
Abstract
Introduction
Participatory research (PR) has been found to have a positive impact on people living in long-term care (LTC). Yet, limited attention has been paid to the ethical complexities that are encountered in the research process. Our paper offers a reflexive account of the ethical issues related to power dynamics in a PR study involving the co-design of a virtual reality (VR) program in LTC.
Method
This reflection is part of a larger study to co-design a VR program in LTC settings. Our interdisciplinary team consists of an older adult with dementia, students and researchers in nursing, rehabilitation science, social work, computer science and engineering. We critically reflect on PR processes: co-design workshops, residents-led co-creation of videos, and staff-led VR implementation. We discussed the power dynamics faced, the methodological insights and lessons learned. A thematic analysis was conducted based on data drawn from fieldnotes, reflective memos, and team meeting discussions to identify recurring patterns related to power dynamics and participation.
Results
We identified the following themes: 1) the unintentional exclusion of residents’ voices in co-creation, 2) perceived autonomy and different levels of knowledge regarding VR technology, and 3) unfamiliarity with the research team and process.
Conclusions
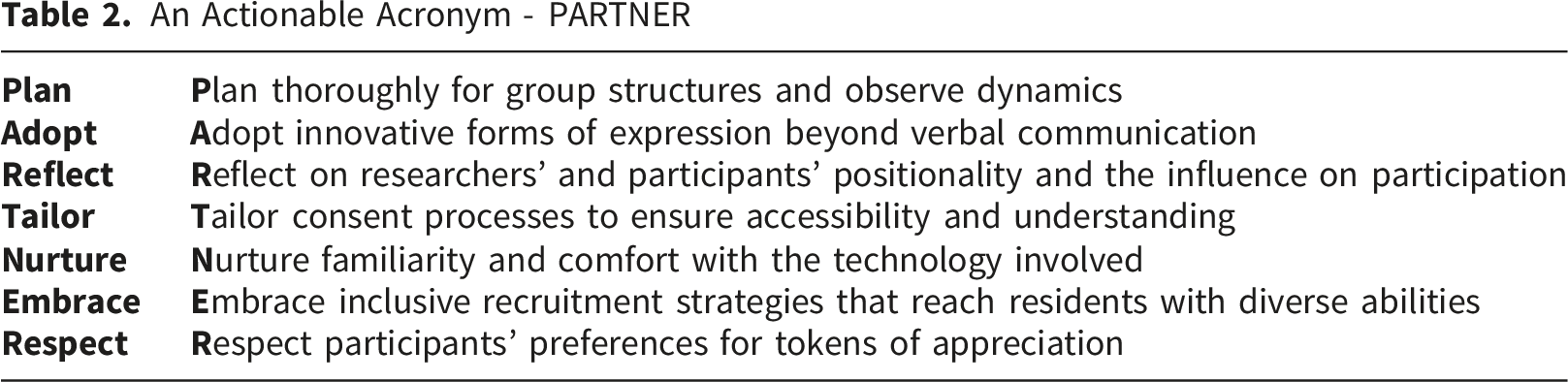
Our results underscore the fragility of inclusive engagement in PR. We summarized the lessons learned with the acronym - PARTNER to guide future PR and projects co-designing and implementing technological interventions in LTC to promote more inclusive participation. We argue that genuine participatory practice requires ongoing reflexivity on power dynamics, attention to structural constraints, and care for relational dynamics in LTC settings.
Introduction
Participatory research is an approach that involves people with lived experience and those directly affected by the research as active contributors (Vaughn & Jacquez, 2020). Their experiential knowledge offers valuable insights that can strengthen research quality and contribute to positive change in the communities involved. Several strengths of participatory research have been reported, including increased capacity for resource utilization, improved practices, and a higher likelihood of detecting problems within communities (Jagosh et al., 2012). However, participatory research also presents ethical and relational complexities. Common challenges include building and maintaining trust with community partners and ensuring there is no inequity in power or resources (Cargo, 2008).
In long-term care (LTC) settings, the use of participatory research has grown in response to the pressing need for more person-centred and inclusive approaches to care (Scheffelaar et al., 2020). By 2030, approximately 82 million people will be living with dementia (Guerchet et al., 2020). Within that number, 33% of those younger than 80 and 42% older will be residents who are living with dementia in LTC homes (Canadian Institute for Health Information, n.d.). The drivers of using participatory research in LTC include improved content validity and increased LTC residents’ involvement in research processes that directly impact them (Scheffelaar et al., 2020). In the study by Scheffelaar et al. (2020), the authors reported facilitators and barriers at different levels that should be considered in participatory research. Some of the facilitators from the co-researchers’ perspectives included motivation and preparation for the research, while the barriers included physical limitations and laborious processes (Scheffelaar et al., 2020). A scoping review conducted by Terkelsen et al. (2022) also revealed that future research should focus on co-creative and co-productive interventions for specific populations and should consider factors that impact the co-creative or co-productive process when working with older adults.
