
Abstract
This paper outlines the application of Experience-Based Co-Design (EBCD) to explore the perspectives of older adults living with HIV regarding virtual geriatric care. The study focuses on identifying the unique needs, challenges, and preferences of this population in the context of remote healthcare delivery models. EBCD, a participatory research method, engages service users, healthcare providers, and stakeholders in co-designing solutions to improve healthcare services. By involving participants throughout the research process, the approach ensures that resulting interventions are informed by real-world experiences, enhancing their likelihood of acceptance and effectiveness. The methodology includes in-depth interviews, focus groups, and journey mapping with older adults living with HIV to gather data. Through collaborative discussions, care gaps were identified, and key areas for improvement in virtual care were highlighted. Active participation from healthcare professionals ensured that these findings were translated into actionable solutions. Practical insights were also gained on fostering an inclusive and respectful environment for marginalized populations, ensuring that their voices were central to the co-design process. This study demonstrates that EBCD is an effective method for engaging older adults living with HIV in the design of virtual care interventions, leading to patient-centered solutions that address both clinical and psychosocial needs. Key contributions of the study include the development of a framework for applying EBCD in virtual geriatric care, identification of critical care gaps in this context, and the promotion of inclusive practices for vulnerable populations. The findings suggest that EBCD can play a significant role in advancing health equity and improving the quality of care for older adults living with HIV, especially as virtual healthcare continues to evolve.
Introduction
Since the advent of antiretroviral therapy (ART), HIV has transformed from a fatal diagnosis into a manageable chronic condition (Edelman et al., 2013). However, as people with HIV age, they experience a complex array of both physical and mental health challenges, including multiple comorbidities such as cardiovascular disease, diabetes, cognitive decline, frailty and mental health challenges (Courlet et al., 2019; Gates et al., 2018; Guaraldi et al., 2019; Sarma et al., 2023; Shippy & Karpiak, 2005; Solomon et al., 2014). These individuals also contend with the cumulative effects of long-term HIV treatment, stigma, and social isolation, which can exacerbate physical and mental health conditions (Brown & Adeagbo, 2021). For older adults living with HIV, healthcare needs extend beyond traditional HIV care, and there is a growing recognition of the need for comprehensive, geriatric-focused services that address these intersecting health and social concerns (Kokorelias et al., 2023a).
Collaborative care models that bring together HIV specialists, geriatricians, primary care providers, and mental health professionals can ensure that older adults with HIV receive comprehensive and coordinated care (Kokorelias et al., 2023a). This team-based approach is especially important for addressing the overlapping challenges of aging and chronic HIV management, improving health outcomes, health literacy and enhancing the quality of life for older adults living with HIV (Sangarlangkarn et al., 2017; Varadarajan et al., 2024). In Canada, however, best-practice models of geriatric-HIV care have not yet been established (Kokorelias et al., 2023a) This gap in care is particularly pronounced in rural areas (Kokorelias et al., 2023a, 2023b) where access to specialized geriatric and HIV services is limited due to a shortage of geriatricians and other relevant specialists (Kokorelias et al., 2023a). Yet, even in urban centers, geriatrician knowledge of managing HIV and its associated complexities, including long-term treatment effects, comorbidities, and psychosocial challenges, is often insufficient (Hughes, 2011; Jones & Barber, 2022; Levett et al., 2014). Thus, access to geriatricians with specialist knowledge remain scarce.
One innovative solution to these challenges is the implementation of virtual HIV models of geriatric-HIV care, that leverage technology to enhance accessibility and integration of services (Kokorelias et al., 2023a). Virtual models can play a critical role in addressing barriers such as geographic constraints to limited specialist providers, mobility limitations, and the stigma often associated with in-person clinic visits (Farooq et al., 2024). These models enable patients to connect with multidisciplinary healthcare teams—including HIV specialists, geriatricians, primary care providers, and mental health professionals—via telemedicine platforms, thereby facilitating the collaborative care necessary for managing the complexities of aging with HIV (Farooq et al., 2024; Zinck et al., 2022).
Older adults with HIV represent a heterogeneous population, characterized by diverse cultural backgrounds, socioeconomic statuses, and lived experiences (Crystal et al., 2003; Gari et al., 2013). These factors significantly influence their health outcomes, (Aidala et al., 2016) care preferences (Gari et al., 2013; Saha et al., 2013) and engagement with healthcare services (Freeman et al., 2017). Yet, current models often fail to account for these sociocultural nuances, risking inequitable access to and effectiveness of care (Kokorelias et al., 2023a). Incorporating the perspectives of patients, caregivers, and healthcare providers into the design process can ensure that virtual care models reflect the unique needs and values of the populations they serve. One way of addressing the diverse needs of older adults living with HIV is through co-design of virtual HIV models of care that are sociocultural responsive and inclusive (Kokorelias et al., 2023a).
