
Abstract
In 2023–2024, we conducted a qualitative study on palliative care among Israeli-Arab end-of-life patients, following ethical approvals at our university and in the participating hospitals. The study was conducted by a female Muslim Israeli-Arab Ph.D. student and supervised by a male white Jewish professor. Yet our cultural differences led to methodological and ethical challenges and tension. Over time it became clear that such obstacles could not be adequately addressed through “common” practices of reflection and positionality. To achieve a more refined understanding of the challenges and their impact on the researchers, the participants, and the research at large, a culturally-responsive research approach was applied. Following the critical advocacy research design, this study analyzed the major challenges and solutions associated with conducting this research in Israeli-Arab society. Situational-analysis methods were used to interpret and understand the data. Based on a five-stage analysis, four major themes identified: Facing death and choosing research; relationships with participants and other related stakeholders; conducting interviews and feeling bound (or supported) by ethical guidelines; and supervisor-student relationship. Discussing these themes provides a rich understanding of these challenges and of the concept of death and dying in Arab society. The achieved micro-, meso-, and macro-level insights advocate for change and further action in academia and research ethics concerning sensitive qualitative studies.
Introduction
Conducting qualitative research with participants at end-of-life (EOL) may be both challenging and rewarding for researchers and participants. This type of sensitive research (Alexander et al., 2018; Dickson-Swift et al., 2006) entails the exploring of delicate, complex, and often controversial issues that these vulnerable individuals must deal with when they may feel time is limited and precious. Additional complexity emerges when the research population consists of minoritized communities, whose beliefs and practices differ substantially from the white, western, colonial, and liberal traditions-of-thought that are often perceived as the norm. Such tension can be especially observed when dealing with palliative care, which provides relief and symptom management, enhances dignity and quality-of-life, and supports EOL patients and families (Kitchen et al., 2024).
The term culture refers to the shared experiences of individuals, including language, values, customs, beliefs, and morals, as well as to their world views and means of knowing and communication (Jordan & Hall, 2023). Culture plays a meaningful role in coming to terms and coping with illness, while preparing for death (Cain et al., 2018; Gysels et al., 2012). As such, the combination of minoritized communities, cultural issues, and EOL renders research on this topic highly sensitive and challenging. For example, some minority groups receive more aggressive treatments at the EOL and use advance care planning less frequently due to cultural taboos around discussing death. These taboos may stem from the perception that speaking on death may trigger misfortune or contradict religious faith, particularly in the Arab, Asian, and South Asian contexts (Kwak & Haley, 2005; Natour Hleihel & Sperling, 2025). Family rituals and involvement heavily influence care decisions. In some communities, collective family-based decision-making overrides individual autonomy, and adult children or extended relatives are entrusted with EOL choices (Bullock, 2011; Natour Hleihel & Sperling, 2025).
Moreover, in such cultural contexts, religious and societal norms often inhibit open conversations about dying. Talking explicitly about death is sometimes perceived as a sign of despair, spiritual weakness, or even a provocation of fate (Sayid Ahmad & Peled Raz, 2025; Natour Hleihel & Sperling, n.d.). Euphemisms are often used in Arab communities to avoid direct references to death or dying (Abdessamad, 2024). Instead of explicitly saying “death” (الموت), people may use softened expressions like “God’s decree” (قضاء الله) or such as “God’s will” “مشيئة الله” or “when the time comes” “عندما يأتي الأجل” often replace direct terms like “death” or “dying.” These cultural codes are reinforced by communal expectations to preserve hope and emotional stability, particularly within close-knit family systems. Such dynamics can foster internal tension, guilt, or hesitation when faced with decisions about PC at the EOL, especially when such decisions are seen as a form of “giving up” (Abdessamad, 2024). Despite growing awareness of the importance of culture in EOL care, healthcare providers often lack training to address these cultural differences, limiting culturally appropriate care (Glyn-Blanco et al., 2023; Natour Hleihel & Sperling, 2025.) Specifically, research among palliative care professionals has identified insufficient training, language and ritual-related barriers, and organizational constraints as significant obstacles to delivering equitable care (Cáceres-Titos et al., 2025; Coombs et al., 2022).
Understanding this cultural backdrop is crucial, as it significantly shapes the way Arab patients and families interpret, postpone, or reject referrals to PC at the EOL. Decisions often framed not merely as medical choices, but as existential, spiritual, and communal ones (Al-Harrasi et al., 2025).
According to the reflexivity concept developed by scholars from the global majority (Berger, 2015; Sword, 1999), researchers hold a prior beliefs, values, and experiences that impact their decision to undertake the specific research, their motivation to pursue the research plan, their understanding of interactions with the participants, and their approach to the data analysis. Both authors hold the ontological position focusing on how the research participants perceive and make sense of their finality (or that of their patients), the decisions that they must make in these moments, and the rich context that impacts the researchers. We also hold an epistemological view, whereby identifying and understanding the participants’ experiences and perceptions, and the meanings that they attach to them, can be achieved through their individual interpretation and shared construction of meaning created by both participant and researcher (Clair, 2014).
DS, the first author of this article, is a white, middle-aged, Jewish cisgender man, a bioethics university professor with vast experience in qualitative research. The second author, NNH, is a young Muslim-Arab cisgender woman who is conducting her Ph.D. research in nursing, under the supervision of DS. NNH’s research focuses on EOL in Arab society through in-depth interviews that are conducted with terminally ill patients and with healthcare professionals, based on the interpretive phenomenological approach (Gephart, 2018; Larkin et al., 2009; K. A. Lopez & Willis, 2004). The aim of these interviews is to explore and understand the participants’ beliefs and perceptions regarding access – and in turn, referrals – to palliative care at EOL, specifically within the Israeli-Arab society, encompassing Muslim, Christian, and Druze populations. In her comprehensive mixed-methods study, NNH also uses quantitative questionnaires for examining relationships between religion, religiosity, anxiety regarding death and dying, and the intent to seek (or decline) palliative care among members of the Israeli-Arab population in general. Yet this is beyond the scope of the current article. After the research proposal was reviewed and approved by two external reviewers, it was submitted to the ethics committee at the researchers’ academic institution and to the institutional review boards (IRB) at the participating hospitals. As is commnly required in the research application, we elaborated on the possible risks to the participants and their families following their participation in these interviews, such as feeling emotional distress by the introduction of some of the questions or being asked to reflect on death and dying issues that might be unspeakable.
We also addressed ways for mitigating these risks, or helping participants overcome them, should such risk occur, for example informing them of the option of referring to the hospital social worker or a relevant patient organization for further help and advice. Data collection started immediately after the ethics approvals have been granted. No other contact with the ethics committees has been made since then, nor was it required by them.
