
Abstract
Loneliness epidemics affecting roughly 10% to 40% of adult populations do not have sufficient guidance for public health experts or governments to adequately address. To improve guidance, we developed an interdisciplinary approach to deepen explanation of underlying causes of loneliness using a critical realist lens. Using theory about social connection as a human basic need to frame our analysis, we first conducted thematic narrative inquiry to examine broader patterns in the social systems adults described during loneliness experiences. Secondary data came from online, open-ended survey responses by anonymous adults about their loneliness experiences, made publicly available by The Loneliness Project in 2018. We further developed our results through abductive reasoning to deepen explanation of underlying causes. Major Health Problems, Big Moves & Small Families, Stigma Mistreatment or Abuse, Caregiving Beyond My Capacity, and Fitting In, described five social systems of poor relationship quality that could compound across society and over time, resulting in exclusion from society. These systems could intersect, explaining differences in the severity of exclusion. Five main social systems were found to describe the process of marginalization from society. These results offer an alternative approach to clinical and therapeutic interventions for loneliness that have focused on individual changes of lonely adults to find inclusion in their communities. It may be possible to identify specific mechanisms for marginalization that could be changed to reduce severe and chronic loneliness for whole communities.
Keywords
Introduction
Prevalence of serious loneliness in adult populations varies based on age and country, with higher estimates found to range roughly between 10% up to 40% (Surkalim et al., 2022). Chronic or severe feelings of loneliness are predictive of worsening mental health, such as anxiety, depression, or suicidal ideation, and physical health like cardiovascular disease or all-cause mortality risk (U.S. Department of Health and Human Services, 2023). As a result, local and national governments have declared a loneliness epidemic, designating new agencies and/or policies to address it (Goldman et al., 2024). Guidance to effectively address loneliness is lacking, as therapeutic interventions are found to have significant improvements in reducing loneliness, but not enough to return to baseline levels (Hickin et al., 2021; Hoang et al., 2022). Loneliness also has a long list of risk factors outside the control of therapy, such as geographic and income barriers for connection, but there is no guidance on how to address them effectively (Barjaková et al., 2023; Goldman et al., 2024). An inability to identify and determine effective interventions at the scale of an epidemic may be due to confusion around what causes loneliness. In an interdisciplinary literature review, a causal mechanism for how the quality of social connection as a human basic need could directly impact human health was identified, with shared understanding across biology and social science disciplines (Bauer et al., 2025). Our study aimed to use this theory to better understand the social environments of lonely adults and improve explanation of underlying mechanisms for how these social environments increase loneliness.
The confusion surrounding loneliness stems from conflict in underlying assumptions. On the one hand, loneliness is thought to indicate that the human basic need for social connection is not being met in a way that is critical to human survival and health. Social connection can encompass any direct social interaction in human society and its impact on human wellbeing (Bauer et al., 2025). Loneliness is framed within it as a physiological signal similar to hunger, in which there may be neurological feedback systems that regulate social connection with others to fulfill neurological dependency on social interactions (Cacioppo & Patrick, 2008; Fulford & Holt, 2023). It may play a key role in human evolution that was critical to the survival of early ancestors (HHS, 2023).
On the other hand, loneliness is also thought to be a perception that one’s quality of relationships is different than desired, described by the Cognitive Discrepancy Model (Lim et al., 2020). Loneliness is not correlated with social isolation, which is the measure of one’s quantity of relationships (HHS, 2023). One can feel alone in loneliness, even when having a high number of relationships with others. It can be measured using a validated survey that asks about perceptions of relationships, such as feeling left out, isolated, or lacking companionship (Russell, 1996).
Loneliness researchers can overlook this theoretical tension to simultaneously treat severe forms of loneliness like a mental illness that indicates dysfunction as well as an unmet basic need. Deprivation of a physiological need like food and water can develop into disease (McEwen, 1998), but there is an important distinction between interventions that supply for basic needs within communities and clinical interventions to treat malnutrition or dehydration. Loneliness interventions can blur this distinction, commonly testing one-on-one therapeutic interventions or small group community interventions in order to improve personal relationships with oneself, family, friends, or community members (Eccles & Qualter, 2021; Paquet et al., 2023). With a focus on quality, they often have goals to increase meaningful relationships, such as relationships that are emotionally satisfying or in which individuals feel valued (O'Rourke et al., 2018). Some loneliness researchers are also proposing pharmaceutical interventions that ignore relationship quality, but hope to modify the impact of loneliness internally to disrupt what they consider to be destructive social behaviors (Cacioppo & Cacioppo, 2018; Jeste et al., 2020).
The challenge in loneliness research is understanding the paradigm shift in treating social connection as an equivalent human basic need to water, food, and shelter (HHS, 2023). There are biology implications when describing humans as a “social species” and “social connection” as a universal need that includes “quality” in relationships (Tomova et al., 2021). It pushes both biologists and social scientists into an uncomfortable space of integrating their work that has a history of ethical concerns (Schutt & Turner, 2019). The scale of integration would also be unprecedented, potentially simplifying all of human social life into an overarching category of quality that is critical to individual survival. Critical realism may help work through disciplinary and theoretical tensions that can improve understanding of loneliness and how to effectively address an epidemic.