Co-design is a participatory research approach that actively involves end-users in the design and development of programs, services, or interventions (Brown et al., 2024; DiGioia & Shapiro, 2017; Donetto et al., 2014; Robert et al., 2013). Unlike traditional top-down models, co-design fosters collaboration by ensuring that solutions are informed by the lived experiences and needs of those most affected by the issue being addressed (Brown et al., 2024; Donetto et al., 2014). Core principles of co-design include mutual respect, shared decision-making, capacity building and iterative feedback, which together create an inclusive process that is responsive to diverse perspectives (Brown et al., 2024; DiGioia & Shapiro, 2017; Donetto et al., 2014; Robert et al., 2013). By emphasizing the engagement of older adults living with HIV, co-design aims to produce contextually relevant, effective, and equitable outcomes that are more likely to be embraced by the community (Brown et al., 2024). At the same time, engaging participants in participatory research practices, such as co-design, requires trust-building and inclusivity, especially for populations that have historically faced discrimination in healthcare settings (Christopher et al., 2008; Jagtap, 2022; Lucero, 2013). Likewise, a common issue is tokenistic involvement, where participants are invited to participate in name only, without meaningful opportunities to influence decisions or outcomes (Jackson et al., 2020; Romsland et al., 2019). Lastly, many traditional research practices have been criticized for being extractive (Igwe et al., 2022), particularly in the way they engage with communities and participants (Wilmsen, 2008). In such cases, participants invest time, knowledge, and emotional labor, but the benefits of the research—such as improved programs, policies, or interventions—rarely flow back to them. Instead, the research findings are frequently disseminated in academic settings/formats with little regard for how they can be shared with or applied to benefit the communities involved. This approach not only perpetuates power imbalances between researchers and participants but also risks producing interventions that fail to address the lived realities of those they aim to serve.
This paper aims to address these barriers by sharing the practices and strategies we employed in our co-design process to create virtual HIV models of care that are socioculturally responsive and inclusive (Kokorelias et al., 2023a) We adopted an iterative approach to our research methodologies, integrating continuous feedback from participants to refine the research process and build trust throughout the process. By detailing our methods and the lessons learned, we hope to provide a practical framework for researchers and practitioners seeking to overcome similar barriers in the development of equitable and effective care models for older adults living with HIV.
Methodology
A protocol for our methodology has been published elsewhere (Kokorelias et al., 2023a) Briefly, this study used an Experience-Based Co-Design (EBCD) approach, a participatory method widely used in health service research to enhance healthcare services by actively engaging patients and families in the design process (Donetto et al., 2014). The study was guided by intersectionality frameworks (Crenshaw, 2017) and the Knowledge to Action (KTA) Framework (Graham & Tetroe, 2010). The intersectionality framework ensured that the research considered the complexities of overlapping identities, including race, gender, and socioeconomic status, while the KTA framework helped facilitate the translation of research knowledge into practice (Kokorelias et al., 2023a).
To take part in the study, individuals must have self-reported as HIV-positive, be 50 years old or older, and live in Ontario. For participant recruitment, purposive and quota sampling methods were combined to ensure a diverse and representative sample, including individuals from various gender identities, sexual orientations, racial and ethnic backgrounds (Acharya et al., 2013). The research team actively sought participants from community-based organizations, religious institutions, and culturally-oriented events to engage diverse populations, particularly those who may not have traditionally been included in research.
The study was conducted in three phases (Kokorelias et al., 2023a). Phase 1 involved semi-structured focus groups or one-on-one interviews to gather insights from participants regarding their healthcare experiences, including critical points along their illness trajectory, transitions between care settings, and needs related to receiving geriatric care (Kokorelias et al., 2023a). Participants selected their preferred interview format (in-person, phone, or videoconference). Each interview ranged from 50 to 82 min (with an average duration of 62 min), was transcribed verbatim, and was followed by an optional demographic survey. Phase 2 focused on co-designing strategies to improve existing geriatric care models and create an innovative virtual care model that was culturally appropriate (Kokorelias et al., 2023a). This phase employed a modified 3-D cycle of Appreciative Inquiry, a strengths-based approach aimed at amplifying positive experiences to foster growth and sustainable change (Kokorelias et al., 2023a; Trajkovski et al., 2013). Participants worked together to envision an ideal future for geriatric-HIV care, identify key elements of a new care model, and create design principles for a virtual care approach (Kokorelias et al., 2023a). This phase lasted 2 hours per session and occurred in person.
