
Abstract
Equity in healthcare is the ideal state where everyone shares equal rights and opportunities. To date, research methodologies are limited in their scope to translate into more equitable healthcare policies and practices. We present a re-interpreted grounded theory methodology to contribute to active dialogue toward optimizing equity through research. This re-interpreted research methodology is presented within a study investigating why ethnic disparities in infant survival from critical congenital heart disease occur in a multi-ethnic national setting in New Zealand. Using dialectical pluralism, we developed an innovative Multi-ethnic, Multisource Grounded Theory methodological concept by deliberately integrating Indigenous and multi-ethnic intersectional perspectives on health inequities from diverse data sources (literature reviews, retrospective case studies, and interview transcripts). Central to the process was the uplifting and centralizing of Indigenous voices. Conceptually, Multi-ethnic, Multisource Grounded Theory could reframe an existing research domain to equip researchers with a framework to intentionally integrate cultural considerations when building information from diverse data in the health equity space. Theoretically, this approach could enhance methodological rigour and support the translation of responsible, ethical, and equitable healthcare models.
Introduction
Generating knowledge about the intricacies and human realities of health inequity by race or ethnicity through safe and suitable research is critical to inform appropriate solutions (Bonham et al., 2018; Lu et al., 2022; Pfeffer, 1998). To that point, it is necessary to appreciate the complexity ingrained within the cumulative and compounding variables that interconnect when discussing inequities. Accepting the intersectional nature of the terms race, ethnicity, and culture is fundamental for investigators. Ethnicity describes a biologically based population group of common ancestry, culture, and language (Flanagin et al., 2021). In contrast, race depicts a socially organized construction of population groups with common phenotypical features within a social hierarchy (Lu et al., 2022). Finally, culture is a group of individuals with a shared understanding or common perspective that is dynamic in nature (Napier, 2015; Pfeffer, 1998). Although ethnicity, race, and culture all have unique descriptors, there is much overlap in how these words are applied in practice.
Exploring the area of health equity by ethnicity is innately challenging and can be nuanced with delicate content. We contend that traditional methodological approaches underplay the multidimensional and dynamic social processes overlying the determinants of inequitable health outcomes by ethnicity and race, with grounded theory (GT) offering the space and data emphasis to translate truth into tangible and culturally appropriate research knowledge (Glaser et al., 1967). Initially described in 1967 by Glaser and Strauss, GT is a systematic research process in which a theory is developed or deduced from concepts identified in the data through an iterative process of data collection and analysis (Glaser et al., 1967). Therefore, there is breadth in GT to incorporate multiple ethnic groups’ worldviews and flexibility in the iterative nature to ensure Indigenous ways of knowledge can be upheld respectfully in addition to traditional Western knowledge creation in research. Indigenous refers to the native inhabitants of a land or place.
Indeed, we have a responsibility to respect all ethnicities and their respective cultural views and values, with the inclusion of ethnic-specific practices having the potential to enhance and enrich research, particularly since The United Nations Declaration on the Rights of Indigenous Peoples depicts “Indigenous peoples have the right to maintain, control, protect and develop their cultural heritage, traditional knowledge and traditional cultural expressions, as well as the manifestations of their sciences, technologies and cultures” (Assembly, 2007).
We posit that a methodological shift is required to construct culturally appropriate knowledge in the multifaceted area of health inequity by ethnicity. We illustrate the principles of multi-ethnic, multisource GT, a methodological framework respecting Indigenous and Western knowledge creation in the presented study set in New Zealand (NZ). The NZ context is unique, with ongoing implications of Te Tiriti Waitangi (The Treaty of Waitangi, the founding document of Māori Indigenous partnership with the Crown), which are expected to be upheld, extending into research including Indigenous Māori. In addition, NZ is a country of immigrants, with many peoples Indigenous to Oceania (Pacific peoples) also residing in NZ.
Since NZ represents many cultures and peoples, an intersectional, culturally sensitive methodological research lens is necessary to acknowledge the diversity of the population in NZ and ensure safe research practices for this diversity. For instance, a large population in NZ has ancestral ties to the Pacific (8%) and to Asia (15%) (Bedford et al., 2019). Consequently, we strive to produce knowledge that respects Indigenous knowledge creation by interweaving a Kaupapa Māori and Pacific research methodology, Talanoa (Cammock et al., 2021; Nepe, 1991; Vaioleti, 2016) with Western methods.