Critical realism is a philosophy of science that is known to emerge in research during times of crises when prevailing wisdom fails to account for unintended or unforeseen consequences (Buch-Hansen & Nielsen, 2020). One of the goals of critical realism is to reflect on assumptions used in fields like public health, and examine how well these assumptions explain our reality (Bhaskar, 2016). It is suitable for loneliness research, because critical realism has been designed to examine open systems centered around human social life (Bhaskar, 2016). In qualitative research it can identify and deepen explanation of mechanisms that produce events, like a loneliness epidemic, even when mechanisms are not directly or empirically observed (Elder-Vass et al., 2023). Since critical realism rejects the dualities that can be found in other philosophies of science, such as the duality of an objective reality found in positivism and a socially constructed world of meaning found in social constructivism, its application is suggested to address problems that arise when switching between paradigms (Bhaskar, 2016; McEvoy & Richards, 2006).
An underlying causal mechanism for how the quality of social connection can directly impact human health has already been theorized through interdisciplinary models that integrate biology and social science knowledge (Bauer et al., 2025). However, uncertainty remains about how the mechanism works, and it fails to explain the quality issues in social connection experienced by lonely individuals. In a prior qualitative study, we adapted a critical realist approach to deepen explanation of relationship quality during lonely experiences (in review). In an online community of over 200 adults, we found a discrepancy between four poor qualities and one positive quality: grieving relational loss, rejection of who I truly am, present but emotionally absent, and excessive labor, in contrast with being cared for. However, this discrepancy only explained feeling lonely in direct social interactions. The study was unable to achieve a goal of critical realism to develop depth in explaining underlying mechanisms producing loneliness beyond its experience and direct social interactions. The results suggested we needed to use a different method that could examine the interplay of larger social processes occurring across society.
We conducted a qualitative research study that examines patterns in social systems resulting in feelings of loneliness, as observed by 219 adults in an anonymous online community. We used thematic narrative inquiry to analyze secondary data. Data were framed with theoretical models that describe a causal mechanism for how a whole social environment as a system can directly impact human health outcomes through loneliness. We used abductive reasoning to examine these results further and how they can deepen explanation of the theoretical causal mechanism. In this way, our final results can be interpreted through a critical realist lens. We aim to improve guidance for developing effective interventions at the scale of loneliness epidemics.
Materials and Methods
Methodology
We conducted a secondary qualitative analysis in two distinct steps. While each step is informed by a different philosophy of science that can compete with the other, our overarching approach is interdisciplinary to focus on common ground (Bergmann et al., 2012; Repko & Szostak, 2008). We chose this approach because the scale of integration that would be required between biology and social sciences to understand social connection as a human basic need under the same philosophy of science is beyond the scope of our research study. Instead, our study worked toward bridging this divide by developing an interdisciplinary approach. In an interdisciplinary literature review we examined a wide range of theories across biology and social science disciplines to identify shared understanding about a causal mechanism for how social connection as a human basic need could directly impact health outcomes, including through loneliness (Bauer et al., 2025). Both steps in our study are dependent upon this theory as common ground, but differ in how each develops its results (Price et al., 2017; Repko & Szostak, 2008).
The first step of our study used a social constructivist philosophy to conduct thematic narrative inquiry on stories told by adults about their loneliness experiences. It used our interdisciplinary theory to frame narratives. Through story, this approach examined overall patterns in whole social systems connected to feeling lonely. Results are descriptive in story form. We wanted to examine if any patterns could be found in adult loneliness experiences regarding the quality of whole social environments.
The second step used abductive reasoning to deepen explanation of how adult loneliness occurred based on our results. It recontextualizes the existing theory about a causal mechanism we identified in our interdisciplinary literature review to better reflect our findings (Price et al., 2017). This step interpreted our results through a critical realist lens. Unlike social constructivism, critical realism is primarily interested in improving explanation of the causes of events that adults experienced as loneliness (Bhaskar, 2016). It describes a ‘real’ world that is distinctly different from an individual’s experience of that world, or patterns in the world that are directly observable (Price et al., 2017). Larger social mechanisms or structures emerge in the real world that can explain how or why an event occurred, like how a social system pattern resulted in adult loneliness. Critical realism is amenable to interdisciplinary approaches when multiple disciplines are needed to understand the layered nature of reality (Price et al., 2017).
The following theory describe three interdisciplinary models identified in our interdisciplinary literature review (Bauer et al., 2025). They are complementary to fill in key gaps that theorize an underlying causal mechanism for how overall exposure to social interactions can be critical to an adult’s survival and health through loneliness. We combined the three models based on points of overlap in their knowledge (Figure 1) (Repko & Szostak, 2008). Theoretical Causal Mechanism Linking Loneliness to Health Outcomes Through Social Connection as a Human Basic Need.
The Social Exposome Model
The social exposome model was developed in environmental health and social epidemiology to capture the total exposure to social experiences that can impact an individual’s health outcomes (Gudi-Mindermann et al., 2023). It is important to our study because it describes a theorized causal pathway for how larger social structures, like culture and a political economy, can end up impacting the health of our bodies through direct social interactions. Direct social interactions are defined as the people or actors who are involved, the places where interactions occur, and the dynamics or qualities of those interactions. For example, a larger social process like a cultural message about a specific gender or race, can influence how people in a community end up interacting with that gender or race (Gudi-Mindermann et al., 2023; Krieger, 2016). Since the health and development of our nervous system seem dependent on social bonds, if individuals are exposed to harmful social interactions due to ideas about their race or gender, it can produce stress and may develop into dysfunction if it surpasses a critical threshold (Fulford & Holt, 2023; Krieger, 2016; Matthews & Tye, 2019). Social connection issues that drive loneliness in a way that is critical to human survival and health, would need to occur through direct social interactions according to this theory. It is not limited to only social interactions in personal relationships but encompasses any interaction between two or more people.