One strategy that is increasingly being used to improve care and residents’ quality of life in LTC is technology. Older adults living with dementia in LTC have diverse needs that technology can potentially fulfill. Virtual reality (VR) is an example of technology that offers new possibilities for engagement and improved health outcomes (Bhargava & Baths, 2022). Past research has shown that VR can improve overall quality of life for people living with dementia by enhancing mood and preserving cognitive function (Huang & Yang, 2022). Unfortunately, the currently available VR programs come with challenges. Some challenges associated with headsets include dizziness, experiencing discomfort, motion sickness and eye strain (Saredakis et al., 2020). There are also challenges to using VR in LTC, such as adapting this technology to the specific context of LTC settings and the lack of individualization in VR programs (Hosseini et al., 2023).
Current literature on VR or technology use in LTC settings focuses on exploring outcomes, facilitators, and barriers to implementation; much less attention has been given to the participatory processes in developing these technologies (Hung et al., 2023; Wong et al., 2024). While the work by Gaber et al. (2024) and Scheffelaar et al. (2020) laid a foundation for illuminating the “backstage processes” of participatory research in LTC, they did not include studies or reflections on participatory research related to the development of technology in LTC. Technology can introduce a layer of complexity to collaboration with partners in LTC; for example, residents’ and staff’s perceptions of the technology may shape the co-creation process differently. With emerging interest in using technology to support the quality of life and care for residents in LTC, it is crucial to also explore the “behind-the-scenes” processes of co-creating technology in LTC.
In this paper, we present a reflexive account of our experience co-developing a VR program through the Virtual Immersive Program (VIP) project, a co-created, person-centred initiative designed to enhance the quality of life for people living with dementia in LTC settings. We focus on the ethical complexities that emerged during co-design, video co-creation, and implementation. Guided by the critical theoretical lens, we examine how power dynamics between researchers and participants can influence the research process. Our reflection contributes to growing calls for deeper attention to the everyday, often “messy,” relational work of participatory research and highlights the need for ethical, inclusive innovation in LTC.
Theoretical Foundations
We adopt a critical theoretical lens to guide our examination of power dynamics in research with marginalized populations in long-term care settings. Drawing on Foucauldian perspectives (Powell, 2023), power is conceptualized as relational and embedded in social structures, shaping which knowledge is legitimized and whose voices are heard. Several key tenets that guide our critical lens (Levitt, 2021): 1. 2. 3.
By applying this lens, our study emphasizes co-research approaches, participatory practices, and research that generates tangible benefits for the studied population. This includes designing inclusive environments that account for participants’ varied cognitive and physical abilities and ensuring that their perspectives meaningfully inform the research process.
About the VIP Project
The VIP project is a participatory project conducted in LTC settings with residents, families, staff, and interdisciplinary researchers. Grounded in human-centred design principles, the project actively involves residents, families, staff, and decision-makers in developing a personalized and accessible VR program tailored to their needs and preferences. The project explores two research questions: (1) How do residents, families, and staff perceive a VR program in LTC, including its content, barriers, and facilitators? (2) What are the experiences (positive impact and challenges) of people living with dementia, families, staff, and decision makers, in co-designing a virtual immersive experience program in LTC?
To address the research questions, the team employed qualitative methods, including focus groups (co-design workshops), interviews, and observations in two LTC homes in Vancouver, Canada. Data were gathered iteratively to inform the adaptive development of the VR program. We used various VR technologies, including VR headsets and projectors, and adopted diverse strategies informed by input from all participants. This participatory initiative aimed to reduce loneliness and foster social connection in LTC homes, and to challenge exclusionary models of technology design and implementation by centring the voices of people with dementia throughout the research and development process. By prioritizing lived experiences, the VIP project offers a scalable and sustainable model for inclusive innovation in dementia care within LTC. The study was approved by the Research Ethics Board of the participating universities (Ethics ID: H23-01481). Written informed consent was obtained from participants before participation, with the purpose and details of the study discussed. Verbal consent was obtained before each co-design activity. All participants in the study were reminded of the research’s purpose and their right to withdraw at any time.
Methods
This reflection paper focuses on the ethical and relational dimensions of the participatory process—what we call the “backstage” work—highlighting the importance of reflexivity, shared learning, and methodological transparency in participatory research. To guide this reflection, we adopted Rolfe’s et al. (2001) model of reflection, which has been widely used in collaborative research, including studies on dementia and technology (Sakamoto et al., 2023). This reflection centres on three key questions which inform the structure of our paper: (1) What? – What ethical issues related to power dynamics emerged during co-design processes? (2) So what? – Why do these ethical reflections matter for participatory research in LTC? (3) Now what? – What actions should be taken?
