
Abstract
The COVID-19 pandemic sparked what may be the largest number of oral history projects addressing a single public health issue. These collections range from brief informal efforts like those created in classrooms across the country to rigorous and formal projects led by institutions and those with expertise in oral history and archiving. The contribution of this article to existing methodological knowledge is that it brings an underutilized form of qualitative data—namely, COVID-19 oral history archives—into view for public health researchers and practitioners, and provides actionable guidance on using these data to address public health challenges. First, we orient readers to the range of existing COVID-19 archives, the questions they speak to and materials they include, and their current levels of accessibility. Second, we describe three ways that these archives might be used by the public health field to improve trustworthiness, preparedness, and health equity. These paths include: (1) Research: Using archives as a source of in-depth qualitative data on COVID-19 lived experiences to build contextualized understandings and refine ongoing emergency response and preparedness, (2) Teaching: Listening to archives as an opportunity for public health students to center the margins and strengthen emotional intelligence and empathy, and (3) Public Engagement: Creatively activating archives to deepen understanding of different truths and the different mindsets that shape our ability to achieve health equity. We anchor these paths with descriptions of how each might unfold based on existing work and/or models. Through these paths, we argue that oral history archives are a powerful resource for equitably and creatively addressing public health challenges.
Introduction
This paper is an invitation to make use of a form of qualitative data that we do not typically think about as a resource for public health: oral history. It is an invitation to consider what we can learn from creating spaces for people to tell stories about themselves, their experiences and their communities—in this case, about the COVID-19 pandemic—and then making these stories accessible for others to read, listen to, or watch. Finally, it is an invitation to stretch our view of what is useful in public health and what new ways of learning and practice might lay a more generative, connected, and equitable foundation for encountering and addressing public health challenges. In this paper, our aim is thus twofold: (1) to describe the diversity of COVID-19 oral history archives, and (2) to explore and develop three pathways by which oral history archives can be used by public health practitioners, educators and related professionals to work toward improved trust in public health, more equitable public health emergency response and preparedness systems, and ultimately equity in health outcomes across societal groups.
Imagine stepping into a cool room that appears at first to consist of only white walls. As artist and oral historian Nyssa Chow writes about her project Trace: A Memorial, “What you first encounter is absence […] a seemingly empty room.” As you move through the room, “the voices find you […] memories in media res, unbidden, unpredictable, like grief itself” (Chow, nd). If you pause, you realize that only you can hear a voice in that particular place, and that it is a portion of an oral history interview conducted with an essential worker in the early months of the pandemic. The audio evokes the worker’s feelings of being “invisible, expendable, abandoned,” the voice is full of “nuance, situated knowledge, and context” (Chow, nd). As you continue to move, other voices find you, allowing repeatedly “a solitary experience of listening in a crowded room” (Chow, nd). Five years after the beginning of the COVID-19 pandemic, how does this experience support our ability to access emotionally what was urgent earlier? How does it expand our understanding of what people experienced? How does it connect us to each other? How does it help us mark the distance between where we were and where we are now? Were you a public health practitioner, how might it shape the public health work you do?
Trace is just one project that has been nurtured and germinated in the soil of a COVID-19 oral history archive, and our goal in this paper is to broaden who might use these archives to sow other seeds. We are motivated by how much fertile ground exists. During the COVID-19 period, we witnessed a flourishing of oral histories collected to document people’s experiences of the pandemic, as well as the responses to racism and movements for racial justice that spiked concurrently. Oral histories were already being recorded by a team at Columbia University as early as March, 2020. By September, 2020 the Oral History Review, the journal of record for oral history in the United States, had published a special section on doing oral history during the pandemic (Caruso et al., 2020). Public historians launched rapid response collecting initiatives at local and international scales (Baik et al., 2022; Kelly, 2020). There was a palpable sense of living through a period that would be looked back on historically. At the same time, the demands of social distancing led us to be isolated from our larger social worlds, and technologies that became ubiquitous in many lives (e.g., Zoom) facilitated ease of engagement and recording. Collections arose to document the experiences of people with different backgrounds, in different places, with different professions, including people involved in the history-making decisions of this period.