To recruit healthcare professionals for interviews on their views of EOL, NNH used convenience, purposive, and snowball sampling. Yet the task of recruiting terminally ill patients was more difficult, due to their serious medical condition, the possible objection of their families, and cultural issues affecting the extent to which patients are informed of their medical condition in the first place and shaping one’s decision as to whether to speak on death and dying at all. To overcome such obstacles, the recruitment process was facilitated by medical professionals and social workers from the participating hospitals.
Four inclusion criteria were applied in this study, whereby the patient was: (1) at least 18-years-old; (2) a member of the Israeli-Arab society; (3) literate in the Arabic language; and (4) declared terminally ill under the Israeli Dying Patient Act 2005 (with a life expectancy of up to six months). After identifying such patients and obtaining their informed. She then travelled to the hospital to conduct the interview as quickly as possible. At the time of writing this article, we had conducted interviews with 11 terminally ill patients (as well as with 10 physicians and 16 nurses). With each participant’s permission, we recorded and transcribed the interviews. DS asked NNH to write a reflective diary, expressing her thoughts, comments, and emotions regarding the general research process and the specific interviews – in line with the bracketing method (Tufford & Newman, 2012). Writing this diary helped NNH to separate her personal experiences from the broader picture explored throughout the research. Moreover, writing the diary enabled DS to provide NNH with more specific and relevant feedback, especially as he did not attend the interviews.
As the research progressed, we met periodically to discuss the research and address NNH’s reflective diary. NNH frequently spoke of the challenges that she faced in executing the research plan. At first, we perceived these challenges as being expected and appropriate. Yet over time, it became clear that a broader perspective for reflecting upon these challenges was necessary – as was the need to incorporate and critically examine the cultural dimensions that were present in these challenges. This was an especially important insight, as these challenges had not previously received focused attention during our discussions or IRB submission yet were hidden and underscored in our more general understanding and reflective processes.
To better understand, contextualize, and manage these challenges, we employed the concept and methodology of culturally-responsive research (CRR). Doing so enabled us to reveal and reflect on new challenges as they arose, while relating to issues that had already been addressed through “ordinary” prism. The CRR methodology strives to embrace cultural and epistemological pluralism, while deconstructing western colonial traditions of research, holding the veil of objectivity and value of neutrality (Zhao et al., 2025), and serving the interests of the economically powerful (Jain et al., 2025); this approach also recognizes the primacy of relationships within power-sharing dialogical encounters (Berryman et al., 2013). CRR, whose roots lie in critical theory (Freire, 2020) and in Kaupapa Māori frameworks (Bishop, 1996), holds that the manner in which the research is conducted is of great importance. Specifically, the process through which knowledge is produced is imperative for performing actions that transform society and its institutions, while objecting to (or reinforcing) oppressive systems (Gilbert & Pasque, 2023). CRR also acknowledges that cultural dimensions, which exist in all phases of research, should be leveraged for promoting meaningful engagement through both theory and practice (Jordan & Hall, 2023; Lindsay Nurse et al., 2021; Pasque & Alexander, 2022).
CRR addresses the needs and concerns of diverse populations from a racial, ethnic, linguistic, and economic perspectives (Lindsay Nurse et al., 2021). By promoting diversity, equity, inclusion, and cultural respect, CRR promotes social justice and community empowerment (Hall et al., 2023); yet this approach also requires researchers to be responsive toward cultures, namely to engage in relationships with cultural communities. This includes actions such as analyzing contexts and examining sociopolitical assumptions (i.e., reflexivity); integrating the participants’ culture (i.e., responsibility); developing culturally-sensitive data-collection tools (i.e., receptivity); and establishing a culturally-responsive review panel (i.e., responsibility) (Jordan & Hall, 2023; McBride, 2015). The aim of the study presented in this article, therefore, is to explore, provide a better understanding, and indicate the need for change regarding the challenges that stem from conducting culturally-sensitive research on EOL (in this case, in the Israeli-Arab society), designed and analyzed through CRR.
Methodology
Research Design
In line with the CRR approach, this study follows the critical advocacy research design (Pasque & Carducci, 2015). This research paradigm draws on critical social theories and on qualitative methodologies for producing ideological and transformative knowledge. It is also inspired by the sociological writings of Bourdieu, who claimed that the primary contribution of social scientists to society is to illustrate the mechanisms of domination, while demonstrating how they reproduce social inequities (Shields, 2016). In this approach, the researcher is perceived as an engaged advocate for those whose voice is not clearly or adequately heard. Through their advocacy role, the researchers shift from an objective observer to an agent of change (Pasque & Carducci, 2015).
Procedure
We began our research by claiming our own identities (the overall way by which we define ourselves) and sharing our experiences and beliefs regarding death and dying, sanctity-of-life versus quality-of-life, the role of family and individuals in society, and the meanings that we attach to palliative care. The purpose of doing so was threefold: (1) to share our cultural knowledge on these issues; (2) to declare and examine our roles as researchers and as Ph.D. student/supervisor; (3) and to directly challenge the appearance of our being neutral, powerful/powerless, dependent/independent, experienced/inexperienced, and knowledgeable/unknowledgeable of each other. We vowed to constantly re-examine and reflect on these perceptions as the study progressed.
After conducting some interviews, and in line with the critical advocacy research design, NNH was asked by DS to answer the following questions in writing: (1) What were your major challenges as a Muslim-Arab researcher who is conducting a Ph.D. study on palliative care in the Israeli Arab Society? and (2) How did you address and manage these challenges? The questions were phrased in such a way as to reflect on NNH’s minoritized culture, with the potential of reflecting on any potential change in areas that directly arose from the research. NNH was asked to provide an open, honest, detailed, reflexive and – wherever possible – uncensored responses to these questions. She was not given any instructions as to which of the challenges that were previously discussed in the routine mentorship meetings with DS, to focus on, nor was she limited by time or space.
Six weeks later, NNH produced a 10-page report in response to these questions, organized in five headings and a summary chapter. The report was read and re-read by DS, who added comments throughout the document, asking for clarifications and further information. Two weeks later, NNH submitted a revised 13-page report. The data and insights presented in this article are based on our analysis of this in-depth report.
Data Analysis
Inspired by Gilbert and Pasque (2023), this study applied situational analysis methods (Clarke, 2005; Clarke et al., 2017) for interpreting and understanding the data presented in the report using critical frameworks. In line with the critical advocacy approach, whereby every research study must be examined and understood within its own specific context, situational analysis focuses on the situation of inquiry as the ultimate unit of analysis. Such analysis offers three major cartographic approaches as maps: (1) situational maps, that present the main situational aspects in research (major human, non-human, discursive, historical, symbolic, cultural, political, and other) and encourage analysis of their interrelations; (2) social worlds/arena maps, which offer meso-level interpretations of the inquiry situation, in relation to collective actors, key non-human elements, and the arenas in which commitments and discourses take place; and (3) positional maps, i.e., the main positions that were taken (or not), representing the full range of discursive positions when addressing a certain issue. By specifying and emphasizing the non-human elements in a given situation, this approach enhances the visibility of significant materialities and discourse from the onset of the analysis.