Team Roles
VIP Research Team
Our research team is multi-disciplinary. It consists of an older adult living with dementia, two family partners, undergraduate and graduate student trainees from the disciplines of nursing, social work, science, biomedical engineering, health sciences, political science, and researchers in nursing, rehabilitation science and computer science. Throughout the project, our interdisciplinary research team met weekly, either in person or via Zoom, for one-hour sessions to share progress updates, discuss emerging challenges in the co-design process, ethical dilemmas and technical aspects, and collaboratively develop mitigation strategies. In addition, team members who facilitated the co-design workshops held a 30-minute debriefing session after each workshop. These debriefs were used to reflect on the data collection process, record insights, and inform ongoing work. Trainees also wrote field notes and reflective memos after site visits to co-create videos with residents and observe staff-led VR adoption. These reflections were an integral part of our trustworthiness strategy of reflexivity.
The Reflection Team
The reflection team involves all authors of this paper, who represent the majority of the research team. It consists of undergraduate and graduate student trainees from the disciplines of nursing, social work, biomedical engineering, science and health sciences, an older adult living with dementia, and researchers in nursing, rehabilitation science and computer science. Four research trainees, including JW, KW, AS and MV, were deeply involved in the data analysis, from generating codes to preliminary themes. The four trainees presented to the larger reflection team for discussing the final themes and manuscript development.
Data Analysis
Coding Examples

Positionality and Reflexivity
Our team reflection process was collaborative, involving all team members. It was also reflexive, grounded in an awareness that our diverse social locations shape our perspectives and interpretations. Our reflection team included members with diverse experiences working on projects in LTC, with older adults living with dementia, family members, and frontline staff. For example, some team members’ long-standing healthcare experience provided an insider perspective on the institutional hierarchy of the healthcare system. However, this perspective may also create “blind spots,” leading members to make assumptions solely based on their healthcare experiences and clinical norms. Members from diverse disciplinary backgrounds and with less experience working on LTC projects could offer another perspective, challenge potential assumptions and stimulate fruitful conversations regarding the power dynamics encountered during the research process. Team members were also aware of how our diverse cultural backgrounds could shape interpretations and understanding of power dynamics. The team member living with dementia’s role was crucial in ensuring constant reminders to team members about their assumptions and in shifting the discussions from a theoretical lens to the lived reality of residents. For example, our patient partner’s experiences of diverse group dynamics in other participatory research projects simulated and enriched the team’s reflexive dialogue in the ethical issues behind our co-design workshops’ designs in our project. The collaborative, reflexive reflection process encouraged team members to acknowledge their diverse assumptions and challenged the team to critically reflect on the research process from multiple angles.
Results
What? – What Ethical Issues Related to Power Dynamics Emerged During Co-Design Processes?
We identified the following themes: 1) the unintentional exclusion of residents’ voices in co-creation, 2) perceived autonomy and different levels of knowledge regarding VR technology, and 3) unfamiliarity with the research team and process.
The Unintentional Exclusion of Residents’ Voices in the Co-Creation Processes
Power dynamics played a central role in shaping how residents’ voices were included—or excluded—throughout the co-creation process. Despite the team’s commitment to inclusive engagement, certain practices unintentionally constrained whose perspectives were heard and prioritized.
Recruitment Strategy
A contributor to this imbalance was the staff-mediated recruitment strategy. Staff selected residents based on criteria provided by the research team, which prioritized participants who were verbally communicative and able to engage in dialogue. As a result, only residents with strong verbal communication skills were invited to participate, excluding those who communicate differently (i.e., through non-verbal means). Although these decisions were made with the intent to facilitate smooth collaboration, they privileged certain communication styles and overlooked others, such as non-verbal or behaviour-based forms of expression. This approach unintentionally failed to represent the diversity of communication modalities present in LTC settings and marginalized residents who may still have valuable input but were unable to express it through conventional means. An interview with a recreation team member further highlighted how resident behaviour varied widely and should be interpreted with care. She mentioned, “If some people that you see here wander off, you look at [their behaviour] and wonder why they’re walking around, right?... We've got to look into their behaviour at the time you offer [VR] because…everybody’s different.” (a recreation staff). This insight underlines the importance of creating more inclusive engagement strategies that respect residents’ diversity and recognize that communication is not always verbal.
