
Abstract
Keywords
Background
Among people in prison, the prevalence of homelessness is twenty times higher than the general population, resulting in housing insecurity upon release (Bashir et al., 2021). Consequently, housing interventions, like permanent supportive housing (PSH), are increasingly supplementing or even substituting for reentry interventions by focusing on reducing legal involvement among residents (Hunter & Mercier, 2023; Kriegel et al., 2016; LeBel, 2017). PSH is a housing intervention that provides permanent housing through an apartment or unit and case management, medical, mental health, and substance use services (Henwood et al., 2013). Like most reentry interventions for people with serious mental illnesses (SMI), PSH primarily focuses on meeting the clinical and service needs of people with SMI and substance use disorders with largely positive outcomes. There is substantial evidence indicating that PSH improves housing outcomes and reduces hospitalization and ER visits (Rog et al., 2014).
Although PSH independently provides resources that can be essential to the reentry process, they are not necessarily responsive to the unique needs of formerly incarcerated people with SMI (Fontaine, 2013; Hamlin & Purser, 2021; LeBel, 2017). Relative to formerly incarcerated people without SMI, people with SMI have longer incarcerations, higher recidivism rates, lower likelihood of getting and staying on community supervision as a condition of early release, and less time in the community (Cloyes et al., 2010; O’Keefe & Schnell, 2007; Prins, 2011; Skeem et al., 2011). They also have elevated rates of homelessness, medical problems, and substance use disorders (Baillargeon et al., 2010; Baranyi et al., 2022; Bashir et al., 2021; Bronson, 2017; Bronson & Berzofsky, 2017; Cuddeback et al., 2010; Roman & Travis, 2016). Reentry interventions provide a critical anchor in the absence of coordinated discharge planning, often beginning during an incarceration and continuing through the transition and integration of a formerly incarcerated person with SMI.
During reentry, housing interventions like PSH require additional strategies to function as standalone reentry programs aimed at reducing recidivism and improving mental health outcomes during reentry (Leclair et al., 2019). This is in part because PSH are often located in high-risk environments (e.g., high-crime, high-poverty neighborhoods) where its formerly incarcerated residents are more heavily surveilled and also surrounded by spaces they are often mandated to avoid (Tsai et al., 2011). In addition, despite provision of housing and mental health services, PSH does not address the community integration of its residents, a critical component of reentry (Motte-Kerr et al., 2020). Reentry programming is significant not only as a touchpoint for necessary resources and social services, but also in its potential provision of support to people who are re-engaging with their communities following extended incarcerations (Blank Wilson, 2013; Wilson et al., 2017). While PSH do not systematically address this type of community integration, community integration is an inevitable extension of housing. Housing is situated in a larger neighborhood environment with both risks and benefits, unavoidable to its residents, and also, potentially resourceful.
Extant research indicates that community context, like the environments surrounding PSH, influences intervention success (Barrenger & Draine, 2013; Barrenger et al., 2016). If interventions operate in risky environments (e.g., an area with higher crime), their impact may be diminished without supplemental intervention focused on the environment itself. Likewise, resource density plays a role in the types of services and linkages that can ultimately be made accessible to community members if an intervention is case management oriented and reliant on external treatment and service providers. For people with SMI, riskier, resource-poor environments can broadly impact access to treatment and opportunities for support and community participation.
Although PSH are typically situated in high-risk environments, they are also surrounded by public spaces that can be resourceful and supportive for formerly incarcerated people, people with SMI, and people who are homeless (Fields, 2011; Herbert & Beckett, 2010; Kriegel, 2019; Kriegel et al., 2019, 2023). Quality public space is associated with a sense of community and can contribute to improved physical and emotional wellbeing (Cattell et al., 2008; Francis et al., 2012; Gesler, 1992; Snethen et al., 2021). Formerly incarcerated people with SMI face cumulative stigma related to their SMIs and incarceration histories, prior institutionalizations, and policies preventing their full community participation and sustaining a sense of carceral citizenship (Miller & Stuart, 2017; Rowe & Baranoski, 2000). Given this, public space engagement and accessibility is particularly important for this population, though often hampered by restrictive and/or exclusion policies (Herbert & Beckett, 2010; Miller & Stuart, 2017; Mitchell, 1995; Stuart, 2016). Formerly incarcerated people with SMI, particularly those who are or have been homeless, rely on public spaces because they provide social interaction and a sense of belonging (Herbert & Beckett, 2010; Kriegel, 2019; Kriegel et al., 2023). They also use these spaces to build capital, find social support, and meet basic needs through access to computers, internet, outlets, and a safe space to spend the day (Desmond, 2012; Fields, 2011; Kriegel et al., 2023). In a recent study on the use of public space during reentry, formerly incarcerated participants with mental illnesses described seeking out strangers in public spaces, with whom they developed rapport and trust and participated in supportive interactions, with little expectation for reciprocity (Kriegel, 2019). Participants also used non-clinical public spaces for solitude, socialization, and resource acquisition (Kriegel et al., 2023). These spaces collectively demonstrate an opportunity for PSH to not simply address the housing and treatment needs of its residents, but to explore their unique community reentry needs of those residents who are formerly incarcerated and have SMIs.