There is no agreed definition of Kaupapa Māori research; however, several principles are generally applied, including acknowledging and respecting Māori culture, control, identity, relationship and potential (R. M. Brown, 2018; Rangimarie, 2008; Smith, 1997). Similarly, Talanoa has a broad uptake in pan-Pacific research, and although it originates from one island origin, the focus is on conducting research within respectful relationships and conversation whilst acknowledging the influence of community, heritage, and holistic wellness when conducting and applying research with multiple Pacific population groups (Cammock et al., 2021; Vaioleti, 2006, 2016).
The presented study also draws inferences from varied data sources. Theoretically, the use of complementary data from differential origins enhances the robustness of conclusions drawn from GT research (Glaser et al., 1967). Accordingly, literature review results, retrospective critical congenital heart disease (CCHD) case data and interview data from parents and health professionals were integrated to produce an extant explanatory GT to explain disparities in CCHD outcomes by ethnic group in NZ (Cloete et al., 2019).
The benefit of GT in utilizing multi-sourced information is that the methodology accommodates all data types (Glaser et al., 1967). Moreover, expounding a theory through the systematic GT approach offers the resilience to adapt and explore cultural inferences, assumptions, and other invisible human factors in a contemporary way to provide nuanced original theories beyond data descriptions (Birks et al., 2019; Birks & Mills, 2015; Creamer, 2021; Vogl, 2023). As such, the GT approach can be successfully re-interpreted and reconstructed to explicitly meet the innate needs of any research question, particularly those that probe into why or how phenomena occur through dynamic methodologies and philosophical paradigms (Birks & Mills, 2015; Charmaz, 2000, 2014, 2017; Corbin & Strauss, 2010; Cullen & Brennan, 2021; Glaser et al., 1967; Olmos-Vega et al., 2022).
Knowledge Creation
Scholars offer multiple philosophical paradigms and viewpoints about how knowledge is created, collected, and understood through research (Alharahsheh & Pius, 2020; Levers, 2013; Mertens, 2007; Morgan, 2014; Yong et al., 2021). A research paradigm contains four components - ontology, epistemology, methodology and methods (Alharahsheh & Pius, 2020). Epistemological and ontological positioning are components of an individual or collective cultural worldview, describing what is true or real and how knowledge is constructed to inquire about these truths (Rousseau & Billingham, 2018).
Therefore, a researcher’s overarching worldview supports and deepens a chosen inquiry framework and methodology to guide and inform the method employed to answer a specific research question (Charmaz, 2017; Scotland, 2012). Notably, dominant Western-centric ideology may overshadow cultural considerations when conducting studies, particularly when including Indigenous and minoritized ethnic groups, devolved of power, which was one driver of the development of approaches such as Kaupapa Māori. Consequently, cultural implications must be considered when ‘outsider’ researchers include diverse communities in their inquiries of which they are not ‘inside’ or a part of (Holmes, 2020). In addition, prevailing culturalist presumptions within Western-centric research practices historically have disempowered minoritized peoples, with recent advances focused on decolonizing research to include and describe minoritized and Indigenous peoples’ experiences fairly (Vaughn & Jacquez, 2020).
To successfully decolonize research design and conduct it in NZ, it is necessary for studies to accommodate a range of intersubjective realities and worldviews (Goodyear-Smith & Ofanoa, 2022; Harris et al., 2012). To this end, integrating the principles of more than two culturally relevant methodologies in a study to provide a fuller holistic view of phenomena within the tenets of GT is yet to be clearly outlined and will be explored (Enari, 2021; Wilson et al., 2022).
Paradigm Framework
The unique ability of GT to be flexible and compatible with multiple paradigms was a strength when considering the philosophy underpinning the research presented (Charmaz, 2000, 2017; Charmaz & Thornberg, 2021). Thus, dialectical pluralism was the overlying paradigm chosen with an exploratory and confirmatory philosophical approach (Johnson, 2017). Dialectical pluralism 2.0 was described in 2017 by Johnson (Johnson, 2017) and refers to the understanding and acceptance of disparate realities experienced by differential populations that thrive in the respectful tensions and dialogues produced (Johnson, 2017). Further, dialectical pluralism allows for synergies between different research methodologies and is defined as working within a meta-paradigm or a paradigm that can include and accommodate multiple perspectives or worldviews within one research philosophy (ontological pluralism and diverse epistemological outlooks) (Johnson, 2017).