The failure to include a broader range of residents reinforced the existing power hierarchies and constrained whose experiences shaped the co-creation process. One licensed practical nurse reflected on this challenge: It really depends on who’s there. Some residents aren’t really watching or engaging in a way that’s obvious… but if [resident name] is here, you can ask her directly what she likes. Besides her, others might not respond right away—but that might be because they aren’t given the right support or opportunity to share. (a licensed practical nurse)
This comment reveals that quieter or less expressive residents may still have meaningful contributions but require alternative forms of engagement and facilitation. Without this support, their voices risk being overlooked, reinforcing a model of participation that centres only those who can easily articulate their views. Power tensions thus further extend among residents, especially for those “not responding right away,” need more time to process, quieter and less vocal may become silenced. Their sharing opportunities may be overridden and “taken away” by residents who were able in expressing themselves verbally. This exclusion might have been interpreted as a tacit rejection of those individuals who were excluded, creating a power imbalance between the research team, residents participating in the co-creation process, and excluded residents. The ethical implications are significant, as they suggest that the current co-creation model did not address the broader perspectives present within the resident community and worsened existing power imbalances.
Group Dynamics
Furthermore, in the early co-design workshops, grouping residents, staff, and family members together created complex relational dynamics that shaped who spoke and who was heard. While the intention was to foster inclusive dialogue, the combined presence of these three participant groups revealed relational hierarchies that made it challenging to gather equitable input from all voices. The research team quickly recognized that grouping residents, family, and staff together in a single setting introduced challenges to the co-creation process, as each group’s varying priorities and communication styles often clashed.
Staff were primarily focused on the feasibility of implementing VR technologies into care routines and expressed concerns about how residents might receive such experiences. One care staff reflected on their experience, So [I] explained to her what was going on, and we took it really slow, and she likes it, you have to be very, like you were saying. You have to take your time and explain it to [residents], you can't just plop it on someone. (a recreation therapist)
This highlights a focus on staff practice, which sometimes pulls focus away from resident-led content discussions. Residents, by contrast, were most engaged in discussing the content of the VR experience that resonated with their personal interests and memories. During one conversation, a resident excitedly expressed a desire to watch hockey games: “I would like to see it like playing in a [hockey] game.” (a resident)
In the co-design workshops, family members played a supportive role, acting as mediators between staff and residents to balance the conversation without dominating. They demonstrated attentiveness to residents’ emotional and personal histories, using shared memories to guide the co-creation dialogue. One family member reflected, “I think if it’s music that is their era, it really moves them. You’ll connect them to memories and stuff like that… I know that my mom and dad used to really love [dancing].” (a family member)
Despite these moments of enthusiastic engagement, the group format often favoured residents who were more vocal. Quieter residents struggled to participate in the large-group setting, leading to fragmented conversations in which a few dominant voices shaped the discussion. In our observation, a team member noted that when more residents were present, they would often speak over each other, and combined with hearing difficulties or overstimulation, this environment may have overwhelmed some residents, making them less likely to contribute. This dynamic created a hierarchy among residents, privileging those with greater assertiveness while giving fewer opportunities to others who may have had strong opinions on the discussion topic.
This observation also held true for staff-resident interactions. Even when discussions centred on staff practice, our team members noticed that staff often stepped back to avoid speaking over residents and sometimes refrained from sharing their own insights unless explicitly invited, which shifted the conversation back to resident interests. Although they could have leveraged their healthcare experience to shape the conversation, they prioritized resident input instead. Our team members observed that staff members tended to maintain their caregiving role in the co-design workshops and focused on caring for the residents’ needs, and allowed spaces for residents to talk. They only expressed their opinions when invited by the facilitator. This may have been a deliberate attempt to reduce potential power imbalances between staff and residents. However, this self-regulation may have also led to missed opportunities for staff sharing and could have made staff feel sidelined in the co-creation process.
This theme illustrates an ethical tension in co-creation: how to balance the facilitation of resident-led engagement with the risk of unintentionally excluding others. It also highlights how power can operate subtly through recruitment practices, workshop design, and communication norms—even in participatory settings with inclusive intentions.
Perceived Autonomy and Different Levels of Knowledge Regarding VR Technology
Perceived Autonomy
The perception from residents having limited autonomy in relation to staff and research figures in LTC settings contributed to the power dynamics encountered in the co-design process. In particular, residents were sometimes hesitant to challenge researchers’ input or assert personal preferences. Researchers greatly valued residents’ perspectives and catered closely to the needs and interests of residents with dementia as part of the co-design process. In contrast, residents might tend to conform to researchers’ expectations and completely accept the VR technology presented by researchers without providing much feedback. This led to a dynamic where researchers, despite their intentions to empower residents, were positioned as de facto decision-makers. For example, this dynamic was observed during a one-on-one interview with one resident after she had tried using the VR headset for the first time: Research assistant: How do you think that we can use this for people who have dementia in long-term care homes? Resident: Well, they’ll listen to it anyway. Research assistant: They’ll listen to it anyway? Resident: Yeah. Research assistant: Do you think they’ll like it? Resident: We do whatever they [staff in LTC] do for me, we accept it [the activity staff do with residents].