The Cognitive Discrepancy Model
The Cognitive Discrepancy Model suggests that what matters in direct social interactions to cause feelings of loneliness, is their quality. This model is commonly referenced in loneliness research and social psychology to suggest that loneliness is a signal when there is a discrepancy between the quality of relationships one has compared to the quality of relationships that one wants (HHS, 2023). The discrepancy has both been described as a purely subjective determination as well as an automated feedback mechanism in human physiology (Cacioppo & Patrick, 2008; Fulford & Holt, 2023).
Using the same data and population as this study (N = 219), in a prior study (in review) we identified four specific qualities in direct social interactions that resulted in adult loneliness: Rejection of Who I Truly Am, Excessive Labor, Present But Emotionally Absent, and Grieving Relational Loss. These four poor qualities were being compared to only one positive quality: Being Cared For. However, the method of thematic analysis that we used in the study was only able to describe the discrepancy in relationship quality as an immediate cause of feeling lonely during a social event. Results from this study suggested a need to examine the whole social environment of lonely adults that could capture the dynamics of larger social processes and their relationships.
The Socio-Ecological Model
The Socio-Ecological Model compliments the other two models by organizing an entire social environment into strata that serve different roles in the social environment based on how they impact human development and health (Bronfenbrenner, 1977). For our study, we used the Socio-Ecological Model from the U.S. Centers for Disease Control and Prevention that contains three different strata to organize our social environment: relational to describe personal spaces and networks of friends and family, community to describe community settings and networks like school or work in which many social interactions are occurring, and societal to capture large and abstract social processes and structures like culture or policies in a political economy (U.S. Centers for Disease Control and Prevention, 2022). These three strata capture different scales of human social life, from the individual to a society. However, they should not be thought of as completely separate from each other. When combined they form a social system of interactions that occur across the strata in a dynamic way to ultimately impact an individual’s health (Bronfenbrenner, 1977; Meadows, 2008).
Data Source and Study Population
Description of Data Source.

We collected secondary data from The Loneliness Project website. It was developed by a Canadian artist in an effort to destigmatize experiences of loneliness (Korda, 2017). The artist created an open-ended survey asking participants to tell stories about their lonely experiences and received over 2000 survey responses. In personal communication (January 12, 2023) she explained how she selected 300 responses to be publicly available on The Loneliness Project website. Survey responses were selected based on what she found to be the greatest diversity of topics found within loneliness stories, diversity of geographic locations of survey submissions, and diversity in self-identified ages (Korda, 2023). The selection process was not intended for scientific research.
We decided to conduct our study on survey responses from The Loneliness Project website because loneliness is often stigmatized to the point that it is difficult to recruit severely lonely people to participate in research (Barreto et al., 2022). The high participation of roughly 2000 individuals in the project and the artist’s explicit intention to destigmatize loneliness is useful in collecting information about loneliness that would have otherwise not been shared in research. It has been found that anonymous online communities can share more information about a stigmatized topic that is missing from research studies (Rains, 2014). Since our study is trying to understand loneliness as part of a shared human basic need for social connection, we also wanted to capture a wide range of views about the same health topic that are often found in stories shared online (Keim-Malpass et al., 2014). The validity of secondary data analysis in qualitative research is improved when the research question or aim aligns with the topic of data (Chatfield, 2020).
Our study had access to a total of 300 survey responses that were publicly available. Since loneliness experiences may differ across developmental stages, we limited our study sample to adults ages 18+ who can use the same measures of loneliness in population samples (Cole et al., 2021; Panayiotou et al., 2023). Survey participants only self-identified a first name and age, allowing us to select the 249 total survey responses that self-identified as being ages 18 or older. We tested our methods on an initial 30 survey responses. In conclusion, there were a total of 219 survey responses of adult ages 18 or over that we included in our study. Even though there is limited sociodemographic information about the study sample, the data aligned with our research aim to better understand loneliness as an indicator that a shared human basic need for social connection is not being met. Loneliness has been found to be a universal experience regardless of culture, sex, and language (Alsubheen et al., 2021; Hudiyana et al., 2022).
Analysis
There were two authors leading the analysis as an interdisciplinary research team. The lead author is an expert in population health research and mixed-methods, using a biology lens to understand how social environments impact health outcomes. Having worked in multiple health disciplines, they endorse a critical realist philosophy that rejects dualism between clinical and social science research that are both necessary to address social determinants of health. Their background is in both ecology and chronic disease prevention, in which key concepts from ecology about relationships in our ecosystem are often found to overlap with key concepts about relationships in the social sciences. This perspective places human beings as part of a natural world that is both real and interpreted.
The supervising author is an expert in qualitative research and narrative inquiry methods. She endorses a social constructivist philosophy that focuses on the collective meaning of stories in which adults communicate their identities and life experiences. With a background in clinical social work, she has engaged in the narratives that patients use to describe themselves as a way to examine alternatives that can improve relationships with oneself and others. Similar to the lead author, she is trained in systems science to consider how social environments result in health outcomes, but focusing primarily on mental health. This perspective considers the possibilities of human beings to improve their well-being and find meaning by re-constructing the world in which they live.