Theoretical Framework
The risk environment framework provides a structure for understanding community reentry and has been used to inform the development of structural interventions addressing health disparities (Rhodes & Simic, 2005). Risk environments are the spaces where individual, interpersonal, and structural/environmental factors interact to increase the chance of a certain risks like drug use, HIV transmission, or reincarceration (Barrenger et al., 2017; Henwood et al., 2018; Rhodes & Simic, 2005). They have two dimensions (i.e., types and levels) and are shaped by two mechanisms of influence (i.e., susceptibility and vulnerability; see Figure 1). The different types include physical environments (e.g., public spaces, PSH), social environments (e.g., social networks), economic environments (e.g., cost of living), and policy/political environments (e.g., federal housing policies, municipal homelessness policy priorities). Each type of risk environment exists at the macro environmental level (i.e., broader structures and policies informing local practices) and the micro environmental level (i.e., personal decisions or community norms). As an example, a micro social environment might include everyday social interactions while a macro social environment would include both structural stigma and marginalization. While conceptualized through its elements, a risk environment is the totality of these various types, levels, and mechanisms of influence. Risk Environment Framework.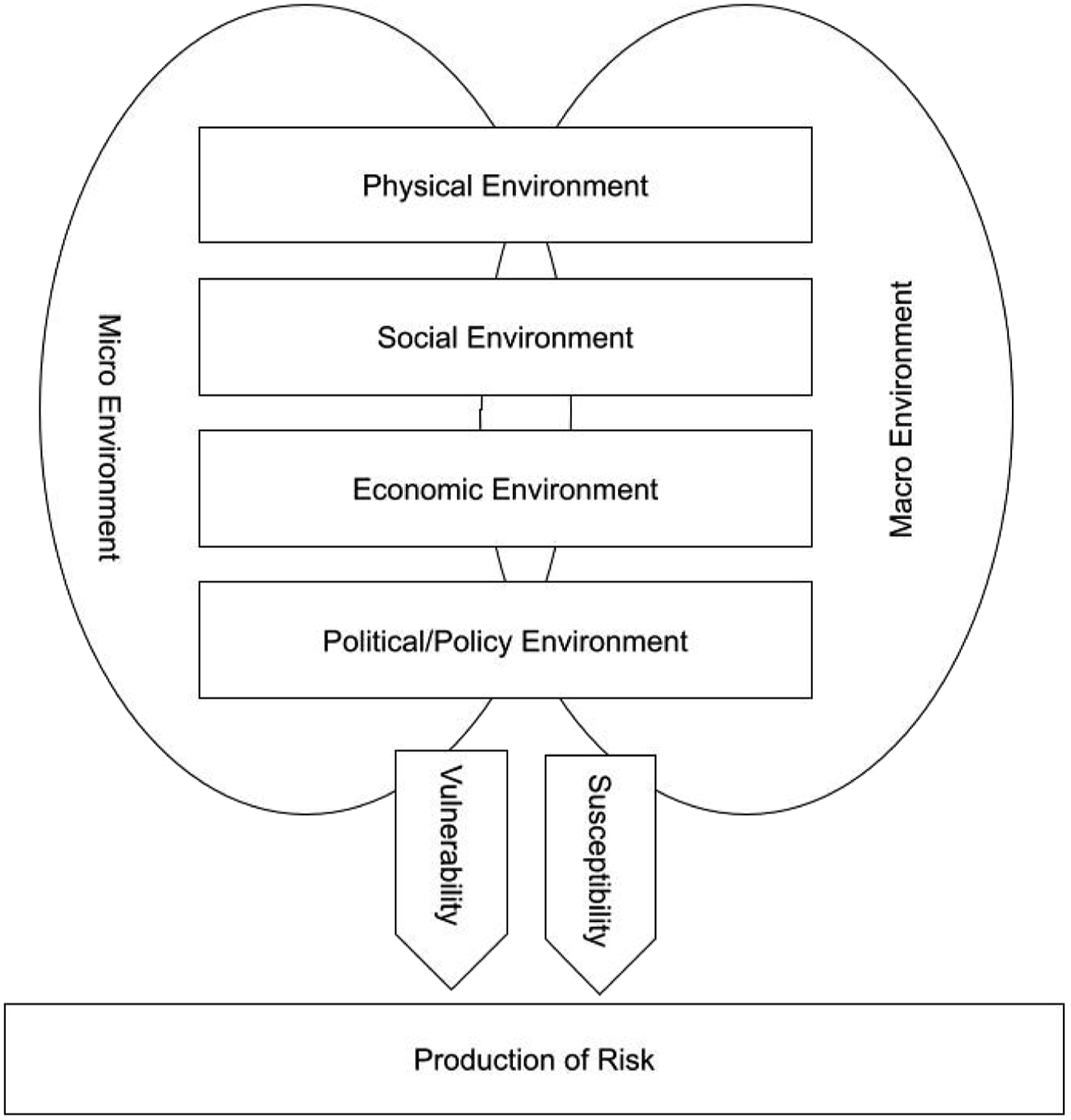
During reentry, production of risk in these environments is confounded by the presence of SMI and histories of homelessness, both of which inform susceptibility and vulnerability to different risks. Both populations are, for example, more susceptible to reincarceration and more vulnerable to the consequences of incarcerations (Herbert et al., 2015; Matejkowski & Ostermann, 2015; Rhodes, 2002). Risk environment analyses, conducted using ethnographic methodologies, have examined both reentry for people with SMI and PSH for adults engaged in high risk behaviors (Barrenger et al., 2017; Henwood et al., 2018). In both cases, risk environment analyses situated the role and impact of community context therefore creating opportunities for multilevel intervention targets that are both responsive to community context and optimize the perspectives of impacted community members through participatory methods (Agurs-Collins et al., 2019; Blankenship et al., 2006; Minkler & Wallerstein, 2011).