This exchange illustrates how structural norms in LTC—where care is typically administered rather than co-developed—may carry over into research participation. Residents may hesitate to voice dissent or propose alternatives, deferring instead to perceived authority figures. Later in the interview, when the researchers asked whether the video was boring to receive feedback on the VR program, the resident responded in a way that felt obligated to adhere to the researchers’ expectations: Research assistant: (The resident was not showing enjoyment or enthusiasm.) Do you think the video is boring? Resident: No. Whatever you are happy with.
Furthermore, some residents were uncertain whether they could fulfill their roles in the co-creation process and offer insights to researchers, due to existing power imbalances. As a result of this perception, residents doubted whether their contribution was helpful. For example, one resident commented on the experience of participating in the co-design workshop. He said, Providing feedback is productive, and it gets the point across that you want to get across… other than that, I can’t really tell you anything more because I don't know, although I've been involved. (a resident)
To address the power imbalance among residents, researchers engaged residents in filming videos for the VR program and showed them to other residents for feedback, helping residents feel more involved in the co-creation process. According to research team reflections, personally filming videos and sharing them with other residents allowed residents to “feel a sense of pride and ownership” (a research team member’s field notes) in their contributions to the research process and in co-designing the VR program. Therefore, researchers believed that engaging residents in the filming process played an integral role in deconstructing the power challenges encountered.
Differing Levels of Knowledge of VR Technology
Differing levels of knowledge of VR technology among researchers, residents and staff contributed to potential power imbalances. Some staff members believed that VR technology could only be well-utilized by younger generations who have been exposed to technology growing up and use it more often in their daily lives. The assumption that older staff do not have the same capacity as younger generations to enjoy and use technology limits their ability to be fully engaged with the technology, they could use daily in LTC. For example, one staff member during a one-on-one interview expressed: It depends on your staff, right? Like, I have more of an aging staff. So… I don't think a lot of them would be into that, but if you got like the young people that are coming in that are a bit more tech savvy, they probably would enjoy that. (a recreation manager)
Researchers recognized that this had created a power dynamic in which the research team, consisting mainly of young university students, became the VR experts in the relationship. This could have prevented older staff from making meaningful contributions to the co-creation process. In addressing this challenge, researchers encouraged staff members to train other staff to use and facilitate VR adoption, and to take the lead in adopting VR in their workplace and in their routines with residents. For example, one of the recreational staff helped create a guide to using the VR projector, which enhanced staff confidence and enabled broader engagement. As a recreational manager shared: We’ve been using it [the projector] for a whole bunch of programs. So, not just showing small videos, but we use it for bingo. We used it when we did National Film Day, which is all across Canada. We showed our film. We've used it to show a sports event. So it's been really great having that.
Residents also expressed anxiety around using headsets, particularly when viewing content alone. Despite residents seeing the same program through the VR headsets together with other residents, the headset provides an individual experience, and residents may not see the same scenes due to different video time points. Particularly, one resident specifically stated their feelings of fear when seeing a program with fish: “So if you see the fish, and I’ve seen it. They’re huge… you think they’re gonna come at you. No, I was I was scared… But you got to have a lot of people in the room.” (a resident)
To address this concern, the research team provided a virtual reality projector as an alternative. This allowed several residents to experience VR simultaneously and to have increased opportunities for social interaction with one another. As part of a team reflection, researchers noted that projectors were well received.
Unfamiliarity With the Research Team and Process
The research team identified that a major challenge in the co-creation process was the unfamiliarity between residents and the research team, which impacted residents’ engagement, the consent-obtaining process, and the acknowledgement of participation. The absence of a pre-existing relationship introduced subtle power dynamics, positioning researchers as outsiders and diminishing resident trust and comfort. One team member reflected: “Even though we are filming in a familiar environment that the residents are in, our identity as an outsider may bring them suspicion. We would not want this suspicion to impact the meaningful co-creation and enjoyment of their time.” (A research team member). The member’s reflection highlights the dissonance between the research team’s intentions and how they were perceived by residents, many of whom were hesitant to fully engage due to the presence of unfamiliar individuals and unclear expectations.
For some residents, unfamiliarity may have prevented them from sharing their needs in favour of perceived researcher convenience. One resident remarked, “I think whichever is most possible for you, the easiest for you.” (a resident). This sentiment reflects a broader dynamic in which residents sought to reduce the burden on the research team, even when it meant silencing their own preferences. Rather than viewing themselves as co-creators, these residents valued the researchers’ judgment.