In the first step of our analysis, we conducted thematic narrative inquiry using a social constructivist approach to examine patterns of whole social systems resulting in adult loneliness. We adhered to the methodology described by Riessman, who is a leading expert in narrative inquiry. A narrative analysis was selected because it is designed to care about the context of stories rather than just the individual experience of them (Creswell & Poth, 2017). It aligns with our aim to improve understanding of an adult’s overall exposure to a whole social system during loneliness experiences. Since the secondary data we used are open-ended survey responses found online, we used narrative inquiry as a type of narrative analysis that can explore small stories. Small stories describe brief and everyday storytelling that can be about key events or shared experiences (Bamberg & Georgakopoulou, 2008). We specifically used thematic narrative inquiry to analyze the ‘what’ of small stories by framing them within theory, capturing the whole social environment of each story as a case-centered approach (Riessman, 2007).
We developed familiarity with the data as a research team and tested our methods on an initial 30 survey responses (Riessman, 2007). As a reminder, every survey response on The Loneliness Project website was answering four different prompts asking about loneliness experiences (Table 1). Even though these stories about loneliness often jumped in time, narrative inquiry analyzes all four survey prompts at the same time since they are told and interpreted when the participant fills out the survey (Riessman, 2007).
Survey responses were uploaded to ATLAS.ti 23 to organize them and the software was used to track labels. Three authors who conducted the analysis, including a research assistant, generated initial ideas for labels that could describe patterns in the overall social system that adults recounted as contributing to their feelings of loneliness. We defined it as labeling that is distinctly different from coding, because they were not used to break up a story into key concepts. Instead, labels in thematic narrative inquiry kept a whole story intact to answer what the story communicated about a research topic (Riessman, 2007). Labels were discussed as a research team at weekly or bi-weekly meetings from December 2023 to May 2024. Key decisions around definitions and patterns were tracked in an audit trail. The final labels were again discussed after all 219 survey responses had been read by these three authors.
To make sense of our resulting labels, the lead author further refined them by developing each into a final narrative (Creswell & Poth, 2017). Final narratives included shared and significant patterns found across survey responses that had been highlighted by the research team during discussions. These patterns were explicitly framed within theory, which we illustrated through simple drawings (Figure 2). Our research team solely interpreted survey responses to identify patterns of social systems, not to interpret the composition of a social system. For example, we did not interpret specific cultural messages or institutional policies – they were explicitly mentioned in survey responses – we only interpreted patterns found across them. Each label and its final narrative were presented to all study authors for feedback. Example of Framing a Survey Response With Theory.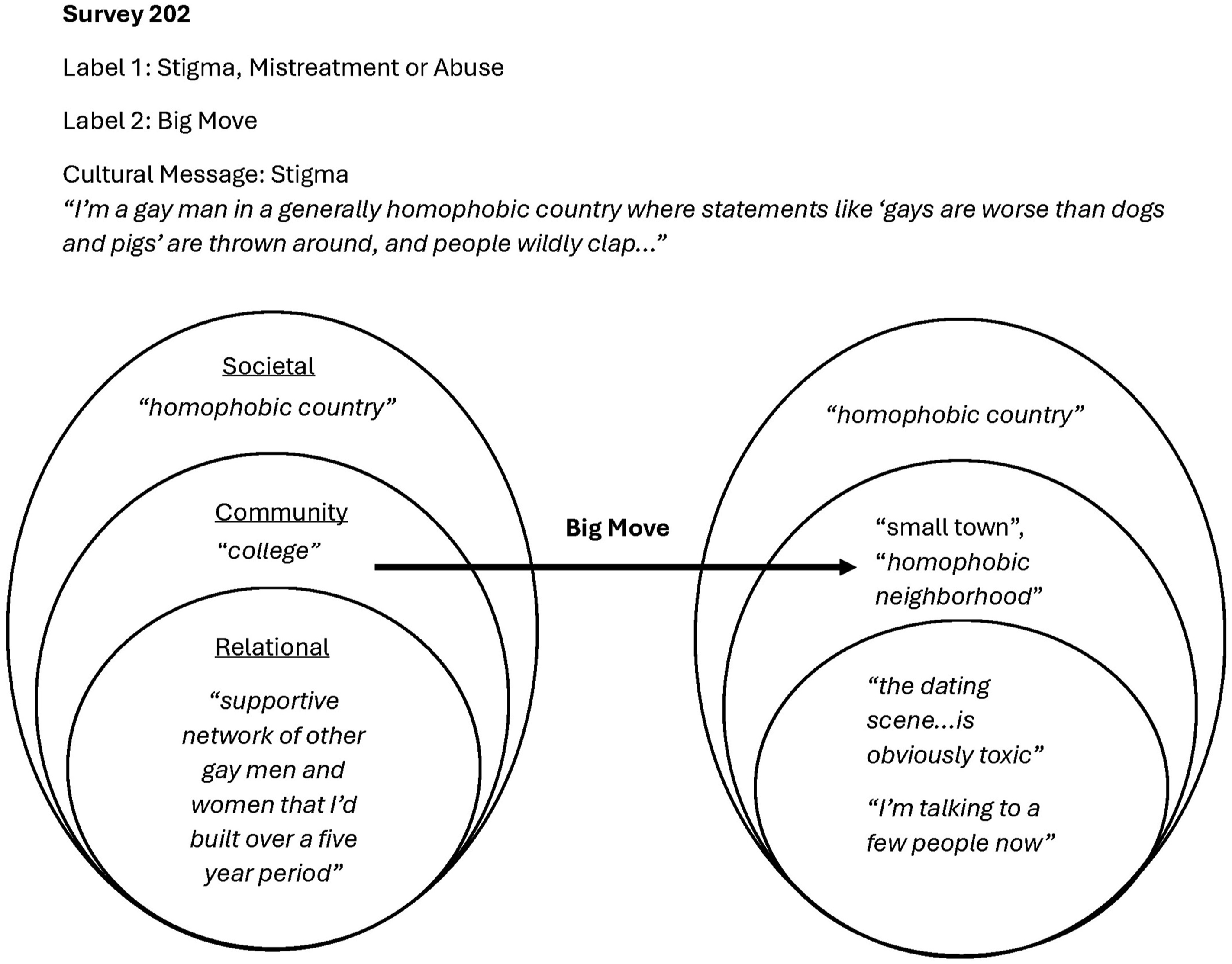
The second step of our analysis was developing our results beyond descriptions of the experiences and events of adult loneliness to deepen knowledge about the underlying causes that tend to produce these events. This distinction is known as the three domains of reality, that was developed by Bhaskar in critical realism (Bhaskar, 2016). We used abductive reasoning that is informed by Tavory and Timmermans to interrogate our results in relation to existing theory that has the power to explain the results as defined by critical realism (Price et al., 2017; Tavory & Timmermans, 2014). Abductive reasoning starts with an observation and then seeks a likely explanation. Tavory and Timmermans highlight the importance of this method in addressing theoretical tensions, and using unexpected results to improve upon existing theory (Tavory & Timmermans, 2014).