Risk environment factors interact in both private and public spaces to contribute to community participation, treatment engagement, psychiatric distress, and substance use, which we collectively define as reentry wellbeing in the present study (see Figure 2). PSH are both private and public spaces and are consequently well-situated as a platform for interventions focused on improving reentry wellbeing by targeting the interplay of individual, interpersonal and structural factors. Yet, the current approach to understanding risk environments through ethnographic methods alone limits the reach of these examinations because risk environments are both measurable and meaningful. Ethnographies study the subjectively meaningful relationship that people have to their spatial environments, but require prolonged engagement for often undetermined periods of time and resources (Atkinson et al., 2001; Small, 2009). Short term ethnographic methods, like go-along interviews, provide an alternative, but are neither participatory nor do they capitalize on geospatial analysis through GIS, and therefore benefit from complementary methods to enhance their findings. Triangulating data through participatory and spatial methods is thus critical to optimizing risk environment analyses to examine the broader geography of PSH, including both private and public spaces, and their measurable and meaningful impacts on reentry wellbeing through individual, interpersonal, and structural factors. With this information in hand, it is possible to develop more impactful reentry interventions and better facilitate reentry wellbeing. Reentry Wellbeing for People with SMI.
To date, public space and interactions within have not been investigated empirically to understand the reentry outcomes of formerly incarcerated people with SMI, including those in PSH. Extant research often relies on singular methods to examine reentry; however, reentry is both complex and dynamic and informed by both individual and structural processes. Given this research gap, this study incorporates GIS, participatory mapping, semi-structured interviews, and go-along interviews to apply a risk environment framework to PSH for people with SMI during reentry and support the development of a targeted intervention. In doing so, we hope to achieve a multi-angular understanding of what reentry looks like through measurable data (e.g., GIS data) and meaningful experiences captured through qualitative and participatory methods. In the final phase of the study, we will employ participatory methods, through use of a Generative Co-Design Framework, to co-design a multilevel intervention framework with both data collected and the lived experiences of participants and providers. Participatory methods, used during data collection through participatory mapping and in this final phase, are methods that prioritize community voice and action in the research process (Minkler & Wallerstein, 2011; Stringer, 1996). Through participatory methods, we leverage the contribution of people with lived experiences in the data we collect and analyze.