Residents’ unfamiliarity had implications beyond relationship-building and directly impacted the consent process. While some residents expressed interest in the VR component of the project, a significant number were hesitant to sign formal consent forms. This reluctance was rooted in uncertainty around the purpose and implications of the consent process. The act and the need to sign a “binding” document that uses overly complex language created a power dynamic which placed residents in a subordinate role. Some residents appeared reluctant to go through the consent form with our research team members and eventually withdrew from the VR activity before understanding the full picture of the project. After observing this in the early stages of the project, the research team reflected on how to better balance the need to obtain informed consent from residents without scaring them with the consent form and on how to obtain consent without unintentionally imposing power differences on the residents. The research team began explaining the consent form to residents in plain language. With mixed success, this strategy may not fully overcome the initial anxiety or discomfort introduced by the formal consent-obtaining process. Furthermore, the unintended consequence of difficulties obtaining consent was that residents who were willing to sign a consent form and engage with the research process had greater access to decision-making spaces and influenced the co-design process than those who did not. This suggests a more profound power imbalance between residents who are comfortable navigating formal systems and those who are not, despite both groups potentially having meaningful perspectives to offer.
The research team also reflected on the ethics of offering gifts to participants, a practice intended to express appreciation but raised concerns about potential coercion. While these tokens were small and provided as appreciation, even modest gifts might shift the dynamics of participation, creating a sense of dependency or obligation. Although the team took steps such as repeatedly reassuring residents that the gifts were to appreciate their sharing, explaining that the project was not-for-profit, and ensuring that residents knew gifts were not conditional on participation or framed as compensation, this act of gifting unexpectedly created an uncomfortable environment for some residents, making them feel obligated to participate. Ultimately, a gift from the research team could have exacerbated existing power imbalances between various partners and the team.
Discussion
So what? – Why do these ethical reflections matter for participatory research in LTC? Our research team’s reflection contributes to the underexplored “backstage” process of participatory research in technology development in LTC involving diverse partners, as well as methodological insights into ethical issues related to power dynamics in the co-design process. It adds to the growing evidence regarding the intersection of technology, co-design, and LTC.
The staff-mediated recruitment strategy in our study highlighted a critical tension between protection and paternalism. This recruitment approach may potentially reinforce paternalistic behaviours among staff and the stereotype that staff are the best advocates for residents. This reliance on staff perpetuates the assumption that residents have a declining capacity to make decisions regarding their own well-being (Seedsman, 2019). While having staff support in selecting the “most appropriate” or “well-fitted” resident participants may seem practical, it can unintentionally override residents’ agency and deprive them of the opportunity to negotiate their own risks and contribute to research activities. This reliance places staff, rather than the residents, at the centre at the first step of the research process. This may also reinforce the norm of “surrendered dependency” in LTC, in which residents comply with dependency and institutional control because they believe that staff are the sole experts and authorities (Mortensen et al., 2024).
The unintentional exclusion of voices also resulted from our limited focus on using verbal communication to exchange information in the co-design workshops. The lesson learnt to enhance the recruitment process is to encourage researchers to have an open mind (Sakamoto et al., 2023) and reimagine how the co-design process can be tailored to the population in LTC homes. This takeaway challenges traditional forms of verbal discussions in focus groups or interviews and advocates for considering other forms of expression and diverse inquiry methods, such as an arts-based approach (McArthur et al., 2023). Researchers can then accommodate residents with a broader range of capacities. Yet, it can be uncomfortable for researchers to explore the unknown and take the first steps toward adopting innovative co-design methods. Researchers can consider partnering with colleagues with expertise in different co-design approaches. They can engage these experts in project planning and participatory processes for guidance and support. Researchers need to provide more detailed documentation of engagement strategies to include people with communication challenges in LTC.
Another notable implication that emerged from our reflection is the significant role of group dynamics in the co-design process. There is no one-size-fits-all solution regarding the appropriate group structure (Wiersma et al., 2016). Although our research team tried to enhance inclusivity by bringing all partners into a single discussion group, we unintentionally imposed a hierarchy and power imbalances due to differences in priorities, communication styles, and stereotypes about residents’ and staff’s roles in a care home. This observation adds to the limited body of evidence regarding group structures and dynamics when working with people living with dementia. Current literature focuses on the complex dynamics among family care partners and people with dementia. A previous study found that in groups composed solely of people living with dementia, they could express themselves, support one another, and learn from one another (Wiersma et al., 2016). In our study, however, we observed that some residents were more outspoken and dominated the conversation. This created an ethical tension between empowering some residents while simultaneously excluding others. Unintentionally, researchers can develop a new hierarchy among residents in LTC, where only the more vocal residents are empowered and dominant. While having residents willing to contribute deconstructs the stereotype of residents as passive dependents, researchers need to remain sensitive and respond to any observed imbalances in the hierarchy of participation among residents.