Two supervising research authors and the lead author identified existing theory with explanatory power, to understand what can explain adult loneliness and its increasing severity found in our results. We presented our results to all study authors for feedback.
Results
From thematic narrative inquiry on 219 survey responses, a total of 5 final narratives were developed from labels to describe five distinct social systems resulting in adult loneliness in our study sample. Major Health Problem; Big Moves & Small Families; Stigma, Mistreatment, or Abuse; Caregiving Beyond My Capacity; and Fitting In, are labels that describe the five narratives (Figure 3). The five labels with their narratives are briefly described below and fully detailed in Supplemental Material. Five Final Labels and Narratives Framed Within Theory.
Major Health Problem: A Social System of Physical Isolation
While loneliness is understood as an indicator of poor quality in relationships, Major Health Problem described how physical isolation could result in loss or an absence of social interactions across a whole society due to physical barriers to connection. Physical isolation often occurred when participants described the loss of their bodies due to physical or mental health issues, especially when a person became housebound or confined to a hospital, some losing contact with their entire social network over a long or uncertain period of illness. In illness, loss of control over one’s own body directly impacted the ability to have relationships with anyone. Examples included the loss of hearing and speech to communicate, the loss of safety in providing childcare due to unexpected seizures, or the loss of trusting oneself around others when diagnosed with bipolar disorder. Participants described feeling physically trapped in their homes, in their hospital rooms, and in their own bodies. If unable to join in on community life, participants could lose any exposure to a community. They additionally struggled with cultural messages of feeling like a burden or causing others discomfort when unable to work or having uncertain futures. The relationship most impacted was sometimes the relationship with one’s own body and feeling lost on how to socially connect with others moving forward. “I’m lonely because an illness I didn’t ask for, that is killing me, has left me homebound and uncomfortable to look at because it took too long for the doctors to catch it. Aside from when my boyfriend gets home from work, I spend my day entirely alone. And most of his time after work is running errands and cooking and picking up the slack so...Alone and a burden.” (Survey 146)
Big Moves & Small Families: A Social System of Social Isolation
Participants could also experience a total loss of their social network due to death and/or moving away that resulted in social isolation. Again, social isolation is known to be distinct from loneliness as a structural issue with the total quantity of relationships someone has, but when coupled with qualities like loss or emotional absence, did result in loneliness. While death is a permanent loss, moving away was still significant because those connections are no longer exposed to daily life together. Participants described the deterioration of a small and shrinking social network. It left participants feeling vulnerable, wondering what their future would be like. Participants described how the loss of a relationship was sometimes the last family member they had. Some described the long periods of time they would spend alone on evenings, weekends, holidays, or for significant life events. When participants experienced total loss of their last existing personal and community relationships, it could only be described as unmoored, or a complete disconnection. The reality of family and friend life for participants could be a challenging contrast to cultural expectations for having personal relationships. “In my home country, my city was the country‘s capital so there were always gigantic celebrations with families, relatives, friends, and I was invited to go to a lot of places to celebrate. Here in Canada, one of my parents has to work on either Christmas or New Year. It‘s sad because now, it’s just my parents, my younger brother and I during the holidays. My youngest brother passed away a few years ago and we already didn’t have a lot of people to celebrate it with in this new country.” (Survey 86)
Stigma, Mistreatment or Abuse: A Social System of Rejection
Loneliness included experiences of rejection, mistreatment, or abuse that led participants to feel that who they were was somehow wrong. The range of participants’ life experiences and identities that were stigmatized by others was vast: such as being a sexual or gender minority, being overweight, being single, or being an immigrant. These experiences were often in the context of personal relationships and could start in childhood. Religious beliefs, cultural beliefs and government or institutional policies were identified by participants as contributing to stigmas that showed up in social interactions with others and impacted the ability to form close relationships. For example, participants who identified as gay could not openly date due to cultural stigmas or national laws against homosexuality. One participant with HIV as a child experienced the distancing of relatives from forming relationships due to stigma around the disease, and did not receive family support to get needed medical care. Sometimes the lack of response by community members who witnessed a participant being mistreated was the main contributor to feeling lonely. “I’ve been lonely since I was very little. Maybe because I was sexually abused, other kids shied away from me. Maybe they sensed the blackness on my soul.” (Survey 120) “In elementary school, another girl I considered my close friend slammed my head into a wall in front of all my classmates. No one cared to even gasp or laugh…They all looked and looked away, continuing what they were doing as though nothing had happened.” (Survey 152)
Caregiving Beyond My Capacity: A Social System of Excessive Labor Demands