In this study, “non-human” specifically refers to material and discursive elements such as the physical space of the hospital room where interviews were conducted, and prevailing gender norms including restrictions on physical contact, prohibitions on mixing men and women together, and adherence to modest dress codes particularly relevant when interacting with religious patients. These factors critically shaped the research process within the conservative Arab-Muslim or Druze context.
Mapping the data in this manner. Situational analysis was an appropriate method for this study, enabling us to empirically construct the situation of inquiry; in addition to it corresponding with CRR, it also allowed us to uncover and reflect on various intricacies that were related to the main research, while paying attention to the DS-NNH mentor-mentee relationship and to NNH’s relationship with the participants. This approach provided a rigorous and trustworthy method for analyzing the challenges that were reported by NNH under CRR.
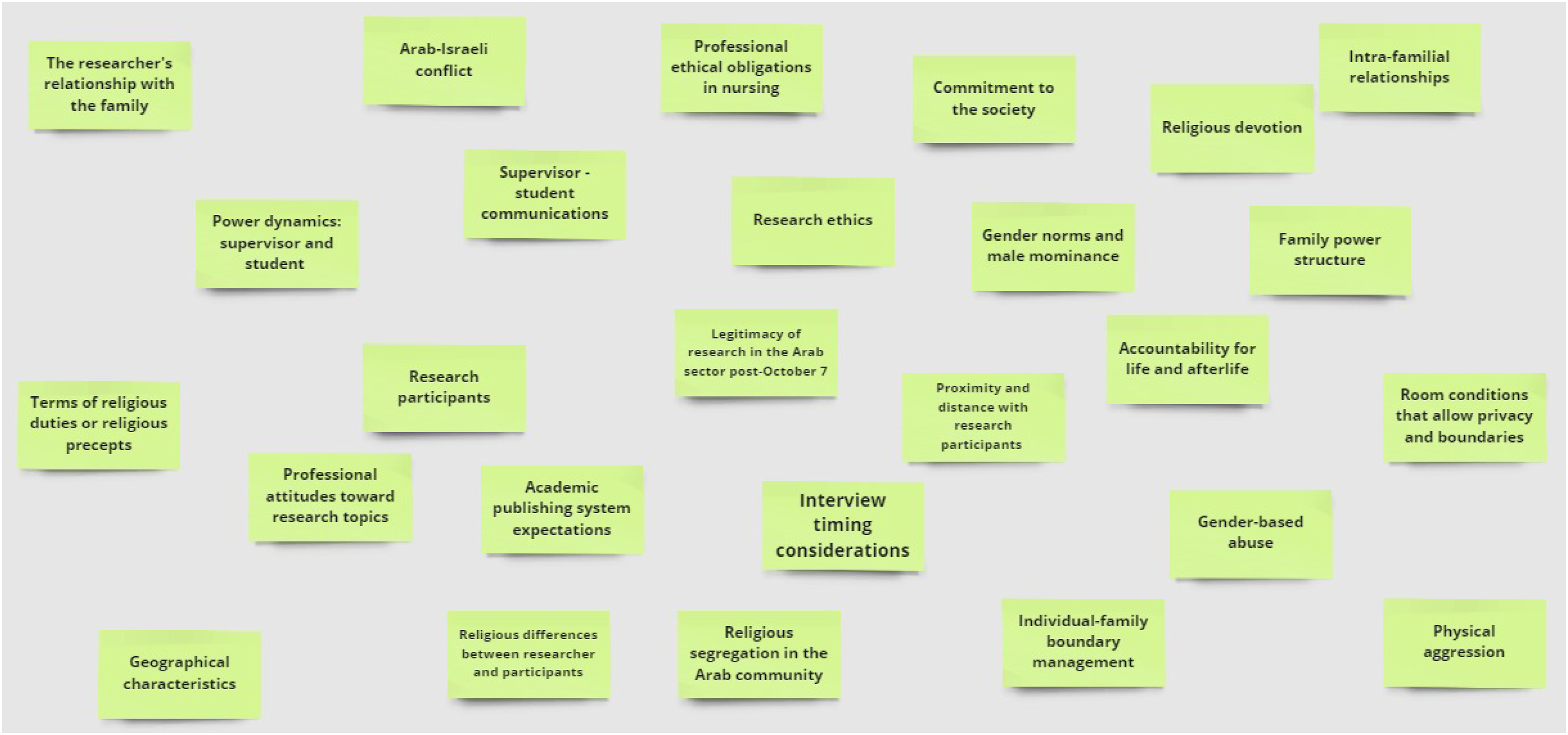
Both authors engaged in the analysis of NNH’s report, independently and jointly, through ongoing dialogic reflexivity. The analysis consisted of five stages: (1)We read and re-read NNH’s revised report regarding the challenges that she had encountered as a Muslim-Arab Ph.D. researcher who was interviewing terminally ill patients and healthcare professionals from the Israeli-Arab society on the topic of death and dying; (2) Similar to traditional open coding, each researcher created a messy abstract situational map using the MIRO Application (miro.com/app). No instructions were given regarding the format, order, or rules for creating this map, or the terms and concepts from the report that should be included on this page. We then combined our maps into one using two different colors, one for each researcher. At this stage, we were aware that differences would likely be seen between the two combined maps due to our different cultural backgrounds. (Annex 1). We then asked questions about the various aspects that appeared on the page and their interrelations; (3) We color-coded the various entries and added arrows between them, similar to axial coding. This allowed us to create a more advanced situational map – an abstract relational map (Annex 2); (4) We asked questions about the abstract relational map. The aim was to explore social arenas that were involved in the entries, examine relationships between them, refer and identify collective players and non-human elements, and explore the related discourse. Throughout this detailed process, we inquired about cultural, symbolic, political, economic, power-oriented, spatial, and temporal aspects. We then created a new map – a social world/arena map (Annex 3); (5) Building on our earlier separate and joint analyses of the various immediate aspects identified in the report and their interconnections, this mapping enables us to conceptualize broader themes and topics that are socially and politically constructed through a deliberative process. Visualization of Coding Maps from Two Researchers Relational Map of Coded Concepts Social Arenas Map : Entities, Relations & Discourses.