Phase 3 aimed to refine the design principles by engaging participants in discussions and workshops to explore barriers and facilitators to implementation and provide feedback on the proposed solutions (Kokorelias et al., 2023a). This phase used a World Café format to encourage dynamic conversations and cross-pollination of ideas (Banfield et al., 2022). Participants helped refine the virtual care model, creating a unified set of recommendations for implementation (Kokorelias et al., 2023a). The research team worked collaboratively with the advisory committee, incorporating feedback from participants to refine the findings and design principles. This phase lasted 4 hours per session and occurred in person.
Nineteen unique participants participated in Phase 1 (n = 14) or Phase 2 or 3 (n = 12). Seven people participated in all phases of the study. Participants ranged in age from 50 to 80+ years, with the majority falling into the 50–54 age group. In terms of gender, the group included 10 men, 6 women, 1 transgender individual, 1 non-binary participant, and 1 Two-Spirit participant. Geographically, the participants were from a mix of urban (14), suburban (2), and rural (3) living settings, reflecting a broad representation of Ontario’s population. The study included participants from diverse countries of birth, with 8 individuals born in Canada and others originating from countries such as the USA, Guyana, Vietnam, Israel, Uganda, India, Zimbabwe, Trinidad and Tobago, Italy, and Armenia. The length of time these participants had spent in Canada varied, with the largest group (8 participants) having lived in the country for their entire lives, while others had resided in Canada for varying periods, from 0–5 years to over 10 years. In terms of language and ethnicity, most participants (10) identified English as their first language. Ethnically, the group was diverse, with a significant number identifying as Asian (East Asian, South Asian, South East Asian), Black (African and Caribbean), White (European and North American), and mixed heritage. A few participants also identified as Indigenous or Latin American. Household income levels were distributed across various brackets, with 12 participants earning under $30,000, and fewer participants in higher income categories.
Ethical considerations were central to the study, particularly given the sensitive nature of the healthcare topics addressed, such as aging and HIV. The research team ensured that participants had flexible participation options (e.g., one-on-one interviews or focus groups, virtual or in person options) and were supported by trauma-informed clinicians throughout the process. Confidentiality was maintained through secure data handling practices, and participants were equitably compensated for their involvement. The study was submitted to a research ethics board Sinai Health Research Ethics Board (REB: 23-0106-E).
The research team consisted of Canadian researchers with expertise in HIV, equity-informed healthcare, health service research, and implementation science, as well as clinicians (including physicians in geriatrics, family medicine, and infectious diseases, occupational therapists, and social workers), trainees (PhD and medical students), health service administrators, and peer-researchers with lived experience, aimed to co-design a culturally appropriate virtual model of geriatric-HIV care.
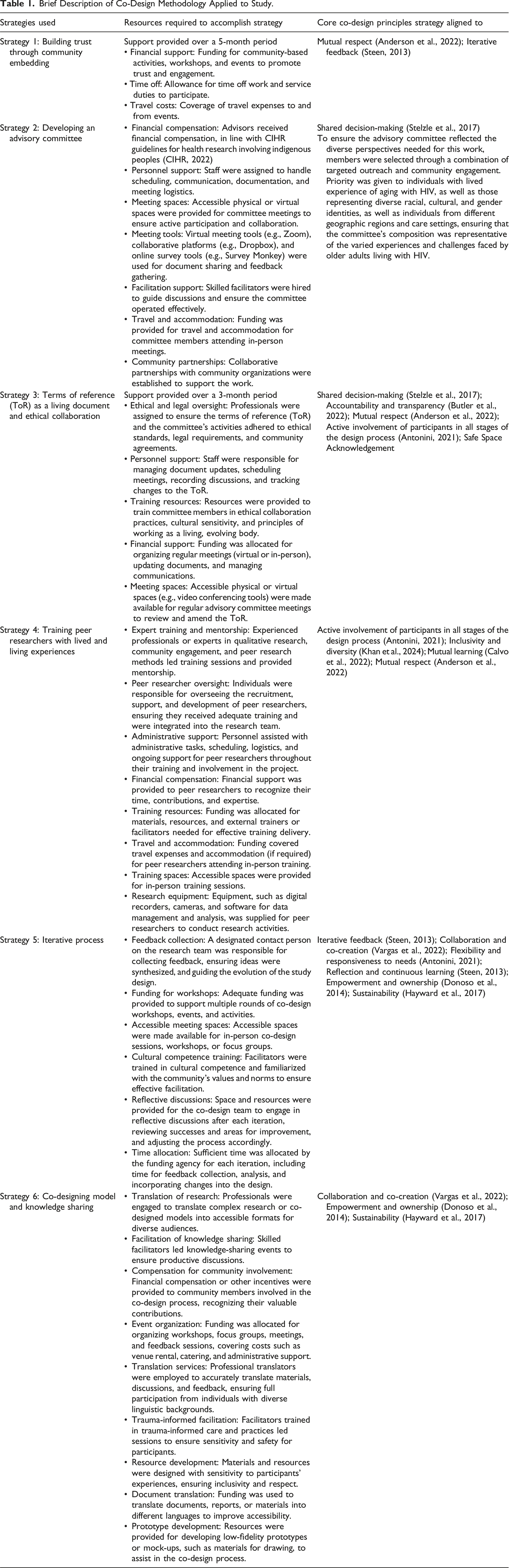
Brief Description of Co-Design Methodology Applied to Study.