Oral history is practiced across a wide range of contexts, from historians creating and analyzing primary source documents in the archive to sociologists using archives as datasets to media makers using stories in films and other artworks. Oral history has grown out of practices of storytelling and orality that are part of all communities. In particular, indigenous and enslaved communities have nurtured and used oral history practices, as “a testament to human survival, our aspirations for the future and the struggle to retain one’s dignity in an uncertain world” (Ortiz, 2021). According to indigenous historian Nēpia Mahuika, oral history remains “a crucial part of how we identify and make sense of our place in the world and the world’s place in our community” (Mahuika, 2019). Indigenous scholars note that these oral traditions are both related to and distinct from “popular academic conceptions” of oral history (Mahuika, 2019), which produce archives of the kind we discuss in this article. These archived forms of oral history are where we place emphasis in this article because of their availability and potential for use in public health, though we acknowledge that projects involving storytelling that are not archived for public use can also be critical sources of knowledge toward public health goals (Kahn et al., 2023).
The forms of oral history discussed in this article are typically intersubjective and grounded in shared authority, meaning that an oral history is co-created by the teller and the listener and shaped by both people’s subjectivities (Frisch, 1990; Portelli, 2018). Oral histories tend to be open-ended and wide-ranging, seeking to understand a specific experience within the setting of a person’s whole life and broad social and historical context. Oral histories focus not only on what happened, but also on what it means. Narrators are specifically invited to make sense of, share, and theorize about their experiences, alongside researchers. The presence of memory, analysis, and subjectivity in an oral history is not a distraction but a core part of what makes oral history valuable. Unlike other forms of qualitative research, oral histories are typically (but not always) produced with the aim of sharing the full interviews publicly and preserving them for future use, creating rich public archives (OHA Principles and Best Practices, 2018; Yow, 2015). Additionally, oral history is a qualitative research method that is often explicitly anchored in practices of social and restorative justice, with those goals at its heart (Janesick, 2015; Kerr, 2016; Mayotte & Kiefer, 2018; National Centre for Truth and Reconciliation, 2020; Voices Remembering Slavery, nd). Writing in the American Journal of Public Health, editor Lisa Bowleg described the importance of the critical use of the social sciences to public health and recommended utilizing diverse and underrepresented methodologies and methods. Bowleg also called for placing greater attention on strengths and assets, rather than solely focusing on problems and risks (Bowleg, 2019). As we will demonstrate in this article, oral history as a method has the potential to address both these calls.
Oral history is a process that creates a product (Lee & Springer, 2020). Much has been written about the process, challenges, and importance of undertaking oral history during the COVID-19 pandemic (for examples, see Caruso et al., 2020). In this paper, we focus instead on the products of these oral history efforts, these records of human experiences during this time, and how we might put them to use. We argue that these stories are a powerful resource for public health. At present, public health tends to value biomedical frameworks and large quantitative datasets above complex and richly told stories (e.g., a 2022 analysis of methods used in the 100 most recent papers in top public health journals showed that only four articles used primarily qualitative methods (Stickley et al., 2022)). Moreover, today’s health inequities are partly due to historical oppressive practices in public health that prioritized physician expertise over that of advocates and affected communities, and disease control over building sustainable care systems, and that failed to address racism and colonization as animating forces (National Association of County and City Health Officials, 2024). These problems persist in many domains of public health. However, the stories that emerge through oral history can “help us build a bridge between the sociological and abstract dimensions and the individually lived, personal dimensions” of oppressive systems at the root of so many public health problems (Bell et al., 2008, p. 9). Therefore, stories can help public health practitioners and researchers see the work of these systems and our humanity more clearly.
Such changes are essential as public health in the United States faces many specific challenges. Trust in the public health field and its institutions has emerged as a major concern from this period (Best et al., 2021), with misinformation circulating widely and rapidly (Murthy, 2021), and partisan differences in trust widening during the 2024 U.S. presidential campaigns (Kearney et al., 2025). The ongoing and immense population health inequities in the United States pose a related challenge. Research indicating that American Indian/Alaska Native and Hispanic populations saw the greatest disparities in observed versus expected COVID-19 mortality demonstrates the need to improve the reach and effectiveness of public health infrastructure and practice (Faust et al., 2024). For example, as Black and Latino parents described their decision-making around vaccinating their children for COVID-19 in early 2022, both historic knowledge of abusive actions on the part of the U.S. public health and medical systems and present day experiences of structural racism were prominent (Whang et al., 2023). In this context, conversations with trusted messengers, like teachers and doctors who listened patiently and validated feelings of hesitation, were described as more impactful than incentives and other messaging that ignored their concerns.