Methods
Study Design
The study uses a rigorous, novel QUAL + QUAN (spatial) concurrent mixed-methods design to examine how individual, interpersonal, and environmental factors situated in the PSH risk environments interact in public and private spaces to inform reentry wellbeing (see Figure 2; Palinkas, 2014). The study will use a convergent parallel design combining quantitative and qualitative data in equal measure to confirm/disconfirm respective findings (i.e., triangulation), enhance and elaborate findings of each method (i.e., complementarity), and to expand on independent findings to create nuance (i.e., expansion; Creswell & Clark, 2017).
Using the risk-environment framework, 80 multi-method interviews (i.e., qualitative, quantitative, and participatory mapping methods) that look at individual, interpersonal, and environmental factors will be conducted with formerly incarcerated participants with SMI (40 people per site). To increase rigor, data collected through these interviews will be triangulated with go-along interviews with up to 20 participants (10 per site; Padgett, 2011). Participatory mapping will be geocoded and sites identified as places of importance, frequent participation, and belonging will be evaluated in relation to features of spaces like resource and treatment availability using GIS to develop a community resilience index. The findings will be presented to a community advisory board (CAB) of two providers and six formerly incarcerated PSH residents with SMI as part of a Generative Co-Design process (Bird et al., 2021; McKercher, 2020).
Recruitment and Eligibility
Eligibility criteria for the study requires participants (1) be an adult (≥18 year of age) residents in PSH in either Los Angeles, California or Spokane, Washington; (2) have a self-reported SMI diagnosis (schizophrenia, major depressive disorder, or bipolar disorder); (3) be released from jail or prison in the recent 5 years following a ≥6 month sentence; (4) be able to speak and understand English. Purposive sampling of formerly incarcerated people with SMI living in PSH will be used through flyers posted in PSH sites as well as word of mouth through program providers. Jail and prison incarcerations are included to ensure inclusion of people serving shorter sentences (less than 1 year) in jails rather than prisons. Those who express interest are screened through a brief 5-question screening tool and eligible participants provide consent to participate. Participants are compensated $40 for the initial multi-method interview and $40 for each subsequent go-along interview.
Study Sites
Data is being collected in Los Angeles, California (n = 40) and Spokane, Washington (n = 40). There are currently over 22,000 PSH units in Los Angeles and 500 in Spokane (Los Angeles Homeless Services Authority, 2024; U.S. Department of Housing and Urban Development, 2023). Access to PSH is based on measures of vulnerability that prioritize people with mental illnesses and consequently, PSH primarily serves people with SMI (Gilmer et al., 2015). Los Angeles and Spokane were selected as a method of critical case sampling, which aims to show variations that emerge through very different samples (Patton, 1990). Los Angeles is a highly urban setting with both racial/ethnic and socioeconomic diversity and is facing a significant housing crisis. Spokane is a mid-sized city that has seen a 46% increase in homelessness in the past 10 years (Spokane City/County Continuum of Care, 2020). It is tucked amid rural counties and American Indian Reservations and has a more racially and ethnically homogenous population. Sample variation derived from the differences between Spokane and Los Angeles will help to resolve feasibility concerns in support of future development and evaluation of an intervention across diverse urban and rural environments.
Measures and Materials
The study is undergirded by the Risk Environment Framework and its analytic axis examines how individual, interpersonal, and environmental characteristics interact in private and public spaces to facilitate reentry wellbeing. To evaluate these characteristics, the measures described below will be used as part of a baseline semi-structured interview. Data collection methods are informed by the ethnographic shadowing template developed by for a prior risk environment analysis of PSH (Henwood et al., 2018). We will examine reentry wellbeing through (1) community participation; (2) treatment engagement; (3) psychiatric distress; and (4) substance use.