Outcomes of the EBCD Approach
Strategy 1: Building Trust through Community Embedding
Our approach to this research was rooted in a deliberate and sustained effort to build trust and understanding within the community of older adults living with HIV in Toronto, Ontario. This was prior to applying for grant funding and sustained over the course of more than a year. Engaging the community early ensured that their voices shaped the study from its inception, aligning with co-research principles that emphasize collaboration in research design—including the development of funding applications. This groundwork not only strengthened our funding proposals by demonstrating genuine community engagement and the relevance of our research questions but also helped us establish meaningful partnerships with key stakeholders. During this time, we immersed ourselves in the environments frequented by older adults living with HIV, such as community centers, shelters, health centers, clinics, and social events, such as those that target stigma. These events were known to the research team through connections built prior to the research. For example, we volunteered our time at these clinics, participated in community initiatives, and attended workshops and events focused on raising awareness about HIV and aging. We spent time in informal settings, such as having coffee and engaging in casual conversations in spaces where older adults gathered, as lay persons rather than researchers. Additionally, we collaborated with local organizations to co-host events, observed routine activities in these environments, and actively sought opportunities to build trust and rapport with the community by consistently showing our commitment to understanding their experiences. Importantly, we did not approach individuals directly or impose our research agenda; instead, we allowed relationships to develop organically. By consistently showing up—2 times a month for a 5 month period—across various locations, we became familiar faces in these spaces. Financially, this initial work was supported through general research funds. Our presence was intentional yet unobtrusive--emphasizing authentic engagement rather than formal research roles (i.e., as study participants). For instance, we shared personal stories, engaged in casual conversations about everyday topics like hobbies and community news, and showed genuine interest in the lives and perspectives of the individuals we met. These informal conversations, initiated by community members themselves, provided invaluable insights and laid the foundation for this project. No data was collected or analyzed during this time period. Many of these conversations began organically, often when we were simply present in the community spaces, participating in activities or having casual discussions with others. Community members would approach us after seeing us consistently return to these spaces or through word of mouth from others who had interacted with us previously. We were transparent about our intention to learn from the community and make sure their voices were central to any future research. Public and patient involvement within co-design involves engaging patients as lay advisers to ensure that research remains relevant and accessible to individuals like them (Louise & Annette, 2019). Importantly, those involved in public and patient involvement are not research participants but rather collaborators in the research process (Louise & Annette, 2019). Unlike qualitative research that explores patient perspectives, patient and public involvement does not originate from an academic tradition but is instead rooted in the consumerist movement and efficiency discourse (Louise & Annette, 2019).
As trust grew, individuals began to share their experiences, challenges, and perspectives on living and aging with HIV. Once individuals knew of our connections to hospitals and clinics, they described the need for improved geriatric care. These conversations became the catalyst for identifying gaps in existing care and conceptualizing the project idea. Before applying for grant funding, we engaged in extensive dialogue with community members about potential methodologies, ensuring that our approach was both feasible and respectful of their lived realities. We were transparent about the limitations of our research funding, including its boundaries and the challenges of translating findings into practice. We openly discussed the reality that the funding available for the project was limited and would influence the scope and scale of the work we could accomplish. For example, we explained that while we hoped to gain valuable insights through the informal conversations and community engagement, the scope of the project would primarily focus on understanding key themes, rather than providing immediate, large-scale interventions or systemic changes. We also mentioned we were limited in how many participants we would recruit and from where in the region of Ontario we’d be able to travel to meet individuals from.
This extended period of engagement allowed us to collaboratively shape a project that was grounded in the community’s actual needs rather than assumptions. However, it also presented several challenges, particularly regarding the limitations of resources and the complexity of balancing community engagement with research timelines. One of the primary challenges was the time and effort required to establish and maintain trust within the community, which is essential for meaningful engagement. This process took longer than anticipated, as we were navigating the complexities of relationships, understanding community dynamics, and ensuring that we did not come across as opportunistic or intrusive, while also balancing the demands of research-careers. Another challenge was the difficulty in ensuring that our research design and methods were truly reflective of the community’s needs and priorities. For example, numerous individuals shared with us the concerns of our work only capturing urban perspectives. While we had the best intentions to recruit individuals from rural Ontario, we were constrained by the funding available, which limited the resources available to support the travel and accommodations of individuals from outside of Toronto for in-person focus groups.