In contrast to the existing literature, our study observed a “self-silencing” phenomenon among staff and family members in the group dynamics. As discussed in a recent article by Wiersma et al. (2016), the presence of care partners could sometimes overshadow the voices of people living with dementia, and individuals with dementia might choose to “self-silence” in the discussion in the presence of family care partners. In our study, when people living with dementia were present in the group, staff and family members’ sharing was limited due to their self-identified supporting role in the discussion. Family members helped translate for a resident to facilitate her participation in the conversation and reassured residents when they tried new technology in the co-design workshops. Staff also tended to “self-silence” to provide space for people living with dementia to speak. This creates an ethical dilemma between fostering inclusive opportunities for residents to share their perspectives and the protective role of staff in ensuring residents have the necessary time to speak. This dynamic reveals the persistent institutional hierarchy and the assumption that staff members’ primary role is as caregivers rather than as research partners. They prioritized the operational needs of the research and the care of their residents over sharing their perspectives. This adds to the complexity of group co-designing in LTC homes.
When planning group structures, Hsu et al. (2025) stated that researchers need to understand their partners’ backgrounds and evaluate the process and their partners’ engagement after the co-design workshops. Being flexible and responsive to observed group dynamics is crucial in the iterative process of a co-design project to optimize each partner’s participation. For example, in our co-design workshops, we started with a session with family, residents and staff together. Gradually, we adjusted to having separate staff-only sessions and sessions with family and residents together. There were also sessions with residents only, such as the co-creation of VR videos. Because of the aforementioned limitations in staff participation driven by their tendency to prioritize resident voices over their own, this change was implemented to ensure an equitable sharing environment and mitigate power imbalances between staff and residents. The researcher, equipped with facilitation skills, is needed in the co-design process to recognize the subtle development of dynamics among partners and encourage participation. Researchers can also explore strategies to manage imbalanced group dynamics and promote equitable, respectful sharing. For example, having a microphone to be an object that represents a “right to speak,” ensuring that outspoken residents do not interrupt or overshadow the individual currently speaking. At the same time, the resident holding the microphone can feel respected and at the centre of attention, and their voice can be heard more easily. Hsu et al. (2025) mentioned how researchers can moderate dynamics in group discussions. In our study, we showed how researchers could deconstruct power imbalances stemming from the traditional marginalized and underpowered role of residents by centring residents’ voices and ideas in co-creating videos. It echoes another reflection paper on co-designing technology with people living with dementia, which argues that researchers should clarify partners’ roles in the co-design process from the project’s initial stage (Sakamoto et al., 2023).
Furthermore, we found that the feeling of unfamiliarity with components of the participatory research process in LTC, such as the use of technology and obtaining informed consent, can exacerbate power imbalances in co-design partnerships. Our research team provided the equipment and orientation to allow participants to use and understand how the technology worked before the co-design workshops and the adoption of VR technology. This preparation helped connect the partners with the technology, made them more comfortable driving the VR co-design and adoption, and empowered them to engage with the explored technology (Sakamoto et al., 2023). Our reflection noted that collective experience with technology can help reduce residents’ fear and unfamiliarity with it. It is essential for researchers conducting technology co-design research to find ways to prevent technology from becoming a barrier to the co-design process.
The team’s reflection on obtaining consent in LTC reiterates the need to critically examine the current consent process and documents, which can be rigid and use dense, unfamiliar language for lay people, such as residents. The overly complicated presentation of information can create a power imbalance between researchers and participants, potentially disengage participants from processing the information on consent forms or even make them reluctant to participate. A previous study reported that a resident was suspicious of the consent documents due to past experiences with the bureaucratic system, which caused the resident’s distress (Balkin et al., 2023). In participatory research, it is essential to ensure that residents and partners understand the research process, its purpose, their roles in the research, and their right to withdraw through the consent process. However, the consent form created ethical dilemmas and power imbalances rather than alleviating them. The lengthy consent forms became a barrier to relationship-building between the research team and residents, a key aspect of participatory research. Rather than adopting a generic format, researchers need to understand the context and tailor the consent documents accordingly. It is worthwhile for researchers to work with the research ethics board and collaborators from outside the field to adapt consent forms using creative approaches, such as lay language and graphics (Fields & Calvert, 2015). It is also essential to understand participants’ priorities and which information is most meaningful to them (Diaz et al., 2025). Tailored consent forms can enhance the inclusiveness of the consent process, improve partners’ understanding, reduce feelings of intimidation, and foster relationship-building with the research team. Scholars also suggested the process consent method, in which the researcher can learn about the person’s preferred way of receiving information and revisit the consent content before and/or during each research activity if needed (Dewing, 2007; Diaz et al., 2025). This ensures the persons living with dementia can have ongoing decision-making power and recurring opportunities to ask questions regarding their involvement or withdraw from each research activity throughout the study.