Work, both caretaking labor in personal relationships and paid labor at jobs, could take a toll on participants that contributed to loneliness. Caregiving included either being a primary caretaker for one or more persons, or sacrificing one’s own needs to care for others within any type of work. Participants discussed the hardship of excessive labor demands, that they sometimes hid to protect others. Excessive labor demands could reflect a lack of shared labor among relationships or reciprocity in being cared for by others. The responsibilities of caregivers stacked up with an inability to find support. Friends and family could be in similar situations and responding to the needs of others already. There may be a community or work culture that is in denial of problems. Participants identified a lack of formalized support, such as in social services or institutional care, and cultural expectations to sacrifice for others in demanding roles, leaving them to figure out how to meet demands on their own. “It means no relief from struggling alone to parent and pay the bills. It means guilt from going to bed asking God to let me not wake up.” (Survey 52) “Being an entrepreneur is really tough and very lonely…In tech startups, founders are 90% men who bluff their way along and never admit that everything isn’t great…I understand a little why a friend committed suicide. There was no one he could share what was really going on in his life.” (Survey 57)
Fitting In: A Social System of Emotional Absence
In loneliness, participants found a misalignment between themself and the dominant culture of people around them. There may be a misalignment in cultures, languages, social expectations, personalities, values, likes and dislikes, and life experiences. Participants acknowledged that there were people around and relationships in their life, but there was an absence of connection that could lead to unfulfilling social experiences. Not fitting in may go unnoticed by others, as outwardly a participant is spending time with others, but may sit in silence or not be engaged in conversations. This can be a lifelong experience, with some participants co-opting cultural terms to describe themselves, like “odd man out” or “weird”, that solidified their inability to connect with anyone around them. Or it could happen suddenly to participants, when a major life event changed relationship dynamics that made their identity or life experiences different than cultural expectations. “Not feeling part of the community even if you are within it. I am deaf and I work with all hearing people. No matter how much my boss knows about deafness, she still doesn’t realize that I miss a lot and I feel invisible at work, that I’m not worth more than just saying hi to.” (Survey 100) “My husband of 36 years died 18 months ago…I have no close friends who are single and couples just don't think about inviting me along when they go out.” (Survey 36) Processes Explaining Increasing Severity of Adult Loneliness.
We then used abductive reasoning to identify theory that could improve explanation of an underlying mechanism for how adult loneliness developed in all five social systems in our results and differences in severity. We examined the five social systems in combination, rather than separately, in order to recontextualize the theoretical causal mechanism for social connection as a human basic need that was described in the Materials and Methods section.
We found that within each social system, poor qualities in social interactions could accumulate across social strata and over time. The quality of social interactions that lonely adults experienced were centered around cultural messaging and the social expectations they established. In either social system lonely adults were not meeting social expectations when interacting with others, and the qualities of these interactions resulted in feelings of loneliness. We were able to identify patterns in cultural messaging, indicating dominant social narratives connected to social interactions lonely adults may experience across larger numbers of people. For example, survey participants often mentioned social interactions and their embedded messaging with groups of people, such as a whole family, a whole group of friends, a crowd in a community space, a whole institution like a workplace or religion, or even a whole society like a country. If poor qualities in social interactions grew across larger groups of people, lonely adults found themselves fracturing off to the margins of an entire society by themselves (Figure 4). When adults described severe or life-long experiences of loneliness, they were describing their overall relationship to the society in which they lived. To explain this emergent process, we identified the theory of marginalization. “…a disappointment and disconnect with the mainstream ways of the world.” (Survey 10) “It is the feeling of being on the verge of tears while the world is moving around you.” (Survey 83)
When re-examining the results across the 219 unique survey responses, though, more than one social system may be found in a single loneliness experience. Each social system reflected a specific pattern in poor quality that could be pervasive in social interactions across strata in society, reflecting different pathways to marginalization. These patterns could intersect in the social interactions that lonely adults experienced. At its most severe, all five patterns may cluster in social interactions. To explain this emergent process, we identified the theory of intersectionality. “…when I was sexually assaulted by a stranger…was in a period where I was losing touch with high school friends and struggling to make friends in college in a program I did not enjoy very much.” (Survey 184) “I was recently diagnosed with a mood disorder…My partner is afraid of me because I can’t check my reactions. I’m in treatment, but I don’t think it’s working, and I can’t return to intense psychiatric care until the end of the year or I’ll lose my job.” (Survey 211)
As described by Tavory and Timmermans when writing a manuscript about abductive reasoning, the development of our results are continued in the discussion section about marginalization and intersectionality (Tavory & Timmermans, 2014).
Discussion
Our results shed light on a key relationship not discussed in loneliness research, which is the relationship that an individual has to the society in which they live. The multidimensional theory of loneliness recognizes two to three subtypes of loneliness that depend on the closeness of a relationship (Anyan & Hjemdal, 2022). Romantic, family, and social loneliness describe a spectrum of intimacy in which loneliness can manifest differently, with social being a wide net that captures relationships with friends, colleagues, neighbors, and/or community members (Anyan & Hjemdal, 2022).