These informal conversations, though not formally recorded or analyzed, provided invaluable insights that shaped the direction of our research design. While no data was collected at this stage, we ensured that these community-driven insights were respected and appropriately incorporated into the project’s development. This was done by including community members in the development of the grant proposal and research protocol, ensuring their perspectives were formally recognized in the study framework. Additionally, we provided transparency about our goals and integrated their feedback into the foundational stages of the project.
Strategy 2: Developing an Advisory Committee
To ensure our project was rooted in lived experience, practical expertise, and policy relevance, we developed an Advisory Committee comprised of diverse knowledge users. The committee included three administrators from non-profit, community-based organizations that provide support to older persons with HIV (e.g., shelters, healthcare organizations, charities, and community centers), two older adults living with HIV, five clinicians with experience working with this population, policy-makers, and members of the research team (Kokorelias et al., 2023a). This structure was designed to bring together a broad spectrum of perspectives, ensuring our project addressed the multifaceted needs of older adults with HIV while grounding our work in practical, real-world applications.
The Advisory Committee was deliberately constructed to reflect the intersectionality inherent in the lives of older adults with HIV. We began by reaching out to individuals who had expressed interest during our community engagement phase. To ensure inclusivity and further diversify the committee, we invited these individuals to recommend others who could provide valuable insights. This snowball approach strengthened trust and reinforced the collaborative nature of the project. While we aimed for a broad spectrum of voices, there were instances where we had to turn down potential members because their experiences or social identities were already well-represented on the committee. This decision was made with care, ensuring that it did not negatively impact relationships we had built during phase 1. Instead, it was an opportunity to be transparent about the committee’s composition and reaffirm our commitment to inclusivity while maintaining a balanced and productive dialogue. In cases where we received more interest than anticipated, we navigated the situation by considering how additional members could add value without compromising the group’s dynamic. The relationship-building work done in phase 1 made it easier to communicate with those whose involvement we had to limit. We could explain our reasoning in a respectful manner, emphasizing that the decision was made to maintain a diverse yet manageable group, and offering other ways for individuals to stay engaged in the project, such as through consultations or ongoing feedback mechanisms.
Recognizing the importance of respecting individual preferences and contributions, we invited Advisory Committee members to decide on their roles, titles, involvement, and authorship preferences on publications, reports and conferences. This flexibility acknowledged their autonomy and ensured that each person’s involvement aligned with their comfort and aspirations. Some members chose to identify as “peer-researchers,” reflecting their active role in the research process and their lived experience (Eaton et al., 2019). Others preferred to retain titles aligned with their professional roles or community affiliations. Many, simply wanted to use their names.
The Advisory Committee played a central role in the project’s success, particularly in ensuring integrated knowledge translation (IKT) (Bowen & Graham, 2013). Members were actively involved in every stage of the research, from refining methodologies and validating findings to co-developing strategies for disseminating and implementing results. Their lived and professional expertise informed how findings were interpreted and shared with various audiences, including policy-makers, practitioners, and community organizations. Furthermore, the committee was instrumental in planning for the practical application of findings. This included advising on how insights from the study could be incorporated into ongoing programs and policies to improve care for older adults living with HIV.
Strategy 3: Terms of Reference as a Living Document and Ethical Collaboration
A critical part of establishing trust and transparency with our Advisory Committee involved developing Terms of Reference (TOR) as a living document (Munce et al., 2024). The TOR served as a foundational agreement that outlined the expectations, responsibilities, and guiding principles for all members’ involvement in the project. It was collaboratively created through an iterative and inclusive process, ensuring that all members had the opportunity to contribute, review, and approve its content. We worked on the TOR until every Advisory Committee member was fully satisfied with its provisions. This process took over 3 months, as we engaged in multiple rounds of discussions and revisions to ensure that each member’s input was considered and incorporated. This approach demonstrated our commitment to shared ownership, inclusivity, and shared decision-making throughout the project. During this process, however, we had to consider power imbalances that emerged during conflicting opinions within the Advisory Committee. In situations where debates were necessary, we were mindful to ensure that each voice was heard and that no single member dominated the conversation. We worked actively to create an environment where members could express differing views in a respectful and equitable manner. For example, when stronger or more experienced voices emerged, facilitators ensured that those with less experience or quieter voices had equal opportunities to contribute, either by directly inviting input or through written feedback options.
The TOR included key aspects such as compensation, members’ rights, meeting schedules, anonymity, authorship, the use of data, and confidentiality. These elements were essential in setting clear boundaries and expectations while promoting transparency and respect. Every item was discussed thoroughly to ensure mutual understanding and alignment with ethical research principles. Members were invited to provide feedback at each meeting to assess whether changes were needed, and any Advisory Committee member had the right to request revisions at any time. This iterative review process reinforced the idea that the TOR was not static but rather a living agreement that evolved in response to ongoing dialogue and feedback.