The research team should also consider how they acknowledge the partners’ efforts in LTC. In a scoping review of the engagement of people with dementia in research (Bethell et al., 2018), only a few studies discussed the ethical dilemmas surrounding compensation for their contributions. There have been different opinions regarding ways of recognition in other research fields. Recognition can be seen as a form of coercion, and the partners might feel obligated to participate in the research. However, with little or no recognition, this can also be viewed as researchers exploiting partners (Millum & Garnett, 2019). In the case of LTC research, monetary appreciation can be appropriate for staff and family members. However, this token of appreciation may not be suitable for residents who cannot leave the care home and use the money. Alternatives, such as gifts of equivalent value to the monetary token of appreciation, could be offered to residents. Researchers can also discuss and decide with residents on their preferred form of appreciation. In our study, the residents were also concerned about why the research team gave them gifts. From an anthropological perspective on gift-giving, our tokens of appreciation can unintentionally trigger the recipient’s (the resident’s) social obligation to “reciprocate” (Sherry, 1983). Researchers should also be mindful that their acts of gifting do not place residents in an inferior position when they feel they have nothing to “reciprocate” (Sherry, 1983). We might thereby impose a power imbalance, unintentionally reproducing and exacerbating the institutional hierarchy in LTC, especially for residents who often have limited resources to give back. It is crucial to reiterate that the token of appreciation does not obligate the partners to participate in the research. The gift represents respect and appreciation for their time and for sharing experiences. Researchers should also consider the place and context in which they give gifts to residents (Sherry, 1983). For example, presenting the token of appreciation in a public common area versus the resident’s private room could influence how residents interpret the researchers’ intent and the gift’s symbolic meaning.
Implications
Now what? – What actions should be taken?
Based on the reflection and analysis, our team summarized the lessons learned to mitigate power imbalances for future research practices for participatory research projects and co-designing technology in LTC settings. These lessons learned serve as a practical guide to encourage researchers, including family, staff, and residents to be accountable in facilitating equal participation and autonomy and fostering equity and inclusivity in participatory and technological co-design research with individuals with dementia in LTC.
An Actionable Acronym - PARTNER
Strengths and Limitations
The reflexive, interdisciplinary approach strengthened the analysis by enabling multiple interpretive lenses and sustained critical interrogation of power relations. This collaborative reflection ensures richer interpretation and methodological rigor. Despite the strengths, we acknowledge several limitations. The first limitation is about the use of the Rolfe’s et al. (2001) model of reflection as our guidance. Its three guiding questions are broad, allowing flexibility and depth in reflections. However, the openness might have introduced interpretative biases, as the model’s application requires input and guidance from senior researchers and interpretations by trainees. The second limitation is about our methodological limitations. Although our team practices reflexivity and constantly challenges each other’s assumptions throughout the study, there might still be unidentified “blind spots” and biases. The presence of unconscious biases among our team members, stemming from prior clinical experiences in healthcare settings and social norms from diverse cultural backgrounds, might have affected their reflections and understanding of hierarchical power dynamics in LTC settings. Furthermore, the study was conducted in two LTC homes in Vancouver, Canada. The specific care homes have their own unique organizational culture and power dynamics. These findings may not be transferrable or relevant to LTC settings in different geographical and cultural contexts. Lastly, although we engaged a patient partner living with dementia in the analysis and editing of this reflection paper, we did not include any residents or frontline LTC staff in the writing process. Thus, we might have missed perspectives that could have enriched the content and depth of this critical reflection.
Conclusion
This reflective paper offers methodological and ethical insights drawn from our participatory research to co-design a VR program in LTC, involving residents living with dementia, family care partners and staff members. By surfacing the underexplored backstage processes of co-designing technology in LTC, including the unintentional exclusion of resident voices, power dynamics related to technological unfamiliarity, and the ethical dilemmas of recognition, this paper contributes to a growing body of work critically examining how participatory ideals unfold in practice. Our analysis reveals that even well-intentioned participatory processes can reproduce structural inequities if power dynamics remain unexamined. Based on the critical reflection, we identified key tensions and developed the PARTNER lessons learnt to support more inclusive and ethically responsive co-design practices in LTC. We call on researchers to document not only outcomes but also the complexities, contradictions, and negotiations inherent in participatory research. Future research should continue to explore and share diverse strategies that support equitable engagement in co-design, especially in the context of aging and care.
Footnotes
Acknowledgments
We would like to acknowledge all residents, family members, and staff who participated in the Virtual Immersive Program (VIP) project. We would also like to acknowledge our family partners, Lily Wong and Christine Wallsworth, and student trainees who were part of the VIP research team.
Ethical Considerations
Our study received ethics approval from the UBC Behavioural Research Ethics Board (H23-01481).
Consent to Participate
Written informed consent was obtained from participants prior to participation, with the purpose and details of the study discussed. Verbal consent was sought before each of the co-design activities. All participants in the study were reminded about the purpose of the research and their right to withdraw at any time.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by Alzheimer Society of Canada (F22-05011).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.