As we argue in this article, valuing these stories, perspectives and memories and centering their truths is critical for rebuilding trust in public health in a segregated and polarized society. Oral history offers an opportunity to understand through contextualized stories how trust is built and broken; how information about public health challenges is gathered and circulates; and how marginalized communities sustain themselves in the face of these challenges. Through exposure to and careful analysis of these stories, public health researchers, practitioners, and others can develop what Engebretsen and Baker (2023) call “narrative preparedness”: an ability to understand and empathize with other peoples’ stories and the values they encode, to assess these stories based on the universe in which these people live and operate and to acknowledge the narrative fidelity of their stories – even when these are in conflict with the rationality of science (p. 7).
Though the number of collections documenting COVID-19 is unprecedented, oral history projects that document public health issues are not uncommon. As examples, books drawing on oral histories of HIV/AIDS from frontline workers to activists have helped people connect with and learn from this epidemic (Bayer & Oppenheimer, 2002; Cvetkovich, 2003; Oppenheimer & Bayer, 2007), while collections focused on the reproductive rights efforts of the past (Smith College, 1971) and reproductive health actions in the present (Duke University, 2024) are documenting these public health social movements over time. A 2018 review article on the uses of oral history in public health found that projects most commonly explored health risks and experiences, including living with illness, and less commonly documented aspects of infectious disease outbreaks or used oral history as a kind of intervention (Tsui & Starecheski, 2018). In the paragraphs that follow, we make a case for expanding and deepening the use of oral history archives in public health, taking the flourishing of COVID-19-era archives as our motivation and case. We first introduce readers to the kinds of data and archives that were produced to document the COVID-19 pandemic. We then present three paths for using COVID-19 archives to invigorate public health research and practice in response to this historic public health challenge.
A Typology of COVID-19 Archives
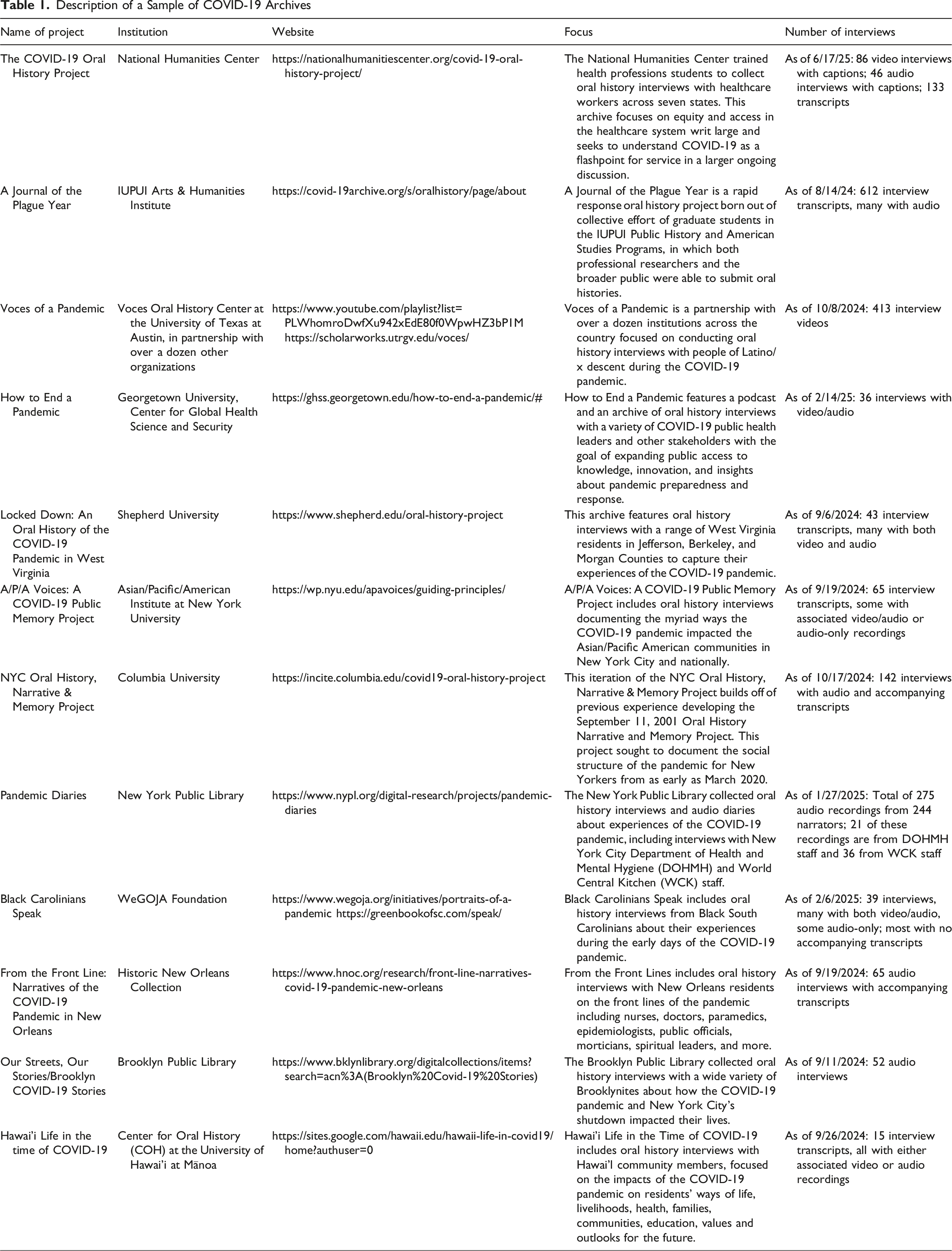
Description of a Sample of COVID-19 Archives
Geographically Focused Projects
Often efforts to collect oral histories have been focused geographically, in part because a particular institution or researcher with an interest in that locality might lead the effort, and/or because of the way that COVID-19 affected geographic areas differently at different times. The NYC Covid-19 Oral History, Narrative & Memory Project was created by sociologists and oral historians at Columbia University. The team from Columbia had led