An important component of this process involved discussing language—both the terminology used and the way concepts were expressed. We prioritized clear, accessible, and inclusive language that reflected the diverse experiences and expertise of all members while ensuring clarity for participants and other stakeholders. This attention to language was crucial in maintaining respectful communication and ensuring that all perspectives were heard and understood.
From an ethics perspective, our goal was to ensure the protection of participants, the confidentiality of shared information, and the transparency of the research process. The Terms of Reference and the collaborative development of the Research Ethics Board application reflected these goals. Through this ethical framework, we ensured that all members understood their roles, responsibilities, and rights within the research. Clear, plain language was prioritized to ensure that all members and participants could engage with the research process without confusion, thereby fostering trust and shared accountability.
One challenge we faced was balancing the need for thorough and inclusive decision-making with the practical constraints of the project timeline. While we recognized that these discussions were crucial for building trust and ensuring ethical standards, the lengthy process also precipitated frustration for some stakeholders who were eager to move forward. Additionally, there were times when conflicting views within the Advisory Committee required debate, which further extended the process. However, we set clear milestones and deadlines for each phase of the decision-making process, ensuring that discussions were productive and that the project maintained momentum. For example, when working on the TOR, we established specific timeframes for each round of revisions and feedback. We communicated these timelines clearly to all members of the Advisory Committee, while also ensuring flexibility for further input where needed. This approach allowed us to maintain forward progress without compromising the quality of the discussions. We also ensured that any concerns or suggestions raised during these periods were captured and addressed, but within the structured timelines we had set.
Strategy 4: Training Peer Researchers with Lived and Living Experiences
For those with living experiences who expressed interest in engaging more deeply in the research process, we developed and implemented a training program using a modified version of one of the co-investigator’s previous approach (EA) (Eaton et al., 2018). The training was grounded in capacity-building and aimed to empower these individuals by equipping them with the skills and confidence to engage meaningfully as active partners in the research. (Eaton et al., 2018) As the training was already developed, we were able to implement some of the teachings within 3 weeks of the TOR being finalized. However, we did not formally evaluate or obtain feedback on the training. The training focused on aspects such as interviewing and facilitation, including active listening, empathy, and the ability to challenge participants constructively. (Eaton et al., 2018) The curriculum also discussed data analysis. During the training, we acknowledged that traditional research hierarchies could create barriers to meaningful collaboration and mutual trust. Through this training, participants had opportunities to engage in multiple aspects of the research process. They co-led interviews, co-facilitated sessions, contributed to data analysis, and co-authored academic papers. Importantly, their feedback was given equal weight to that of academic researchers throughout the research process.
Strategy 5: Iterative Process
Throughout the research, we adopted an iterative process to refine our methods and ensure they were responsive to participants’ needs, preferences, and lived experiences. Central to this approach was offering participants diverse choices in how they engaged with the research. For example, participants could choose between interviews or focus groups, and they had the option to select their preferred method of communication, whether in person or virtually. Additionally, participants could choose to have their interview conducted by a Principal Investigator, a research assistant, or a peer researcher, allowing them to feel the level of comfort and familiarity that suited them best.
We began all group activities, including focus groups and co-design sessions, with comfort talks and the creation of Safe, Brave Space principals inclusive of Confidentiality, Respect, Collaborative Spirt, Shared Space, Positive Crosstalk and Self-Care (Arao & Clemens, 2023). These discussions allowed participants to express their needs, concerns, and preferences openly, ensuring that everyone felt heard and respected. A physician trained in trauma-informed care was available during these sessions, and we provided participants with access to trauma resources should they require support. Importantly, participation in these sessions was entirely voluntary—individuals could choose to partake as much or as little as they felt comfortable with, and their well-being remained at the forefront of our approach.
We facilitated the receipt of feedback on co-design sessions by consulting participants in advance about their preferences on practical aspects of participation. This included their thoughts on location, timing, honoraria, refreshments, and other logistical elements to ensure their comfort and engagement. Additionally, we asked participants about the number of follow-ups that should occur and whether they felt comfortable with certain members of the research team, such as physicians or other team members, being present during sessions. Insights gained from these consultations revealed specific logistical preferences that improved attendance, such as preferred meeting times being mid-afternoon and suitable honoraria involving a choice in participant gift cards (that are physical vs. electronic). Participants also expressed a desire for more inclusive spaces, where not all team members are present, which led us to adjust the composition of the research team present at sessions. Participants also gave opinion as to the food and refreshments they prefer, noting that they wanted salads as numerous events will offer unhealthy options.