Measures of Individual Characteristics
We will use a brief sociodemographic survey, modeled after surveys used in similar studies to identify sociodemographic characteristics. Questions on the survey will cover age, sex, gender, sexual orientation, race and ethnicity, education, homelessness history, mental health history, substance use history, criminal legal history.
Measures of Interpersonal Characteristics
Interpersonal characteristics are defined through social support (i.e., participants’ perceptions of the functions performed by members of their social networks) and social capital (the quality and quantity of resources in participants’ networks; Lin, 2002; Valente, 2010). Social support will be measured using the Medical Outcomes Study (MOS) Social Support Survey, which assesses social support through a 19-item questionnaire (Sherbourne & Stewart, 1991). The survey is divided into four subscales: emotional/information, tangible, affectionate, and positive social interaction. Participants indicate how often each type of support is available to them using a 5-point rating scale (e.g., 1 = none of the time and 5 = all of the time). Social Capital will be measured using the Resource Generator-United States (US), which assesses social capital through a 26-item scale (Foster & Maas, 2016). The survey has three subscales on expert access, problem solving, and personal support. Participants are asked whether they know someone who can provide different listed resources and to then specify relation. The measure captures the human, cultural, financial, political, and physical capital domains of social capital. The Resource Generator-US is adapted from prior scales used in the Netherlands, UK, and Canada for a US audience.
Measures of Environmental Characteristics
Environmental characteristics are defined through community integration (i.e., physical, social, and psychological integration into any defined community), public space engagement (i.e., the use of public spaces to access resources and interpersonal connections), and housing environment. Public space engagement is also defined subjectively through participants’ appraisals of importance, sense of belonging, frequency of contact in each space and objectively using GIS to examine resource and treatment availability/accessibility. To measure public space engagement, geocoded variables derived from participatory mapping data (described in further detail below) will be categorized into three areas: number of places of belonging, number of places of importance, and number of areas of frequent contact. This method of geocoding participatory mapping variables is adapted from Townley and colleagues who used a similar method to understand how homeless youth experience sense of community in their activity spaces (Townley et al., 2016). Community integration will be measured using the 10-item Community Integration Measure (McColl et al., 2001; Townley et al., 2013). The scale looks at feelings of acceptance and opportunities for community participation using a 5-point rating scale (i.e., “always disagree to “always agree”). Housing environment will be measured through the Housing Environment Survey, which assesses the housing environment using a social ecological approach through seven scales and three inventories, including two physical environment scales (i.e., dwelling physical quality and neighborhood physical quality); two social environment scales (i.e., neighborhood safety and neighborhood social climate); three interpersonal relationship scales (i.e., neighbors, roommates, and landlords); and three inventories on housing demographics, housing costs, and residential satisfaction (Kloos & Shah, 2009).
Measures for Reentry Wellbeing Outcomes
For this study, reentry wellbeing is defined through measures of community participation, treatment engagement, psychiatric distress, and substance use. Community participation will be measured using the 31-item Temple University Community Participation (TUCP) Scale (Salzer et al., 2014, 2015). The TUCP asks participants to indicate number of days in the prior 30 they participated in 27 different areas (e.g., going a restaurant or coffee shop), whether they perceive their participation in that area to be important, whether they have participated in that area as much as they desire. Treatment engagement will be measured using the Continuity of Care Measure (CONNECT), which focuses on continuity of care, a critical element of treatment access and provision of people transitioning between systems (e.g., criminal legal, mental health, and housing systems; Ware et al., 2003). The 72-item survey uses a 5-point rating scales to assess a person’s perception of their service providers’ knowledge and availability to client; flexibility; attention to primary care; movement from inpatient to outpatient care; changes in provider; and changes in housing. Psychiatric distress will be measured through the Modified Colorado Symptom Index (MCSI), a 14-item self-report scale that assesses frequency of psychiatric symptoms (Conrad et al., 2001). Responses are rated using a 5-point rating scale (0-not at all to 5-at least every day). Substance use will be assessed using two measures. The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item self-report scale that assesses severity of alcohol use within the recent year, with a total score range of 0 to 40 (Saunders et al., 1993). The Drug Abuse Screening Test-10 (DAST-10) is a brief 10-item scale that assess drug use in the recent year (Skinner, 1982).