These four in-depth stages enabled us to determine the most relevant and meaningful elements that emerged from the report. In the fifth and final stage, these were then defined as the major challenges and controversies and a new map was drawn. The map was organized along two axes: the x-axis, a continuum of the major challenges, controversies, and concepts – ranging from the least responsive to the most responsive cultural issues; and the y-axis, a continuum that ranged from the least contradicting or violating the researcher’s cultural beliefs and sense of affiliation to the least adhering to and promoting the researcher’s cultural beliefs and sense of affiliation (Annex 4). Reviewing all of these maps facilitated the construction of our major findings, in line with the CRR approach. Below we describe our findings along with reference to various interactions with participants from the original research using pseudonyms. Dual-Axis Concept Map of Major Challenges & Cultural Continuums
Findings
Following this five-stages analysis, four main themes were identified: (1) Facing death and choosing research; (2) Relationships with participants and other related stakeholders; (3) Conducting interviews and feeling bound (or at times, supported) by ethical guidelines; and (4) Supervisor-student relationship.
Facing Death and Choosing Research
NNH was born and raised in the city of Shefa-Amer in northern Israel, which she described as “a village in the disguise of a city.” When she was 26, NNH moved to Jerusalem, which differed greatly from the small, conservative, Arab village in which she had grown up. Following this move, she experienced a serious culture shock, as she realized that many of the values that she had been raised on were frowned upon. In her village, modest dress was the cultural norm, staying out late at night was discouraged, and being seen in restaurants or public places during late hours was frowned upon. Bars and nightlife venues were considered inappropriate, particularly for women. In contrast, the urban environment of Jerusalem presented more liberal social norms, making her feel that her behavior and appearance which were once considered respectable were now perceived as outdated or overly traditional.
One of the most significant changes NNH experienced involved personal autonomy. In her original cultural context, decisions such as when to leave the house, where to go, and with whom were often made collectively, with the involvement or approval of family members. In Jerusalem, however, she had to learn how to make independent choices. While this autonomy brought new freedom, it also created emotional discomfort. She often struggled with the idea of not sharing every detail with her family, fearing it would be seen as secrecy or rebellion. The deep family involvement she was accustomed to made this shift especially difficult.
NNH also faced challenges in adapting to new interpersonal norms. Back home, she was taught to offer help without expecting anything in return, to be generous and selfless, and to always show respect to people in positions of authority. For example, addressing professionals formally using titles like “Doctor” or “Professor” was a sign of respect. In the urban, academic environment, however, she was sometimes viewed as overly formal, submissive, or even naïve.
These experiences illustrate the internal conflict she faced in reconciling her deeply ingrained cultural values with the norms of a more liberal and academic society. The tension between maintaining her identity and adapting to new expectations became an ongoing process of negotiation, self-reflection, and growth.
This cultural tension took an emotional toll, she lacked support and 6 months later, returned home. Yet this period greatly changed her outlook on life, and over time, she became more critical of her own society. A year later, she moved to Jerusalem again, where she continues to reside today, 14 years later.
When her father became terminally ill, she felt herself reverting to her original values and cultural beliefs; she cared about what people would think of her, and whether the decisions that she made for her father in his EOL would contradict the Islamic religion. She fluctuated between being liberal and autonomous (as her Jewish friends said, “let it go,” “let her father rest,” and “don’t make your father or your family suffer any more”) to adhering to the beliefs that she was raised upon (“You did the right thing by not speeding up his death” and “You didn’t give up on him and God will reward you for being so good to your father.”) A few days after placing a do-not-resuscitate notice beside her father’s bed, and even though she knew that her father was dying, she took it down and ripped it up. NNH admits that in the end, she acted in line with her inherent cultural values. As she said, “I insisted on talking to him so that he wouldn’t be afraid. I tried to protect him, placing the Koran beside him in the hope that this would calm him down.” Yet she also wrestled with her inner voice that accused her of giving up on her parent, a voice that asked her what she would be able to say to God when her judgement is held; she was worried about how she would be perceived by her society.
While NNH was regarded by others as a devoted and loyal daughter, this internal conflict lived on inside her, mainly: Should she have done more to prolong her father’s life despite his known prognosis? It was this conflict that led her to embark on this research, in the hope that she might be able to help other people in this situation, easing their EOL decision-making while respecting their cultural norms. Yet her decision to pursue a Ph.D. on palliative care in the Israeli-Arab society was met with suspicion, and even with a certain degree of hostility; people often asked her why she had chosen this specific topic rather than so many other potential research topics. However, NNH continued along this path, feeling confident that she was doing the right thing – for herself and for society.
Relationships With Participants and Other Related Stakeholders
This was the largest and perhaps the most compelling theme and as such, has been divided into two sub-themes.
Relationships Prior to Meeting the Participant
NNH’s relationships prior to meeting the participants can be further divided into imagined relationships and her actual relationships with them. She needed the collaboration of the medical staff at the hospital to recruit the patients for the interviews; yet they were not always happy to help her with this task. As a result, she often felt tension between herself and these professionals. This tension was deeply rooted in cultural and institutional dynamics. Within Arab society, discussing death, especially with the patient directly, is often considered taboo, as it may be seen as inviting death, violating family boundaries, or showing a lack of faith in God’s will. In this context, healthcare providers are not merely medical professionals but also cultural mediators who often adopt a protective approach toward patients and their families.
These institutional barriers, in turn, led to complex relationships between herself and the patients, as she imagined them before the interviews. For example, a Jewish physician in the palliative care services of one hospital said to NNH: “You’re not thinking straight. Do you think it’s easy? Do you really think that the family will let you interview the patient? You do know that in many cases, the patients don’t even know that they’re dying.” A similar response was received from a head Muslim-Arab nurse at another hospital: “If you want to be slapped, then why not? We’ll call you for interviews… You’ve no idea what’s going on. The families are really violent on this issue. Just leave it alone.”
NNH recalls the first time a hospital called her, saying that they had arranged an interview for her. The hospital social worker told her that Gamal, a 60-year-old Muslim-Arab man, had just been told that there is nothing more the doctors can do for him. He was in a very bad state but he had agreed to be interviewed. After waiting for quite a while to receive such a phone call, NNH was flooded with many questions: She wondered whether the patient understood what the research was about; how he and his family would react to her; how he understood his medical prognosis; and would they be able to touch upon sensitive issues, given the location of the interview. NNH was extremely nervous, yet at this point, her thoughts and questions were mainly research-oriented, and she did not share them with anyone.
Relationships With the Patients During the Interviews
When NNH arrived at Gamal’s bedside, the patient was looking very tired. He had lost all his hair and was pale, due to the radiation treatment that he had received. He began by talking about his mother, who had died several years earlier. He cried and said, “For me, my mother was the air that I breathed.” NNH felt overwhelmed: I felt desperate, filled with emotions. I wasn’t sure if I should or could physically embrace the patient, as such contact between men and women is forbidden in the Islamic religion (Negiah). I ran out of the room to bring him a glass of water and some tissues; this may have been a type of escape mechanism, allowing me to calm myself down and “press restart” – especially as the patient’s words triggered memories of my father's death.