Strategy 6: Co-Designing Model and Knowledge Sharing
We approached the co-design process with a clear focus on transparency and collaboration, ensuring that participants understood how their feedback and contributions directly shaped the research and the practical applications of the model being developed. After each co-design session, we provided participants with clear explanations of how their input was being used to inform and refine practices at the academic hospitals affiliated with this work. This transparent approach allowed participants to see the tangible impact of their contributions on both the research process and the implementation of findings.
Throughout these sessions, the model was iteratively refined with participant feedback, emphasizing the collaborative nature of the process. We shared findings back with participants in accessible, lay terms to ensure clarity and understanding, reinforcing their role as co-creators of this work. Additionally, we offered certificates of attendance to acknowledge their contributions and to underscore their ownership of the co-designed model.
To maintain ethical standards and respect for participants’ contributions, we sought explicit permission before any findings were published. This ensured that participants retained agency over their involvement and had the opportunity to review how their insights were represented in the research.
Key Considerations
Our co-design process focused on creating virtual HIV models of care that are socioculturally responsive (Kokorelias et al., 2023a). Our study aligns with similar work in health research that highlights the need for culturally and socially responsive care models (Tragantzopoulou & Giannouli, 2024).Trust was foundational to our approach. Over the course of a year, we embedded ourselves within the community by engaging authentically in spaces such as community centers, health clinics, shelters, and social events. Rather than imposing our research goals, we allowed relationships to build organically, fostering spaces where community members felt comfortable sharing their lived experiences. Transparent communication about research goals, funding limitations, and expectations further strengthened these relationships. We recognized that older adults living with HIV have diverse and intersecting identities, experiences, and health needs. To ensure inclusivity, we paid close attention to addressing varying physical, cognitive, and social abilities in our research. For example, we ensured that our recruitment and data collection processes were accessible to individuals with different physical abilities by offering multiple formats for participation, such as in-person interviews, telephone interviews, and virtual meetings. In terms of ethical oversight, we sought Research Ethics Board approval specifically for the research components of the project, such as data collection, reporting, and the approach to participants. This approval was necessary once we moved into the formal stage of designing the grant and began planning the systematic collection and analysis of data. However, the community engagement work, including the relationship-building and advisory committee involvement, did not require Research Ethics Board approval at that stage. These activities were considered part of the foundational work for the project, aimed at fostering trust and collaboration within the community. Instead, it was a process of consultation and partnership building, which laid the groundwork for the research but was not subject to the same ethical review.
While not explicitly considered by our approach, the influence of cognitive deficits also has implications for research methodologies. Older adults living with HIV are at risk of cognitive impairments and as such, researchers must be mindful of these challenges when designing studies that involve older adults with cognitive deficits (Tragantzopoulou & Giannouli, 2023). For instance, ensuring that interviews and focus groups are conducted in ways that allow for clarification, repeated questioning, and alternative methods of expression (e.g., visual aids or written summaries) could help mitigate these issues (Wright & Holliday, 2007). Additionally, in the HIV population, cognitive impairments are often coupled with mental health challenges, such as depression and anxiety, which further complicate the ability of individuals living with HIV to navigate both their healthcare and participation in research settings (Tragantzopoulou & Giannouli, 2023). These mental health issues, coupled with cognitive decline, can also affect the trust-building process in research and healthcare settings, where individuals with past experiences of stigma or discrimination may be less willing to engage fully. Incorporating these considerations into the co-design process was vital for ensuring the inclusivity and accessibility of the virtual care model. As such, we recommend that future co-design efforts actively consider the cognitive and mental health needs of older adults living with HIV as part of the core design principles.
Our research approach emphasized flexible, accessible communication methods and provided participants with choices about how they wished to engage—whether virtually, in-person, or using alternative communication modes—to align with their individual preferences and capacities. Throughout the research, we practiced reflexivity to critically examine our own roles, privileges, and biases as researchers. This process involved regular self-examination and open discussions within the research team to ensure that we remained aware of how our backgrounds, perspectives, and power dynamics might influence the design, implementation, and interpretation of the study. To facilitate this, we held regular meetings with our Advisory Committee where we discussed not only the progress of the research but also our personal reflections on the research process. These conversations allowed us to acknowledge and confront any biases that might have emerged, ensuring that we approached the work with humility and a commitment to inclusivity. We were mindful of how our positions impacted the research process and adapted our methods accordingly. This included using plain language in our interview questions, avoiding technical jargon, and being transparent about our goals in the research to ensure that the participants felt comfortable and that their voices were prioritized. By prioritizing reflexivity, flexibility, inclusion, and continuous dialogue, we sought to overcome barriers, build trust, and create models of care that are culturally and socioeconomically responsive to the needs of older adults living with HIV.