a similar rapid response collecting effort around September 11th and its aftermath, and the city’s status as an early epicenter of the pandemic was one motivation for creating this geographically-focused project. As an alternative example, Locked Down: An Oral History of the COVID-19 Pandemic in West Virginia was organized by historians at Shepherd University, and sought to document experiences of the pandemic in the last U.S. state to record its first COVID-19 case.
Population-Focused Projects
Other projects have focused on particular populations because of the unique role they played in managing the pandemic and/or because of the pandemic’s specific reverberations for them. How to End a Pandemic collects interviews with leaders who are “key actors in past, present, and future epidemics from a wide range of political, business, industry, and public health backgrounds,” while a collection within the forthcoming New York Public Library Pandemic Diaries project focuses on the experiences of employees of the NYC Department of Health & Mental Hygiene (DOHMH). Voces of a Pandemic is “dedicated to recording, preserving and disseminating the unique perspectives of Latinos/as” during the pandemic, in recognition of how heavily impacted they were. A/P/A Voices: A COVID-19 Public Memory Project takes as its motivation both the disproportionate impact of COVID-19 on Pacific Islanders and some immigrant Asian populations and the experience of anti-Asian violence and xenophobia during the pandemic.
Timing of Projects
Several projects collected oral histories only in the earliest and most disruptive phases of the pandemic (e.g., Black Carolinians Speak, 2020-2021), while others have collected for longer periods of time. The NYC Oral History, Narrative & Memory Project collected interviews longitudinally with the same narrators from 2020 to 2022. A number of projects collected interviews into 2023 (e.g., A Journal of the Plague Year, Voces of a Pandemic). In early 2024, the Library of Congress launched a new effort to collect Americans’ COVID-19 stories (Library of Congress, 2024).
Centrally Led versus Decentralized Archives
Another important distinction in types of archives relates to whether the materials in an archive were centrally planned and collected, for instance by a single interviewer or a team of interviewers (as was the case with the majority of archives in Table 1), or whether the approach was more decentralized. In more decentralized projects, a team might create the archival infrastructure and then launch an open call for public submissions. For example, A Journal of the Plague Year, The New York Public Library’s Pandemic Diaries project, and Hawai’i Life in the time of COVID-19 both mixed centralized and decentralized collecting. In these projects, some narrators were interviewed by trained interviewers, while other “crowdsourced” oral histories (or audio diaries) were submitted directly by narrators.