Semi-Structured Interview
Semi-structured interviews will focus on attributes of the physical, social, economic, and political environments detailed by the framework and the individual, interpersonal, and environmental/structural factors. Prompts will ask participants to (1) narrate their reentry experiences; (2) describe where they live, including neighborhood and in-house services and security; (3) describe supports and challenges experienced following release as well as since moving into PSH; and (4) describe where they spend time and the people with whom they spend time. Probes will focus on where participants feel most at ease, most welcomed, and most unwelcomed as well as the people with whom people feel at ease, spend time, and provide and receive different types of support. Broad qualitative prompts permit participant-led descriptions of a problem and interviewer probes ensure the expanse of a question is addressed (Creswell & Poth, 2016).
Participatory Mapping Protocol
Participatory mapping will be used to examine place-based interactions and participant-driven descriptions of community spaces and icons (Parker, 2006). Participatory mapping incorporates elements of inclusion, transparency, and empowerment and has been used in previous research with people with SMI (Townley et al., 2009). Participants will be asked to identify (1) spaces they frequent; (2) spaces they feel are important; and (3) spaces of inclusion and exclusion. To understand the social context of these spaces, participants will be prompted to list any interactions that typically take place in the spaces mapped.
Go-Along Interviews
Up to 10 go-along interviews will be conducted at each site (n = 20 participants). The final number of participants will be determined by saturation of data (i.e., congruence between interview data and go-along data). Go-along interviews combine qualitative interviews with ethnographic observations to understand participants’ experiences and practices as they interact with social and physical environments. During these interviews, interviewers accompany individuals on their natural outings. They are usually 90 min long, but participants ultimately determine length of time that makes sense for the outing (Kusenbach, 2003). The interviewer might follow up on specific interactions and spaces mentioned during the prior interview. Following each interview, the interviewer will record field notes using a field note template, developed by Henwood and colleagues (Henwood et al., 2018).
Spatial Data
Spatial data will include public and participatory mapping data. Public data will be gathered from federal and local government agency websites, including Census.gov, the County of Los Angeles Enterprise Geographic Information Systems, the California state geoportal, City of Spokane Open GIS data, and the Washington Geospatial Open Database. Mortality and crime data will be purchased through state agencies. Collectively, these public servers have data on mental health and substance use programs and centers and other public services, including police stations, courthouses, and libraries. Using methods employed by Townley and colleagues, we will geocode participatory maps, which involves the conversion of addresses to longitude and latitude coordinates (Townley et al., 2016). Addresses will be identified using Google maps through information provided by participants. If participants identify private spaces outside PSH sites (e.g., someone’s home), we will ask participants to identify the closest major intersection to ensure privacy is protected. Participatory mapping data will be parsed into variables based on interview data, including: (1) spaces of belonging; (2) spaces of importance; and (3) frequently accessed spaces.
Analytic Approach
Qualitative Analysis
A risk environment analysis will be conducted through qualitative analyses in two phases. The first phase will include inductive grounded theory methods (e.g., open, axial, and selective coding; Glaser & Strauss, 1967; Strauss & Corbin, 1994). Constant comparative analysis through memo writing will be used as part of the coding process to systematically identify similarities and differences across all interview sources, including semi-structured interviews, participatory maps, and go-along interviews, and to organize and synthesize the large amount of data collected (Glaser & Strauss, 1967; Strauss & Corbin, 1994). Initially, two members of the research team will independently code an initial transcript and then compare results to reach consensus on the codebook. They will then independently code four transcripts using developed codebook and compare code assignments by passage or quote. Discrepancies will be resolved through consensus, and themes will be developed from coded material. The second phase of coding will focus on the different types of environments and influences detailed through the risk environment framework using a template analytic approach (Crabtree & Miller, 1992). Template analysis is particularly useful when using an existing conceptual framework because it allows for the use of a priori codes (e.g., macro environment and micro environment, physical, social, economic, and policy environments, susceptibility factors, vulnerability factors, public spaces, and private spaces). The triangulation of interview data, participatory mapping data, and go-along interview data provides an added strategy of rigor to identify weaknesses and strengths in using our proposed measure of risk environments. ATLAS.ti qualitative software will be used to code transcribed data (ATLAS.Ti Scientific Software Development GmbH, 2020).