Throughout the research process, the trusting relationships we built within the community of older adults living with HIV in Toronto were crucial to our recruitment success. By engaging the community early and consistently over a year-long period, we not only strengthened our funding applications but also cultivated a network of committed individuals who were invested in the project’s success. This strong foundation helped ensure that recruitment efforts were met with enthusiasm and a willingness to participate, as community members felt both valued and heard. The relationships formed during the initial engagement phase made it easier to approach individuals for involvement in the study, leading to a diverse and committed advisory committee.
The involvement of the advisory committee had a profound impact on the design, data collection, and interpretation of the study. By embedding community voices at every stage—from the conception of the research questions to the analysis of the data—we were able to ensure that our findings were grounded in the lived experiences of older adults with HIV. This approach not only enriched the data but also provided unique insights that might have been missed if the committee had not been involved. Their contributions allowed for a deeper understanding of the nuances of aging with HIV, leading to interpretations that reflected the complexities and realities of the community we were studying.
This community-based approach has been highly valued by funders, as evidenced by the ongoing support for this work beyond the initial project. The engagement of the advisory committee and the community’s involvement in shaping the research has made it clear that this work is both relevant and impactful. Funders have recognized the value of this approach in ensuring that research is not only reflective of community needs but also directly contributes to meaningful change. The success of this work can be directly attributed to the advisory committee’s involvement, as their input has continued to inform subsequent projects and has helped sustain the relationships that will carry the work forward.
However, it is important to acknowledge that this process has not been formally evaluated. In hindsight, embedding evaluation activities throughout the project would have provided valuable insights into how the advisory committee was functioning and its impact on the research process. These activities could have included regular reflections or feedback sessions with the committee to assess how their contributions were influencing the study and whether there were areas for improvement in the collaboration. A formal evaluation could also have helped identify any challenges in the working dynamics or gaps in representation that may have emerged over time. Moving forward, this could be an important consideration for future projects to ensure that the committee remains engaged and that their involvement continues to be effective in shaping the direction and outcomes of the research.
We acknowledge that attitudes towards eHealth and virtual care and its adoption can vary significantly across different cultural contexts, influencing the experiences and care of older adults living with HIV. In many countries, healthcare professionals and laypeople alike may have varying levels of comfort and acceptance of virtual healthcare models, which can shape the effectiveness and accessibility of virtual models of care (Fors et al., 2009; Giannouli, 2023; Ribeiro, 2024). Research indicates that in some regions, trust in digital health platforms is low due to concerns about privacy, technological literacy, and cultural perceptions of healthcare (Adjekum et al., 2018). Understanding these diverse attitudes, beyond our study, is essential to developing inclusive, culturally responsive virtual care solutions for older adults living with HIV.
All in all, the practical insights gained from our early community engagement align with broader methodological debates in participatory research, particularly regarding the tension between researcher-driven and community-driven agendas (Montoya & Kent, 2011; Narendorf et al., 2023). As highlighted by other scholars, the challenge of balancing power dynamics and ensuring genuine community input in the research process is central to ethical co-design (Farr, 2018; Wallerstein et al., 2019). Our approach sought to respect community autonomy by incorporating their perspectives into the grant proposal and research protocol, thus moving beyond tokenistic involvement and addressing concerns about the power imbalances that often arise in such collaborations. This process not only reflects a commitment to inclusivity but also engages with ongoing discussions in the literature about the ethical and practical complexities of involving marginalized groups in research decision-making.
Conclusion
Through sustained community engagement, the development of a diverse Advisory Committee, ethical collaboration, and iterative research methodologies, we successfully created a research approach grounded in trust, flexibility, and shared decision-making. By prioritizing reflexivity, inclusivity, and respect for diverse identities and abilities, we ensured that the voices of older adults living with HIV informed every stage of this work. Our commitment to capacity-building, through peer researcher training and transparent, shared leadership, strengthened partnerships and empowered community members to actively participate in research. The iterative process allowed our methods to remain adaptable, responsive, and aligned with participants’ evolving needs. The lessons learned and strategies employed throughout this study provide a practical framework for researchers and practitioners aiming to overcome barriers in the development of equitable care models.
Footnotes
Acknowledgements
This methodology paper stems from the active collaboration and insights of key knowledge users involved in our research. We extend our heartfelt gratitude to the participants whose valuable contributions and perspectives have been instrumental in shaping this editorial.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the AGE-WELL Network of Centres of Excellent (NCE) (AW-CAT-2023-03) Inc and the Canadian Frailty Network’s (CFN) Catalyst Funding Program in Healthy Aging. The AGE-WELL NCE and CFN are funded by the Government of Canada through the Networks of Centres of Excellence program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors do not present any empirical data.