Institution-Held versus Community-Based Archives
A final important distinction among oral history archives is that some are held by institutions or partnerships that have long histories of hosting archives and the infrastructure to do so, like libraries, while others are being managed by less formal groups and/or community-based organizations and their partners. These variations in infrastructure and archiving expertise can translate into differences in accessibility and searchability of archives, as well as perhaps the ability to sustain accessibility over time. While creating Table 1, we found that it was easy to gather descriptive information and access oral histories for some archives, while for others, finding information required substantial outreach. Preparing archives for public access is a major undertaking, and thus a number of archives–even those held by well-funded institutions–were still in preparation at the time of writing and thus not yet accessible (though slated to become so). Notably, some archives of great potential importance for public health, like Black Carolinians Speak, were only minimally accessible. This could be for a variety of reasons, whether unintentional (e.g., due to funding constraints) or intentional, due to the wishes of the communities or individual participants involved (who might prefer for those materials to serve internal needs and goals first or only (Kahn et al., 2023)).
Using Oral Histories to Shape Public Health Learning and Practice
Bringing to mind all of the interview hours, connections, stories, and experiences involved in just the interviews represented in Table 1 motivates us to think carefully and creatively about how COVID-19 archives might be used by the field of public health. Below we detail three paths—research, teaching, and public engagement—through which archives can serve as a resource for addressing public health challenges equitably and creatively. We briefly summarize these paths, their possible outcomes, and their intended impact in Figure 1, and identify the core practices involved in working with oral history materials that undergird all three paths. Paths Between the Use of COVID-19 Oral History Archives and Solutions to Public Health Challenges
Research: Using Archives as a Source of In-Depth Qualitative Data on COVID-19 Lived Experiences to Build Contextualized Understandings and Refine Ongoing Emergency Response and Preparedness
Contextualized Understandings
Epidemiology has been described as the “cornerstone” of public health, using quantitative research to identify “the distribution of diseases, factors underlying their source and cause, and methods for their control” (“Epidemiology Is a Science of High Importance,” 2018). The tools of epidemiology are thus invaluable in public health practice, allowing us to track disease, risk, and make comparisons to shape prevention and response. In their efficiency, parsimony, and quest for generalizability, however, these approaches must reduce complexity and context to measurable, known variables. Because large sample sizes help to ensure validity, epidemiology often prioritizes collecting the data that is most feasible to collect from the people who are best able to provide it. More open-ended, person- and community-centered understandings of public health issues are thus an important complement to epidemiologic understandings. These qualitative understandings can be labor-intensive to collect and distill, requiring skill and trust to gather data. Oral history archives are thus valuable not only for their depth and breadth, but also because they have already been collected. Contextualized understandings of the experiences and truths of marginalized groups (e.g., people who experience racism, sexism, ableism, and other forms of oppression, people who are structurally and economically marginalized, are socially isolated, face language barriers, have poor access to health care and education) can be especially challenging to access, yet it is these understandings that are most essential to the core public health goal of health equity.
COVID-19 archives provide an in-depth view in real time, situated to some degree in the narrator’s personal background, location, and profession, of what it was to experience the COVID-19 pandemic. These interviews sometimes include broader reflections on the meaning of these experiences, as narrators understood them at the time of the interview. Narrators in many cases reflect on the complex social and economic issues that people faced during this period, how they came to learn what they knew and practiced related to COVID-19, the collective and personal strengths drawn upon, and for many, the family or community loss experienced. These interviews thus present an opportunity to deepen understanding of community-driven support systems and the structural and social drivers of health inequities.