Quantitative Analysis
We will summarize baseline characteristics, including age, sex, gender, sexual orientation, race and ethnicity, education, homelessness history, mental health history, substance use history and criminal legal history. Quantitative data collected reflects the risk environment framework and seeks to evaluate relationships demonstrated in Figure 2. We will conduct simple linear regression to determine the association between each interpersonal and environmental measure and study outcome. As the data allows, we will investigate multivariable regression models that include all independent variables to assess the independent effect of each variable on each outcome. All modeling will be performed in SPSS (IBM, 2020) or R statistical software (R Core Team, 2020), as applicable. Both qualitative and quantitative analyses will consider the impact of gender and racial/ethnic identities on the experience of study outcomes given women and BIPOC communities navigate risk environments differently because of social and structural inequalities (Nkansah-Amankra et al., 2013; Spjeldnes & Goodkind, 2009). Quantitative and qualitative findings will be integrated and merged during this analytic phase of the study in order to provide a conceptual framework to inform intervention development (Fetters et al., 2013).
Community Resilience Index Development
Spatial data collected from participants will be geocoded and then analyzed in two ways. First, we will use data collected to develop a community resilience index model. Second, we will conduct a cluster analysis. Conventionally, we use vulnerability indices to characterize and quantify susceptibility to illness or public health hazard (Amram et al., 2020). For this study, we aim to develop a model for an index that can characterize and quantify opportunities for community engagement for formerly incarcerated people with SMI who live in high-risk environments, like PSH. These opportunities can support public space engagement and community integration, which, we hypothesize, help to facilitate reentry wellbeing. Because of the novelty of our index and the limited evidence supporting the integration of objective and subjective measures of space, we aim to develop a model for an index first. Once refined, a community resilience index can identify physical and social spaces of risk reduction and production to support a risk environment analysis. Because we are collecting this data in two predominately urban areas, we will focus on density through availability of these spaces (i.e., how many of these types of spaces exist within a 3-mile buffer around the PSH sites). To develop a model for a community resilience index, we will use unadjusted and adjusted multilevel modeling to examine individual, interpersonal, and environmental indicators as well as density of parks, libraries, coffee shops and restaurants, entertainment centers (e.g., movie theaters), retail spaces, food banks/soup kitchens, and treatment providers (e.g., community mental health centers, substance use treatment programs) and their association with spaces of belonging, importance, and frequency of use (as reported by participants during interviews). To further determine how the relationship between these indicators and the three outcomes generalize to unseen data through a community resilience index, we will utilize leave-one-out cross validation to evaluate fitted models via R^2 and root mean square error (RMSE). A cluster (i.e., hotspot) analysis will subsequently be conducted using the Getis G function in ESRI ArcGIS to identify geographic clusters of two evidenced risk factors affecting formerly incarcerated people with SMI: (1) areas of arrest, clustered by crime and (2) drug overdose, clustered by drug type (Jacobs & Skeem, 2021). The Getis G statistic is used to quantify and assess links between spatially distributed variables (Getis & Ord, 2010). This analysis will allow the research team to identify and map ‘hot’ and ‘cold’ spots of arrests and drug overdoses. To support the risk environment analysis, we will then do an overlay with the community resilience index model to examine the relationship between community resilience (i.e., belonging, frequency of use, and importance in relation to treatment and resource access and provision) and significant characteristics of the risk environment. All geocoding and GIS analyses will be conducted using ArcGIS Pro (Esri, 2020).
Mixed Method Integration
Qualitative, quantitative, and spatial data will be merged after independent analyses are completed for the purpose of convergence, complementarity, and expansion (Creswell & Clark, 2017). First, through convergence, we can confirm or disconfirm findings by triangulating each form of data. Secondarily, we will use qualitative data to provide nuance and depth to quantitative and spatial data. Quantitative and spatial data help to establish relationships between variables, but unless we open the black box with qualitative data, we cannot know the mechanisms by which they work. Finally, we will use qualitative, quantitative, and spatial data to expand on individual findings. This final step allows us to create a more comprehensive and inductive understanding of a complicated theory like the Risk Environment framework. Community-based research is often messy and individual data methods provide limited insight into complex problems. Through mixed methods, we aim to create a nuanced portrait that help in the co-design of a multilevel reentry intervention that supports formerly incarcerated people with SMI living in PSH.