Our results suggest that social loneliness warrants further examination. As subtypes of loneliness have primarily been developed through a psychology or clinical lens that can emphasize personal relationships, our use of the socio-ecological model was able to capture the magnitude of social loneliness that adults described in our data. For example, we identified patterns in lonely adults describing a total loss of any social connection or a rejection of who they are by their country or institution to which they belong. When overwhelmed by social experiences resulting in loneliness, for example, adults conceptualized their relationship to “the world”.
It is unclear in our results how to define or delineate what a society or world is to which individuals relate, but it corresponds with biology knowledge about social species. Social species have been defined by their dependence on cooperation and group living in a society to survive (Wilson, 2000). Becoming separated from a society as an individual is known to be critical to survival across several social species (Wilson, 2000). It can be difficult to conceptualize a parallel, though, for how individuals in modern human life are separated from society, especially when discussing the relationship quality found in loneliness. One idea comes from the SOCIAL framework that has been suggested as a systems approach in public health to examine the quantity and quality of relationships across key sectors in society that are known to be critical to human health (Holt-Lunstad, 2022). It envisions eight sectors, one of which is clinical and population health, taking responsibility to support social connection across strata of society, through the services it already provides. In a positive way the goal is to permeate social connection interventions across society to address loneliness and social isolation epidemics (Holt-Lunstad, 2022). If the goal were reversed, one can imagine how an individual living in a society may experience an overwhelming separation.
Similarly, our results suggest that marginalization of an individual from society may be a way to experience separation, not through physical isolation alone, but through the quality of social interactions that increase severity of adult loneliness. Marginalization has struggled to be defined among the diverse disciplines and organizations concerned with addressing it (Fluit et al., 2024). One scoping review recently integrated its various definitions across 50 years of research, finding four distinct ways to think about it: 1) it is an active process of “othering” that is context-dependent on societal norms; 2) these norms reflect a center and othering is relegated to the margins beyond the center; 3) this process can result in lack of access to resources while simultaneously increasing exposure to adverse life experiences; 4) individuals within a marginalized population can experience varying degrees of marginalization, based on intersecting attributes (Fluit et al., 2024).
In describing marginalization, our results are inconsistent with prevailing ideas found in public health. We identified five social systems in our data that each describe a pattern of poor quality that can accumulate across strata of society and over time, a quality that was informed by dominant social narratives. For example, a stigma about an identity or life experience could inform social interactions in which an individual with that identity or life experience is rejected. While this example could be described as “othering”, dominant social narratives across the five social systems could include positive or mixed values in messaging. Messages that celebrate parenthood or caregiving, for example, were described by parents and caregivers overwhelmed with the labor of their responsibilities. Messages celebrating how to spend holidays with family members excluded adults who did not have relationships with any family. Our results align better with recent research that found breaking with social norms could describe loneliness experiences across cultures (Heu, 2023). We found dominant social narratives in our study to establish social expectations that adults could not meet, whether expectations were intended to be harmful or not, influencing the quality of interactions those adults experienced across strata in society.
Othering may be emphasized in public health, because marginalization is described in the social determinants of health framework to identify ways of addressing disparities in population health outcomes that can be driven by societal structures (Shultz et al., 2023). In updates on how marginalization is understood within this framework, there is an emphasis that being relegated to the margins of society is an active process of a dominant system exerting power over vulnerable populations (Baah et al., 2019). Even though marginalization is understood as being context dependent, static categories have developed in different countries to describe populations found to be high-risk for marginalization, such as by race, ethnicity, gender, or immigration status (Fluit et al., 2024). Our results also included individuals who are thought of as vulnerable based on sexuality, gender, disability, immigration status, and more. However, an important difference in our results is they describe the process of an individual being marginalized in any population, and their experience is not static. This suggests that while marginalization may be more likely to occur in vulnerable populations, it does not exclude the possibility that it can occur to any individual and can change depending on their social context.
We found in our study that some identities associated with loneliness are not static, such as the identity of being single or having low-income, and the social contexts of identities are not static, such as a gay man being rejected in his hometown and accepted in a university community. Resources such as a sufficient income and an existing network of personal relationships were also not guaranteed to prevent marginalization in our results. For example, one participant in our study sample started at an income, job, and friends, that they described as satisfactory, but after an injury, was unable to continue performing their job, forcing them to retire early and drop to a low-income bracket. Over time they were unable to maintain a social life with their existing friends who were in a higher income bracket. They ended up physically isolated at home with their injury and socially isolated with a total loss of exposure to work, community, and personal relationships. An unexpected life event could snowball an individual into an increasing degree of marginalization, even if they had not started there.
This touches on the concepts of intersectionality and accumulated exposure to adverse life events that are included in marginalization (Fluit et al., 2024). Again, the concept of intersectionality in public health or healthcare tends to focus on identities found in demographic measures, like the intersection of gender, race/ethnicity, and class of an individual, to explain worsening disparities in health outcomes and suggest further care or program considerations for vulnerable populations (Oudshoorn et al., 2025). A shift in focus has been encouraged to address macro-level systems and structures of privilege and oppression, like colonialism and sexism, that are shaped by power to drive inequity in populations (Hankivsky et al., 2014). This focus defines intersectionality within a dynamic external environment and context of individuals, as ways that multiple forms of inequity can interact at different scales (Fort et al., 2023).
Our results align with both concepts of intersectionality to some degree. When adults in our study sample described being stigmatized for an identity or life experience they had, the social system they experienced could include intentional oppressive systems, such as a country law banning their existence or a religious taboo against their life experience. However, intersectionality in our results described multiple pathways to marginalization, only one of which included stigma, and the role of power can be unclear.