Qualitative Research Questions to Which Archival Analyses Can Contribute

Analyzing Archival Data
Using archives for research purposes typically involves treating interviews as qualitative data and can employ a variety of approaches. For public health purposes, forms of thematic analysis may be the most appropriate and accessible for answering the research questions in Table 2 in ways that are intelligible to public health audiences (e.g., Braun & Clarke, 2022). Forms of narrative analysis may also be appropriate for exploring the questions focused on stories or individual trajectories over time (e.g., Josselson & Hammack, 2021). For example, longitudinal analyses of how public health leaders told the story of this period at different points may give us insight into how to more effectively narrate pandemics in the future. Additionally, using methods like Carol Gilligan’s Listening Guide may be especially fruitful in helping us to attune to the emotional registers and multiple voices that are woven through narratives (Gilligan & Eddy, 2021). Finally, using large language models and artificial intelligence are also now increasingly common when organizing and analyzing large qualitative datasets (Morgan, 2023), including oral histories (Pandza, 2023), and may be useful for organizing data and assessing its ability to address the questions we have posed in Table 2. 3
Teaching: Listening to Archives as an Opportunity for Public Health Students to Center the Margins and Build Empathy and Critical Thinking
Public health education is evolving in response to the experience of the COVID-19 pandemic era, and oral history can contribute usefully to this evolution. Such education takes place at both the undergraduate and graduate levels, and trains students to work in epidemiology and biostatistics, health policy, communication, health care management, community health, environmental health, among other domains. In recent years, the Association of Schools and Programs of Public Health has called for a reenvisioning of public health education by “promoting inclusive excellence through an anti-racism lens, embracing transformative pedagogical approaches, and nurturing robust community partnerships for the betterment of our global health landscape” (ASPPH, 2024). Listening skills and empathy are foundational to all three of these goals, and particularly to the connected, collaborative work that they require. Yet we have rarely taught these explicitly in public health education. Echoing these goals, Dr. Dave Chokshi, who directed the New York City health department during the COVID-19 pandemic argues for “building the future of public health around people,” and writes that this “must mean getting more proximate to the people whom we serve” (Chokshi, 2023).
Using oral history in public health education can support the development of these skills. Inviting students to work with oral history archives is a common approach in history courses, as a way to foster empathy, engage critical thinking skills, and compare sometimes competing narratives (McNicholl, 2018). COVID-19 archives could be used toward similar educational purposes. For public health students, we might imagine the creation of educational modules that integrate audio interviews and transcripts to create opportunities to listen deeply, to help students connect with experiences of the pandemic that were distinct from their own, to better understand this period, and to suggest public health practices that productively incorporate and respond to these experiences.
A National Endowment for the Humanities (NEH) lesson plan exploring the experiences of enslaved people before and after emancipation provides an excellent structure for considering how we might develop learning modules for public health students (National Endowment for the Humanities, nd). This lesson encourages instructors to select interviews that represent a range of narratives from Born in Slavery, an archive of 2,300 first-person accounts collected as part of the Federal Writers’ Project. To help instructors with this task, the NEH lesson plan highlights 10 sample stories. The first of four student activities is developing an understanding of the historical and administrative context for the interviews to help students understand what they are reading or listening to. Students answer questions like: What was the goal of the project? Who were the interviewers? 4 How were interviewees selected and approached? What do you already understand about the experiences at the heart of these interviews? The second activity involves offering students interviews to read and asking them to summarize certain aspects of these interviews. The third activity is sharing findings within the class so that everyone understands the full sample of interviews. The final activity is a full class discussion driven by the following questions: What different perspectives did narrators present? What details intrigued or surprised you? How have these stories changed your understanding of the topic/experience under study?
A version of this exercise for public health students specifically might extend this discussion into an assignment. This assignment could ask students to describe and critique how public health actions, policies, and systems affected those people whose stories were shared, and to suggest how new public health frameworks and actions might lead to different stories. We see such activities as integral to cultivating a socially conscious public health workforce attuned to both the systemic issues and the first-person stories that can help us address and humanize public health challenges.
Public Engagement: Creatively Activating Archives to Deepen Understanding of Different Truths and the Different Mindsets That Shape our Ability to Achieve Health Equity
This section speaks to ways that archives might be mobilized to invite members of the public to engage with oral history in ways that can deepen understanding of experiences that are different from our own and shift the mindsets underpinning how we, as members of the public, envision what an equitable emergency response and health system can be.
Engaging with Artists, Activists, and Mobilizers of Stories to Create Activations
Oral historians sometimes use the terms “activation” or “mobilization” (Menjívar, 2023) to highlight the ways that oral history materials and people can be brought together for meaningful interactions, sometimes “as a working tool for aiding community efforts for social justice” (OHA Social Justice Taskforce, 2022). The Trace project described at the beginning of this article is one example. Some common ways of activating oral histories are through the creation of listening events, exhibits featuring audio from oral histories, and web-based exhibits where audio clips are curated for public interaction. Other ways that oral histories have been activated include the development and performance of plays based on oral history interviews, as well as documentary films, graphic memoirs, and place-based audio projects using oral history materials. Creating these kinds of products, exhibits, and experiences requires specific skills to craft, curate, distill, and effectively mobilize oral history materials. As such, we might view oral history as equipping artists, activists, content makers, experience designers, and narrative strategists with material to advance and inform strategies in public health and for health equity. In partnering with public health to do this, these practitioners can expand the types of stories and experiences the public is aware of, provoke participants to draw connections between the materials and their own experiences or practices, support visioning and reimagination of systems, and raise questions for participants to grapple with and potentially act on.