Slowly but surely, NNH began to connect with the patient. She felt that it was their shared culture and religious beliefs that had facilitated this. They talked about his religious customs and practices, and he said that he felt safe to meet God. He talked about all the good things that he had done throughout his lifetime, how he had never hurt anyone, so he was at peace and he wasn’t afraid of dying. After a long and meaningful conversation, the patient conveyed his gratitude towards NNH, saying: “Bless you for this conversation. I’ve never had anyone to talk to about these issues up until today.” Upon reflection, NNH perceived this interview as very meaningful; she felt that it had extended beyond the realm of a mere interview, beyond the scope of her being a nurse and researcher. She felt privileged to have participated in such discourse with a person at EOL. She felt that she had strengthened him. NNH’s reflection of the interview also highlighted her active role in the conversation, as she was able to discuss: I reflected to the patient how my creed fits together with his discourse, especially as I insisted on strengthening him through the Koran, citing various cultural quotations and other aspects of Islam that he found comforting. This experience really made me feel like I had done some good. Even though I was exhausted by the end.
Another meaningful interaction occurred between NNH and a 35-year-old Muslim woman, Raaifa. After being diagnosed as terminally ill, her husband sent her and their young children to live back with her parents. NNH was very upset when she heard this, saying: “I was so angry with the patriarchal Arab society, and I really felt sorry for her.” Raaifa told NNH that she would do anything to fight and stay alive for her children. NNH was very much touched by Raaifa. Throughout the interview, NNH held Raaifa’s hand, and with her consent, hugged her. Upon leaving the patient’s room, NNH felt physically distressed (“I felt a heaviness and tightness in my chest”) and needed to sit quietly for a while, contemplating everything they had discussed.
Yet from NNH’s point-of-view, not all interviews were as successful. For example, when she went to interview Bassam, a 40-year-old Christian Arab, he was lying curled up in bed, hooked up to an intravenous infusion, all skin and bones. His 8-year-old daughter and another relative were sitting beside him. When NNH entered the room, the patient looked at her as if to say, “Come on, seriously?! I’m on pain medication now.” He told her to come back later. 30 minutes later, the interview began. At that point, Bassam turned to her and said, “Do you really think I should be spending my last days on earth taking part in a study? Just let me die in peace. If you really want to, you can interview my relative. He knows everything about me.” NNH remembered this sentence as being very difficult for her. She felt disgrace because she understood his perspective; she was sure that during her father’s last days alive, she would not have wanted to speak to anyone about death. NNH even said: “I would have worried that participating in such an interview would bring us bad luck.” It made NNH revert to the doubts and negative feelings that she had experienced at the onset of her research; she felt that she had no one to share this with.
An additional complex interaction occurred during an interview with Ebrahim, a 38-year-old Druze man. NNH was very curious to interview him, to discuss reincarnation (a belief held by Druze religion), and to learn whether such a belief is beneficial when facing imminent death. Ebrahim was very tall and extremely thin, with piercing blue eyes that seemed almost hollow, “reflecting deep fatigue and emotional strain.”
He looked like a skeleton. His gaunt face resembled a skeleton. His head and neck were completely covered by a black hat, hiding the hair he had lost. NNH felt uneasy because of the tone in his voice and the intensity of his gaze. She began the interview by gently explaining the research aim, aware that the Druze Society is very conservative.. At one point, NNH asked Ebrahim if he believed in miracles. Hearing this, he slammed his fist on the table and shouted: “Why do you speak of miracles? I’m not going to die. I’ll do anything.” NNH felt terrible: I sat frozen in my chair, trying to digest what had just happened. When I attempted to speak again, he simply silenced me, shouting, mumbling about our research and cursing us, “This nonsense.” He was so distressed that the social worker took him to see the physician on the ward, while I packed my belongings and… I felt awful. I was also afraid that he’d walk out of the doctor's room and do something to me. Or that maybe his family would. I got into my car feeling very upset. I hadn’t meant to hurt him. These feelings accompanied me for many days, even until now.
In another case, NNH interviewed Daalil, a 65-year-old Muslim man. A few minutes into the interview, his wife, Nihal, wearing a black hijab and jellabiya (the traditional head and body coverings that are worn by Muslim women for modesty purposes), burst into the room and said, “I’m his wife. I want to be present in the room.” NNH asked Daalil if they could continue with his wife in the room. He agreed, he may have felt somewhat uneasy speaking alone with a woman, appeared more at ease once his wife joined the conversation. The interview resumed, with his wife attempting to dominate the conversation and answer questions on her husband’s behalf. NNH felt that Nihal was going to be present during the interview – with or without NNH’s agreement. NNH perceived this interruption, interference even, as being related to the patient’s cultural norms. She also felt that agreeing to the wife’s presence could be beneficial for research purposes: Maybe it’s because for Muslims, a man and a woman who are not immediate family are forbidden from being alone in a room. Moreover, in Arab society, the family is very involved – often even making decisions on behalf of its individual members. I really wanted this interview to take place, so I didn't impose any conditions.
Yet this was not the only interview in which challenging situations occurred due to the presence of family members. In one case, the participant’s son was also present in the room. This man was very tall, broad, and bald, and throughout the interview NNH felt like he was assessing her “from above,” as she sat in a chair beside the participant; his body language also conveyed a sense of physical threat, as if to warn her to be careful about the questions she wants to ask his father.
Although NNH was aware of the importance of family presence in Arab society where decision-making is often collective and family members are deeply involved in medical matters the initial protocol, developed in consultation with her academic supervisor from a different cultural background, assumed that interviews should be conducted with patients alone to protect privacy and autonomy. However, incidents such as the assertive presence of Daalil’s wife and the dominant body language of another participant’s son highlighted a strong cultural norm: that family involvement is not only common but often expected. These experiences reshaped NNH’s approach, reinforcing the understanding that excluding family members might not only cause discomfort but could also be perceived as culturally inappropriate or even suspicious. As a result, she became more flexible in allowing family members to remain during the interviews when the participant agreed, recognizing their role as cultural and emotional mediators. This adaptation helped to build trust and deepen the quality of the data collected, while also underscoring the need for culturally responsive research practices in PC and EOL contexts.
Conducting Interviews and Feeling Bound (or Supported) by Ethical Guidelines
In the third theme that arose, NNH conveyed that she felt confident and capable of conducting interviews with Arab healthcare professionals, as she was able to identify with them and find commonality. On the other hand, interviewing Arab EOL patients was – and continues to be – a difficult and emotional experience for her. As she wrote in her report, “Just writing about this has my heart racing and I feel a strong sense of discomfort in my chest.”
Since the study centers on palliative care, NNH understood (or decided?) that her research population must include terminally-ill patients. Yet on the other hand, she felt bad about this: I felt selfish. I felt like I was exploiting people at the end of their lives. They should only have to deal with things that are right for them in these moments. Here I am, stealing an hour away from them, [at a time] when every minute matters, just for my own benefit and for academic purposes. I felt like I was a zero [a nothing, worthless].