For example, one participant in our study sample identified as a physician. Physicians have not been described as a vulnerable population in public health. In provider-patient dynamics or physician-staff dynamics they are often believed to hold power. However, the participant described their loneliness as resulting from both excessive labor demands in 24-h or more work shifts and the mistreatment they and their colleagues experienced from patients, nurses, and supervisors to the point of having suicidal thoughts. We labeled this experience as intersectionality because we found excessive labor demands and mistreatment due to stigma to be distinctly different patterns of marginalization across loneliness experiences in our study sample.
Last, the five pathways to marginalization we identified in our results - physical isolation, social isolation, mistreatment due to stigma, excessive labor demands, and emotional absence while not fitting in – could be developed to measure marginalization and risk for loneliness in social environments, rather than demographics. Marginalization has been described geographically to recognize how it can be intertwined with places, visibly seen in certain zip codes or areas of a community with a clustering of poor health outcomes and lack of resources compared to nearby populations (Fluit et al., 2024; Shultz et al., 2023). This approach has helped identify severe forms of marginalization connected to socio-economic status like poverty (Schiltz et al., 2022). Our results suggest that severe marginalization is not always visible or tied to socio-economic status. Considering five ways of measuring a social environment may improve identification of high-risk places and social organizations for severe and chronic loneliness in populations.
Future research may improve upon our study by collecting primary data that has greater detail about adult loneliness experiences. Since our data came from an online platform that focused on destigmatizing loneliness experiences, we had insufficient information about protective factors against loneliness or reversals in loneliness experiences that could be addressed in future research. While some researchers may want to examine each social system we described in better detail, we also encourage research on populations larger than our study sample to maintain a perspective in how results apply to social connection as a human basic need. We found the secondary data we used to be a helpful starting point in understanding loneliness as part of the human basic need for social connection. As we work toward bridging divides in knowledge between biology and the social sciences, researchers may improve upon our approach using the same publicly available data.
Limitations and Strengths
Our interdisciplinary approach included two steps with competing philosophies of science. We found common ground in our methods by using interdisciplinary theory that includes shared biology and social science knowledge about social connection as a human basic need. While we identified the same results in our research team despite endorsing different philosophies of science, the interpretation of those results may differ. Social constructivism may interpret marginalization and intersectionality as solely social constructions capable of change and a unique way of understanding loneliness from the survey participants in our data (Riessman, 2007). Critical realism may interpret results to improve upon existing theory about loneliness to reflect how it can be produced in a real world that is stratified, dynamic, and emergent (Bhaskar, 2016; Price et al., 2017). Critical realism encourages interdisciplinary research to solve problems in a real world, but would suggest further alignment in the ontology and epistemology of the interdisciplinary theory and methodology we used to improve our results (Price et al., 2017).
Since our study uses interdisciplinary theory about social connection as a human basic need, generalizability is an important consideration. It is beyond the scope of this study to address generalizability because participants are anonymous and there was no indication in our thematic narrative inquiry that a form of saturation had been reached even with 219 survey participants.
Secondary data that was analyzed in our study was also selected to be publicly shared by an artist. The selection process was aimed at sharing diverse perspectives about a universal human experience, but those who submitted survey responses may be different than lonely persons who chose not to submit a survey response. Our results are specific to the study sample and are intended to inform theoretical knowledge.
Our results are limited to understanding the social environment of lonely adults without acknowledging their agency and contributions to the societies in which they live (Price et al., 2017). We wanted to first focus on what we could understand about the broader social systems of adult loneliness before introducing more complexity to our results. Addressing loneliness will require a more thorough understanding of the agency of lonely adults and the interplay between agency and society.
Conclusion
Using a critical realist lens to better understand adult loneliness, we identified the process of marginalization and the accumulation and intersectionality of adverse life experiences to explain the increasing severity of adult loneliness. By incorporating interdisciplinary theory about social connection as a human basic need, our results work toward bridging a divide between biology and the social sciences to understand how adult populations may develop severe and chronic loneliness.
Lonely adults described their relationship to the societies in which they live. We identified five specific pathways to marginalization, in which this relationship could be fractured as lonely adults were increasingly excluded from a whole society. These pathways included physical isolation, social isolation, mistreatment due to stigma, excessive labor demands, and emotional absence while not fitting in. Improving clarity around at least these five pathways could improve guidance in public health on how to develop interventions for inherently lonely places and social structures, when adults are facing severe and life-long loneliness in our communities.
Supplemental Material
Supplemental Material - Marginalization and Intersectionality in Adults’ Relationship to Society Explain Increasing Loneliness: A Critical Realist Lens on Thematic Narrative Inquiry
Supplemental Material for Marginalization and Intersectionality in Adults’ Relationship to Society Explain Increasing Loneliness: A Critical Realist Lens on Thematic Narrative Inquiry by Kyla L. Bauer, Sarah Eskew, Gregory Tung, Jenn A. Leiferman, Meredith P. Fort, Beth M. McManus, and Rachel A. Johnson-Koenke in International Journal of Qualitative Methods
Footnotes
Ethical Statement
Author Contributions
Conceptualization – Original Design, KLB, RAJK; Conceptualization – Review & Editing, GT, JAL, MPF, BMM; Methodology, KLB, SE, RAJK; Formal Analysis, KLB, SE, RAJK; Resources, All Authors; Writing – Original Draft Preparation, KLB; Writing – Review & Editing, All Authors; Supervision, RAJK.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is supported in part by the NIH/NCATS Colorado CTSA Grant Number UL1 TR001082.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.