Using Oral History’s “Ecosystem of Stories” toward Narrative Change
Oral histories can be important material for narrative strategists working to advance health equity. Narrative change has become an increasingly visible and resourced part of the public health toolkit in recent years. This work understands narratives, often referred to as mindsets, as “fundamental, assumed patterns of thinking that shape how we make sense of the world and act in it,” which are highly durable with deep historical roots (FrameWorks Institute, 2020). Engaging in narrative change is an intentional effort to shift the stories that guide our mindsets and actions (Robert Wood Johnson Foundation, 2024). This begins with recognizing and critiquing harmful narratives in our society (e.g., individualism, racism, zero sum game, and free self-regulating markets), which helps to make health-promoting systems change feel possible (e.g., changing economic systems, health care systems) (National Academies of Sciences, Engineering & Medicine, 2024; National Association of County and City Health Officials, 2024). As narrative change experts write, “Audiences will interpret the same facts differently, depending on the narrative that is most salient in their minds” (Jenkins, 2018). Oral histories can reveal the dominance and the influence of these harmful narratives in the experiences and perceptions of people and groups during a public health crisis. They can collectively counter harmful narratives about structurally marginalized communities (Hernandez et al., 2017). They can help inform the practices that strategists should use for narrative organizing and power building to shift mindsets toward our ability to create equitable communities and systems of care (Robert Wood Johnson Foundation, 2024).
Some narrative change convenings have emphasized the importance of expanding our understanding of a wide array of different stories and the different mindsets expressed in these stories, writing that “creating an ecosystem of stories, a depth of narrative immersion, is needed to truly change social norms and cultural practices” (Open Society Foundations, 2019). Types of stories that may be especially useful in shifting mindsets to support health equity include those about: intersectional harm and repair; power and contemporary collective action; health realities and harmful systems; reclamation of cultures; connections between land, place and health; and community health, autonomy, and agency (Robert Wood Johnson Foundation, 2024). As in the public health education example given above, oral history archives are well-positioned to supply stories to support this narrative immersion process. Below we provide one example of how COVID-19-related stories, in particular, are being used to try to change narratives with the goal of long-term policy and systems change.
Marked by Covid is a “justice and remembrance movement led by Covid grievers” (https://www.markedbycovid.com/). They organize vigils, meetings with elected officials, and other events toward the goal of acknowledging and remedying “the inept federal response” to the COVID-19 pandemic. The first pillar of their policy platform is “Recognition: Advance healing and restorative justice by ensuring remembrance, accountability for preventable harms, and an unvarnished national narrative” (Marked by Covid, 2022). This involves the creation of public memorials, as well as establishing oral history projects “to capture the lived experience of workers deemed essential, people bereaved by Covid-19, people living with Long Covid, and public health experts.” They thus seek to shift the narrative of COVID-19 as over and thus no longer requiring attention by using the memories and stories of people in these groups. One way they have done this is through the creation of a National Covid Memorial, which uses augmented reality technology to present images and remembrances of a large number of people who died as a result of the pandemic. These efforts anchor a detailed policy advocacy agenda, which centers the ongoing structural needs of those most affected by COVID-19. By engaging the public with these memories, the group aims to facilitate “restitution and accountability for the policy failures that led to profound racial and socioeconomic disparities in risks of infection, severe illness, and death” (Goggins, 2023).