In addition to these subjective feelings, NNH experienced difficulties in achieving ethics approval from each participating hospital. One prerequisite was that a member of staff from the hospital (i.e., NNH’s contact person or a principal investigator from the hospital) would attend a meeting held by the IRB, to defend the research plan and answer questions. One concern, for example, was how would the hospital ensure the patient’s adequately informed consent, especially when, under specific cultural norms, family members are greatly involved in the patient’s medical treatment and decision-making. In some hospitals, no members of staff agreed to participate in such a meeting, thereby hindering NNH’s receipt of the ethics approval. These hesitations stemmed from deep cultural concerns, as previously noted, including the widespread avoidance of direct conversations about terminal illness and death topics that may be seen as disrespectful, emotionally harmful, or in violation of accepted family norms, particularly by undermining the family’s involvement in decision-making. In such a cultural context, conducting a personal interview with a patient without the presence or knowledge of family members may be perceived as a disruption to the family cultural fabric. This raised concerns among hospital staff regarding the researcher’s ability to obtain truly informed consent from patients without violating the deeply held cultural codes of Arab society. These dilemmas intensified the researcher’s inner tension between her commitment to promoting equitable access to PC and her fear that the research itself might harm patients or be perceived as intrusive and exploitative during such a vulnerable stage of life.
Yet her devotion and motivation to conduct this important research, combined with her belief in its anticipated significance and value – especially for the Israeli-Arab society – helped her (try) to overcome these negative emotions; (perhaps only) upon receiving the first ethics approval from a hospital was she truly able to believe that her research is indeed ethical. Interestingly, here too, she was only able to truly believe that her research is not harmful to her society upon receipt of external approval reflecting the protection of research participants (in this case, from the IRB), yet not based on her own personal conviction.
There were additional challenges after receiving ethics approval and prior to conducting any interviews. At one of the hospitals, Faatima, the PI and head nurse at that hospital, a female Arab-Christian individual, continuously ignored NNH’s communications. From time to time, when she did respond, her answer was that no current patients in the hospital met the inclusion criteria; she even prevented NNH from meeting with the heads of the various departments, in NNH’s attempts to advance participant recruitment. In one phone call, Faatima explicitly conveyed her thoughts on the research: Listen, I’ve given lots of thought to your research. Even though the study has been approved, and even though I helped you with this, the research is unethical. You’re harming patients. You’re going against their cultural values… You’ve no idea what goes on inside the hospital. As someone who’s in direct contact with the patients, I’m telling you that your research is unacceptable and I’m going to write a letter to the committee to stop your study. I’m not going to be a part of this research.
NNH was deeply offended by these allegations, which undermined her confidence in both herself and the study. She viewed herself as someone who would never want to hurt anyone, particularly members of her own society. NNH felt motivated by a genuine desire to do good, but her frustration grew at the perception that Faatima’s stance blocked progress and stood in the way of pushing beyond previously untouched boundaries to ensure that patients receive the care they deserve. Moreover, NNH’s personal experience of regret and guilt over her father not receiving palliative care intensified these feelings. These conflicting emotions overwhelmed her, leading to uncertainty about whether to continue the research.
From Faatima’s perspective, NNH’s interviews may have been interpreted not as acts of care or inquiry, but as an intrusion into private, emotionally sacred space crossing unwritten cultural boundaries and potentially burdening patients who are already in a vulnerable state. This cultural clash between Western research ethics that value transparency and autonomy, and Arab norms that emphasize emotional shielding and family mediation may have led Faatima to see the study as fundamentally inappropriate, even harmful.
Following these tensions, after discussing this issue with DS, and following a conversation between DS and Faatima, we decided to re-examine the meaningful interactions that had occurred during previous interviewees. The aim was to emphasize and appreciate the benefits of NNH’s research for the Israeli-Arab Society by expanding and substantiating the discourse on palliative care within the Arab society and promoting its access and availability, while highlighting her desire to not harm any of the participants during her research.
An additional challenge that NNH faced, this time in relation to the interviews themselves, was whether to interview family members rather than the EOL patients themselves. This issue arose after encountering a number of difficult situations, for example where the patient was in very bad physical condition or wanted his loved ones to join the interview, or a family member had insisted on being present throughout the interview (as described above). Not only did NNH’s inclination to regard these requests positively stem from her interest in learning what these patients had shared with their loved ones, but also since the family in Arab Society is very involved in its members’ lives, especially EOL patients.
Yet based on his vast research experience and fearing that only involving family members in some anecdotal situations and not in others, would create methodological problems, possibly even jeopardizing the trustworthiness of the research, DS strongly advised her against this, encouraging her to maintain her original research plan, where the research population is solely comprised of EOL patients. Another concern that DS had was that there would likely be gaps between the patients’ actual desires and knowledge regarding palliative care and the family members’ recognition of this and their willingness to share this during the interview – especially due to the sensitive topic. Moreover, DS reminded NNH that the IRB of one participating hospital even specifically stipulated that “If the patient cannot or does not want to be interviewed, the researcher must not interview a family member instead of the patient.” Although these considerations were methodologically valid and based on scientific reasoning, they were not adequately culturally responsive. This created a significant challenge for NNH.
Supervisor-Student Relationship
NNH and DS frequently met to discuss the research and its progress. In most instances where NNH shared her deliberations, experiences, and challenges, they were both on the same page. Yet three specific cases presented significant differences between them – in attitudes, values, and knowledge. These included: (1) NNH’s desire to interview the patients’ family members, as discussed above; (2) the head nurse’s claim that the research is unethical and could harm patients; and (3) the possible emotional and physical risks to NNH that were associated with the research plan.
Upon further reflection on NNH’s engagement with the participants and their family members, DS began to rethink his insistence and preference for conducting one-on-one interviews with the patient (not including hospitals where the ethics approval explicitly does not allow this). Through the shared analysis of NNH’s report, DS was able to further and more elaborately understand her considerations, expectations, and experiences, including the power-relations between the individual and the family in Arab Society. These will now be addressed and taken into account in relation to the remaining interviews in NNH’s research project. Yet importantly, the exchanges and discourse between NNH and DS have provided more thorough grounds and validation for conducting this specific research – which holds the potential to promote more informed decision-making at EOL within the Arab Society, while improving the quality of life of EOL individuals. As NNH wrote in relation to her encounter with the head nurse, Faatima: With all the emotional turmoil, I’ve tried to gather myself and share this with my supervisor. The truth is that at the beginning of the conversation, I didn't feel like he understood my difficulties in continuing this research. I felt that he was only motivated by his interest in advancing the research. On the other hand, maybe this wasn’t the reason. The reason could be the cultural gap between us. What I experience as a value that contradicts my religious and cultural beliefs is something that is acceptable to him. Our attitudes towards death are so different. Our conversations weren’t easy. But I gradually felt him starting to look at it from a different angle. He managed to open my eyes as well. He emphasized my experiences where patients had thanked me for the interview, saying that I had helped them. At that point, I realized that I have to create change and that’s worth fighting for, to protect the dignity of dying patients and to provide quality care at EOL.