Ethics
In consideration of ethical standards, informed consent will be obtained in writing from all potential participants prior to participation. Potential participants will be told about the study’s purpose and all procedures involved. Study staff will administer the University of California, San Diego Brief Assessment for Capacity to Consent (UBACC), a brief screener of capacity to consent to research procedures designed for adults with psychiatric illness (Jeste et al., 2007). Those who cannot demonstrate capacity to provide informed consent on this screener will be administered the MacArthur Competency Assessment Tool for Clinical Research (MacCAT-CR), a comprehensive, gold standard tool for assessing capacity to provide informed consent for adults with SMI (Appelbaum & Grisso, 2001). Only people with a demonstrated capacity to provide informed consent on these measures will be enrolled in the study.
Direct identifiers will be removed from qualitative data, and identifiers maintained for the purpose of follow-up with go-along interview participants (e.g., email addresses, phone number, name) will be stored in a password-protected document on a password-protected computer separate from participant data. Only study staff will have access to survey data, participatory maps, audio recordings, and transcripts. During audio-recorded interviews, we will instruct the interviewee not to mention their name or anyone else’s name. In the case that someone’s name is mentioned, identifiers will be removed or altered in transcription. Completed data forms will be placed in locked file cabinets at every site, and only authorized staff members will have access to the data. All study personnel will participate in extensive training in consenting procedures and will be required to complete Institutional Review Board, HIPAA, and compliance training.
Rigor
To achieve trustworthiness (including credibility, transferability, and confirmability) as well as evidentiary adequacy, we will incorporate multiple strategies of rigor (Erickson, 1986; Lincoln & Guba, 1985). The research team will document context notes following interviews as well as site notes to detail any observations of PSH sites both during recruitment and data collection (i.e., audit trail). Context notes are qualitative and ask interviewers to (1) describe participants’ overall wellbeing during the interview, including whether they are socially engaged or withdrawn, their level of functioning, and any evidence of mental health symptoms; (2) describe the location and place of the interview, including physical descriptions (e.g., layout, people who occupied the space during the interview, location condition, meaningful interactions at the location, and any background on the importance of the location to the participant, if relevant; and (3) describe any notable moments during the interview, including any interactions the participant had with other people, the nature of the relationship, or apparent reactions of others to the researcher. In addition, we have embedded member checking, peer debriefing and support, data and methodological triangulation, as well as prolonged engagement at various phases of the study. Phase 3 includes a CBPR-informed intervention co-design process with people with lived experience as well as providers during which findings from qualitative interviews and any initial analyses are reviewed and considered for future intervention development (i.e., member checking). The use of go-along interviews allows for both prolonged engagement across twenty participants to reduce risk of reactivity or respondent bias. Prolonged engagement can also increase risk of researcher bias, which we hope to offset through triangulation of data (i.e., qualitative data, participatory mapping data, and field notes), which can improve reactivity, respondent bias, as well as researcher bias. The research team will finally meet at regular intervals to discuss both data collection methods and emergent findings (i.e., peer debriefing and support).
Conclusion
Public space and interactions within have not been investigated empirically to understand the reentry outcomes of formerly incarcerated people with SMI, particularly those in PSH. This study uniquely employs multiple methods including GIS, participatory mapping, semi-structured interviews, and go-along interviews, to apply a risk environment framework to PSH for people with SMI during reentry. In doing so, we can co-design a targeted intervention that considers the relationship between public and private spaces and the individual, interpersonal, and environmental factors in risk environments that support reentry wellbeing. The findings from this study are well-positioned to consider the variability of risk environments—through geography and embedded features including rurality—and its impact on reentry wellbeing. Doing so will also resolve feasibility concerns in support of larger studies oriented toward intervention development, implementation, and evaluation as well as replication of this study in a larger sample across urban and rural contexts.
Footnotes
Ethics Approval
The Risk Environments of Permanent Supportive Housing for Formerly Incarcerated People with Serious Mental Illnesses study was approved by Washington State University IRB (#19786).
Informed Consent
Informed consent to participate will be obtained from all participants.
Authors Contributions
LK is the principal investigator of the study. The remaining authors are co-investigators and reviewed the manuscript. The authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study was funded by an award from the National Institute of Mental Health (NIMH) (K01MH129482, PI: Kriegel). The funding agencies had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized data from the study will be available from the authors after the study has ended.