Challenges and Limitations
We see oral history archives as offering new ways forward for addressing a range of public health challenges. These new ways forward include contextualized understandings of COVID-19 experiences to improve the effectiveness of emergency response, a more empathetic public health workforce, and a wider array of stories of the pandemic to shift mindsets in ways that promote health equity. Nevertheless, there are some hurdles to incorporating oral history archives more robustly into public health research and practice. First, these archives are powerful in part because of the emotions that they potentially engage and provoke. However, people may resist delving into these archives precisely because of these emotions and the range of traumas that might surface alongside them. (We are reminded of the opening line of a 2023 New York Times Magazine article reporting on stories from the NYC Covid-19 Oral History, Narrative & Memory Project, which read “Notice your resistance to reading the next several thousand words” (Mooallem & Gilbertson, 2023).) Second, archived oral histories preserve what narrators knew or had learned at a given point. They may therefore contain information that was incorrect at the time or that we know now to be incorrect. Thinking through how to assess and handle this when working with these materials for public health purposes is an important step. Third, while qualitative methods have gained recognition and use in some domains of public health (most recently in implementation science (Hagaman et al., 2021)), there are many in the field who still do not recognize the roles and contributions of qualitative research, and thus would not be able to appreciate the value of these archival resources. Fourth, some of the paths we describe would require collaboration with uncommon partners, for example, archivists, librarians, artists, community organizers, and media makers. This might challenge the imaginations and inertia of some in public health, while inspiring others. Fifth, there are important ethical considerations in using archived oral histories. For instance, it is critical for public health practitioners to learn about the goals and contexts of the initial gathering of the oral histories to be used, and to work with these materials in ways that are consistent with initial consent from narrators (and ongoing consent where possible) and that prioritize community health and well-being. Finally, while contemporary oral history often seeks to collect the stories of marginalized people specifically, there are still inequities in whose stories are collected, as well as inequities in the quality and accessibility of archives that we have noted. We are aware that invisibilization of marginalized groups can be magnified by secondary data use (Borderon et al., 2021), and suggest that public health practitioners and researchers emphasize the use of archives focused on these marginalized groups, while collaborating with oral historians and communities facing public health challenges to continue addressing gaps.
Conclusion
Our goal in this article has been to share a sense of the opportunities within oral history archives, alongside an understanding of the challenges of bringing new sources and forms of data more actively into public health. We believe that archives are unique and deep resources, which notably, given the immense effort required to collect high-quality qualitative data, have already been collected. To support the practice of public health going forward, we hope that qualitative researchers, educators, and narrative specialists, as well as emergency preparedness and response leaders and other leaders will collaborate to use archives for research, education, and narrative change, as described above. Engaging with oral historians and archivists to stay attuned to the nature and nuances of these archives would also benefit projects that follow the paths we describe. Moving forward, projects might involve exploring the role of oral history materials in shaping mindsets and health policy, exploring longitudinal uses of oral history archives for public health, and developing community-partnered, participatory public health research using oral history methods and archives. Once we are actively undertaking these collaborative activities, as future directions, it will be important to assess their utility to public health through thoughtful evaluations of both processes (e.g., extent to which empathy, deep listening, and other core practices are cultivated) and outcomes (e.g., increased trust in public health; development of more equitable emergency preparedness and response; achievement of equity in health measures), as outlined in Figure 1. With these efforts, we can make use of the fertile ground that oral history archives offer for seeding the ongoing recovery, repair, restorative and reparative efforts that are needed to encounter current and future public health challenges more equitably and creatively.
Supplemental Material
Supplemental Material - Using COVID-19 Oral History Archives to Support Equitable and Creative Solutions to Contemporary Public Health Challenges
Supplemental Material for Using COVID-19 Oral History Archives to Support Equitable and Creative Solutions to Contemporary Public Health Challenges by Emma K. Tsui, Steffie Kinglake, J. Robin Moon, Riki H. S. Eijima, Amy Starecheski in International Journal of Qualitative Methods.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants in the oral history projects discussed, as well as the individuals who have gathered, prepared, archived, and worked as stewards of these stories. All of you have been an inspiration in this process. We also thank the attendees at the Oral History Association’s 2024 annual meeting who shared input and ideas.
Informed Consent
The oral history projects discussed in this article often draw on the oral history field’s code of ethics, which includes informed consent. (In 2019, a revision to the Common Rule clarified the exclusion of oral history from the category of human subjects research that necessitates review by an IRB.)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was partially supported by the Cooperative Agreement Number NU50CD300866 funded by the Centers for Disease Control and Prevention (which supported Riki H.S. Eijima's collaboration). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention of the Department of Health and Human Services, nor the policy of the American Medical Association.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.