Following these conversations, and especially after writing this article, the emotional toll that this research has taken on NNH will receive much greater attention as the study progresses. As a team, we also realized that emphasizing NNH’s emotional and physical safety must be a top priority, as such risks and even possible violence towards NNH were not known to DS beforehand. Thanks to the shared reflective work of NNH and DS, it became increasingly clear that DS must employ a more in-depth approach to protecting NNH’s safety (in case of feeling physically threatened) and overall well-being throughout the research process.
Discussion
Intracultural and Intercultural Conflicts
This study sought to enhance a shared understanding and contextualization of challenges, experiences, and emotions that emerged as NNH, a novice researcher, embarked on her qualitative research journey to explore palliative care in the Israeli-Arab society. Adding to the difficulties that turned out to occur when conducting such sensitive research was the fact that the Ph.D. student is a female Muslim Israeli-Arab, while her supervisor is a male Jewish professor. Following the critical advocacy research design and using situational analysis methods, the study presented in this article analyzed a reflective report, which was created by the researchers and that detailed and addressed such challenges, experiences, and emotions.
Reflective analysis and ongoing discussions between the supervisor and Ph.D. student revealed that the initial research design employed a mono-cultural, standardized approach. This methodology presupposes that researcher activities and participant interactions can be managed through positionality and reflective engagement. Such an approach assumes that merely recognizing and articulating the researcher’s viewpoints and ideological stance constitutes adequate preparation for ethically rigorous qualitative research. Yet when reflecting on the issues presented in this article, we revealed that such strategies are often insufficient – especially when addressing challenges that are associated with sensitive research topics such as EOL, and even more so when involving dominant cultural issues and predispositions. For example, NNH’s interactions with the participants and their family members, or with the collaborating medical staff, call into question how cultural decision-making and considerations at EOL can be operationalized through research at end-of-life. As a minoritized researcher, NNH was able, in some cases, to form trusting relationships with the participants, while exploring meaningful insights pertaining to her sensitive research topic. Yet, at other times, she struggled to balance between her more traditional views, that had been shaped by her cultural norms and Muslim upbringing, and those that had more recently emerged and were possibly still developing – as she became a more western researcher, pursuing a Ph.D. under the supervision of a Jewish supervisor.
According to the concept of hermeneutical injustice (Fricker, 2007), people are “blind” to their own experiences and interpretations if these do not correspond with general concepts or theories. Indeed, this article demonstrates that some of NNH’s challenges – especially those that relate to her experiences and beliefs as a Muslim-Arab researcher – were not (fully) evident to NNH or to her supervisor. This could stem from the formal requirements that are associated with Ph.D. programs, where researchers are “expected” to be desensitized to particular, powerful, and well-established constructs of organizational and academic oppression (Pasque & Carducci, 2015). NNH struggled with her internal conflict: On the one hand, she was highly motivated to pursue a research study that she believes will be both important and beneficial (especially for her own society); yet on the other hand, she faced great suspicion and even objection to her study, by participants, family members, and position holders within the research setting – stemming mainly from their cultural outlooks and interpretations. Managing these struggles with an ad-hoc approach, NNH transitioned between one extreme position to another, trying to find and re-tell her own place and identity – to herself, to her participants, and to her community at large.
Higher Education Responsibilities Toward Students from Different Cultures
In line with the CRR, this article also reflects on the roles and responsibilities of higher education institutions in general, and of academic supervisors and mentors in particular – with an emphasis on being responsive to students from different cultures (Wisker & Claesson, 2013). This is especially important when conducting context-specific research that may not be in line with the (dominant) manner in which sensitive topics, such as EOL and palliative care, are addressed in western societies. The findings of this study also provide concrete meaning and context to what Carolin Kreber (Kreber, 2023) refers to as the pedagogy of authentic care in the context of postgraduate research. Such pedagogy calls for the development of specific supervision philosophies and skills that will enable students to find possibilities for reflecting their own identities, through the emancipation of and critical engagement with tradition especially as they are under various pressures and uncertainties (Ringo, 2025; Rogers, 2025). This pedagogy is highly significant, as this study also demonstrates how certain issues are ignored, possibly even silenced, by academic institutions – such as ensuring the researcher’s physical safety and emotional well-being (Dickson-Swift et al., 2006; Howard & Hammond, 2019)), or critically examining whether research that is couched as “culturally sensitive” may actually harm the participants or could be perceived as unethical, despite ethics approval.
In recent years, efforts have been made in higher education in Israel to promote Jewish-Arab co-existence (Masry-Herzallah & Amzalag, 2021); indeed, an increase in the number of Arab students can be seen attending higher education programs in Israel (Central Bureau of Statistics, 2022). Yet this study shows how the dominant culture of Jewish and Hebrew academia in Israel (Abu Ras & Maayan, 2014; Mizel, 2021) has undesirably contributed to distancing such issues from the forefront of research. As reflected in the data of this study, this dominant culture might have been understood by NNH as challenging or contradicting her existing norms and expectations.
Research Ethics and the Role of Research Ethics Committees
The data highlight the unique role of research ethics – particularly rules and practices relating to informed consent – and their meaning in relation to the actual practice of research, especially regarding culturally-sensitive qualitative studies. The shared reflective work of NNH and DS regarding these issues – in writing and during discussions – demonstrate how such guidelines actually perpetuate academic imperialism; in other words, they enhance the west’s impact and control of what is considered to be valid and credible knowledge (Alatas, 2008). As seen in the current paper, the political role of the (western homogenic) ethics imperialism is threefold, as it preserves: (1) the enforcing of (or dependency on) hegemonic notions regarding the freedom to choose whether or not to participate in a given study (2) the separation between the self (i.e., the individual); and its surrounding, in this context, the family; and (3) the primacy of quality of life over sanctity of life in and outside this world.
It is obvious from this study that IRBs and research ethics committees do not act in a way that acknowledge the plurality of understandings and meanings regarding the participant’s consent to take part in a research study (Kwame & Petrucka, 2024). Additionally, it seems that IRBs are not aimed at or have any resources to discuss or address ethical issues that emerge during the study itself, after the ethics approval has been granted and following the researchers’ complex interactions with the participants (Sperling, 2022). NNH’s experiences with Faatima (the head nurse), for example, convey the need for ethics committees and IRBs to create a culturally-responsive ethics review process – one that enables further discussions and engagement with the researchers after the approval has been granted and the research has begun – especially when applying the qualitative research methodology involving continuous and, at times also challenging interactions with participants throughout the research phases (Lahman, 2022).
