacement. 13 This study has represented similar trend that ROMs in all physiological motions have been raised in both CPS and ICPS models. In comparisons of ROM between the disk replacement models, the ICPS model showed greatest ROMs in all motions except flexion. The CPS model with compressible mechanism may be influential to the location of C4 vertebral body under the simulated physiological load in this study, indicating that the instant center of rotation may be altered by the compressible mechanism and finally may alter the motion pattern of the vertebrae. This phenomenon may provide the opportunity that the motion pattern can be adjusted by correcting the stiffness of the compressible mechanism (i.e. possible geometrical modifications on the flexible spiral structure such as the thickness, radius, and pitch) to achieve the performance of intact spine. However, the location for the placement of artificial disk may also be influential to the instant center of rotation of segmental motion. The cervical artificial disk models were only placed at the center–center location of the intervertebral space in this study. Further study may also take the location of disk implantation into consideration.
Facet joint is also an important anatomical structure in transmitting physiological load in spinal vertebra. Overload on facet joint may result in its accelerated degeneration, while abnormal motion pattern occurred if the load transmission through facet joint is insufficient. Previous studies have demonstrated that the load on facet joint would be raised after artificial disk replacement both in biomechanical test and computational analyses.13,14 In this study, both CPS and ICPS models showed lager facet contact force in extension and axial rotation. The possible reason for this phenomenon is that no remained intervertebral disk tissue is retained in CPS and ICPS models; hence, the worst case for spinal stability can be simulated. The anterior approach is taken for a general cervical artificial disk replacement surgery; thus, the surrounding tissue (the lateral and posterior walls of the annular structure) may be retained. However, the extremely high facet contact force in ICPS model under extension (24 N) was still risky for accelerated degeneration of the joint, while the force can be reduced to 13 N in CPS model. Following the discussion about the influence of the instant center of rotation, the altered location and motion pattern of C4 vertebrae may be the key factors in this effect on facet contact force. By adequate adjustment of the mechanical stiffness of the compressible mechanism, the goal of ideal magnitude of facet contact force may possibly be realized.
Several limitations in this study should be noted:
The material properties of all components in current finite element model were assigned as homogenous, isotropic, and linear elastic. This study has focused on the effect of different designs of artificial disks. The influence of simplified material properties of bony structure on simulated results may be comparatively minor.
The cervical model enrolled in this study was only C4-C5 segment, while the residual structure of intervertebral disk has been ignored. The effect on adjacent level and the biomechanical behaviors of the residual tissue which cannot be analyzed in this study should be further investigated.
As in the aforementioned statement, only center–center location of cervical artificial disk insertion in intervertebral space has been considered in this study. The different locations of artificial disk placement would be influential to motion pattern after implantation.
The ICPS model in this study was considered to evaluate the geometrical concept of general ball-and-socket-styled cervical artificial disk such as ProDisc-C but cannot be representative to the exact commercial product.
Conclusion
The goal of artificial disk replacement is to preserve the segmental mobility when surgical treatment is necessary in dealing with intervertebral disk degeneration. The novel compressible artificial disk introduced in this study can better achieve the physiological performance in capacity of axial compressibility, and better stability in physiological motion can be maintained. The design of the dual flexible spiral structure in this novel compressible artificial disk should be further investigated to obtain an optimal design with adequate structural stiffness to meet the motion pattern performed in an intact cervical spine.
Footnotes
Academic Editor: Magd Abdel Wahab
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported in part by the administrative bureau of Southern Taiwan Science Park under Grant Number AY-05-01-05-102.