Unique Cultural Challenges of Qualitative Research on End-of-Life
Moreover, NNH’s difficult interactions with some participants and their families highlight the complexity that is entailed in researching a charged topic such as palliative care, one that is culturally, ethically, religiously, and even politically loaded. The concept of epistemological violence refers to the interpretation of data in a manner that highlights the inferiority or problematization of the other (Teo, 2010). This notion may explicitly or implicitly regard reluctance to accessing palliative care, to discussing and accepting death and dying, and to referring patients to palliative care – as problematic and unethical. Yet paradoxically, and as shown in this article, such rules and practices actually oppress culturally-minoritized knowledge and beliefs regarding important life and death issues.
Our analysis highlighted the cultural-academic disagreement as to whether family members should also be interviewed in the research. To understand this finding, we apply a disability studies conception of autonomy that regards the relational constitution of the self as creating rather than curtailing the condition of possibility for autonomy (Braswell, 2011). We argue that Insisting on upholding western principles of research ethics by interviewing only “autonomous” and “capable” individuals (understood under a liberal concept of autonomy), while rejecting the possibility of interviewing a family member together with the participant, or even separatelycould be regarded as epistemicide. This latter concept refers to the purposeful act of devaluing, silencing, and even destroying culturally-minoritized knowledge and meaning (Patin et al., 2021). Doing so may also prevent the provision of space for collaborative learning and co-construction of knowledge (Rodriguez et al., 2011).
Most fundamentally, the data also significantly demonstrate that NNH questioned the legitimacy of her talking to members of the Israeli-Arab society on the topic of death and dying; in doing so, she felt that she was using up the little time that they had left for the benefit of her research, rather than allowing them to spend it with their loved ones. NNH herself is a member of the culturally-minoritized group that is the focus of her research; yet she was deemed untrustworthy by professionals who are members of her community; this made it impossible for NNH to recruit patients at that hospital or to continue with the interviews as planned. This situation also hindered her journey to achieving [western] knowledge and communicating it in a confident manner. This ambivalence cultivated the context within which NNH navigated: On the one hand, NNH felt like she was a “nothing” because she was bothering dying patients during their last precious moments, causing doubt and self-critical thoughts regarding her research design and feasibility. Yet, on the other hand, she felt lucky and blessed that she was able to have such open and meaningful conversations with some of these individuals during a vulnerable time; even feeling that she might benefit these participants by providing a meaningful way to spend timeand to have some control at a point when time was in short supply. Feeling this way encouraged her to proceed with her research, believing in its merit.
Conclusion
The insights presented in this article offer a rich, culturally-responsive, and critical examination of the methodological and ethical challenges that emerged during NNH’s research. They also advocate for change and further actions – within academia and broader social and political contexts. Yet for such change to take place, we must first recognize our interconnectedness and mutual dependence with other communities and systems outside our own. This is especially important in academic institutions where some students are members of minoritized communities – as in Jewish-Israeli academic institutions, where many Arabs also study, or in dominantly white academic institutions, where many non-white students also study. Such awareness is also important for academic mentors who are from different cultures than their students, as in the case of DS and NNH. However, even within the same culture or community, research difficulties may occur, especially in highly sensitive topics; such obstacles may lead to difficulties in interactions with interviewees and peers, and in the data collection, interpretation, and co-construction of meaning. To overcome such obstacles and generate change, the qualitative research design is a most suitable tool – as one of its key attributes is paying attention to the realities and effects of researcher biases (Ford et al., 2008).
Additionally, taking a richer cultural look at these challenges forces us to resist traditional western paradigms and epistemologies, while constantly reexamining and understanding our own identities and beliefs, within and outside our research activities. Doing so also challenges the notions of objectivity and neutrality in research, thereby making us genuinely and purposely engage with the other, with the aim of conducting relational discourse, learning, and knowing (Berryman et al., 2013). The shift towards actively engaging in transformative and critical thinking, to pave the way for future and unfamiliar worlds, symbolizes what Paulo Freire and bell hooks coined as the pedagogy of hope (P. J. Lopez, 2023). We should take this pedagogy seriously.
Finally, the challenges discussed in this study, and our understanding of them in light of the CRR, highlight the need for receiving input from relevant communities, as a means for informing about the implementation and cultural-specific research outcomes (Jordan & Hall, 2023; Pasque & Carducci, 2015); for ensuring that local knowledge is reflected in the gathered data; and for including such input and knowledge in the research plan and report. A promising approach to CRR includes community-based participatory research, a defined collaborative approach emphasizing participation of culturally minoritized communities in the research process from design to implementation and even dissemination, to address systemic barriersand align research methodologies with the lived experiences, priorities and agencies of such communities (Salami et al., 2025; Wallerstein & Duran, 2010). The practice of member checking (Birt et al., 2016; Lincoln & Guba, 1986), which tends to be understood in a limited manner, based mainly on its contribution to maintaining validity and trustworthiness in qualitative research (Candela, 2019; Goldblatt et al., 2011; Hallett, 2013) should be expanded to achieve the goals that underpin CRR. While paying careful attention to avoid undesirable harm or offence of participants who are members of culturally minoritized communities, qualitative researchers should actively involve these participants in the interpretation and meaning-creation of findings, thereby being more sensitive and attentive to the participants’ unique voices and realities).
This manuscript advocates for the continued use and development of the CRR framework and its approach to better understand, contextualize, and address methodological and ethical challenges that arise when conducting sensitive research with members of culturally minoritized communities. We believe that adopting this framework will enhance the cultural sensitivity of future research while supporting novice researchers from these communities in amplifying their voices, recognizing their valuable contributions to academia, and, most importantly, advancing the interests of their own communities.
Footnotes
Ethical Considerations
The general research underlying this study was approved by the Research Ethics Committee of the Faculty of Social Welfare and Health Sciences at the University of Haifa #254/22 (dated 17 July 2022) and the IRBs of the following hospitals: Carmel Medical Center # CMC-0160-22 (dated 21 August 2023); Galilee Medical Center # NHR-0152-22 (dated 15 October 2023); Hillel Yaffe Medical Center # 0119-22-HYMC (dated 3 September, 2023); Nazareth Hospital EMMS # 55-22-EMMS (dated 1 February, 2023); Soroka Medical Center # SOR-0103-23 (dated 28 February, 2023); Hadassah University Medical Center # HMO-0105-23 (dated 19 June 2024).
Consent to Participate
We confirm that all research participants gave informed consent prior to enrollment in the study. Informed consent for publication was provided by the participant.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Israel National Institute for Health Policy Research [grant number 2021/285].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.