Additionally, dialectical pluralism values multidimensionality and produces new holistic knowledge that is thoughtfully constructed and has room to leverage paradox and dissonance according to multiple disciplines (Johnson, 2017). The overarching paradigm applied to the illustrative study is visually represented in Figure 1, and the specific components underlying this are discussed in the next section. Multi-Ethnic, Multisource Grounded Theory Research Framework.
Methodological Approach
Kaupapa and Talanoa Principles and Their Application in This Research.

Table adapted from (Brown, 2018; Cram & Adcock, 2024).
aSamoan equivalent.
Appropriate ethical approvals were in place prior to gathering human participant data. Ethics approval was granted by the NZ Health and Disability Ethics Committee on 04/07/2021 (reference number: 21/CEN/128), and additional locality approval was obtained from each of the five hospital sites involved.
Methodologically, multi-ethnic, multisource GT embeds Kaupapa Māori and Talanoa Pacific research lenses purposefully into data collection methods and analysis to construct culturally pertinent theory (Cammock et al., 2021; Goodyear-Smith & Ofanoa, 2022; Martel et al., 2022; Smith, 1997; Vaioleti, 2016). The described research approach was essential to generate and integrate geographically located knowledge that was culturally applicable to Pacific and Maori populations through partnership and respectful dialogue. Consequently, the narratives of Pacific and Maori participants, their ways of being, and their epistemological positions were highly valued and culturally contextualized during the analysis. Moreover, in the presented study context of prior colonization of Indigenous Māori, the notions of equity, racism, power, and privilege are critically acknowledged and addressed throughout the GT development process to reflect these elements (Berman & Paradies, 2010; Harris et al., 2012).
Kaupapa Māori
Kaupapa Māori has been defined as “having a collective vision [which] binds people to one another for the achievement of [Māori] cultural wellbeing and prosperity (Cram & Adcock, 2022, p. 64). In NZ, Kaupapa Māori was designed to include a Māori worldview within transformative research practices to mitigate disparities (Jackson et al., 2015; Martel et al., 2022; Mahuika, 2008; Smith, 1997). The foundational principles of Kaupapa Māori research include valuing and incorporating Māori language, knowledge, customs, and characteristics (Smith, 1997). In 1991, Nepe described Kaupapa Māori as a “body of knowledge accumulated by the experiences through history, of the Māori people” with each component conceptualizing the ways of Māori knowing and being (Nepe, 1991, p. 4). Moreover, Kaupapa Māori creates space for descriptions of how Māori view and interact with ‘their’ world, applying validity and dignity to redress previous Western ways of victim blaming and shaming (Wilson et al., 2022). In essence, as Wilson describes, “Contemporary Kaupapa Māori research involves engagement with mātauranga Māori [Māori knowledge and ways of knowing] while simultaneously deconstructing and challenging Euro-Western epistemologies that construct and position Māori in negative or harmful and unhelpful ways” (Wilson et al., 2022, p. 383).
Talanoa
Talanoa as a methodology is a unique and culturally specific Pacific approach to research (Vaioleti, 2006, 2016). Talanoa has been ingrained in the Pacific way of living for centuries, with Pacific people valuing reciprocity, respect, and open dialogue (Vaioleti, 2006). Compared to Western methodologies, Talanoa focuses on oral knowledge production and the sharing of information through conversation, usually face-to-face (Vaioleti, 2006). Talanoa is centered around conversations between storytellers and a listener, where a relationship is built on respect for the cultural, spiritual, and emotional complexities shared in stories, as Pacific lived realities include relationships with their ancestors and spiritual world (Enari, 2021; Vaioleti, 2006, 2016).
Where Western research methodologies position those being researched outside of data collection and analysis, Talanoa intentionally includes those being researched as an active part of the process and removes the wall between the researcher and participant (Vaioleti, 2006, 2016). Although Talanoa is generally considered pan-Pacific, the Pacific region is heterogeneous in position, population, and culture across island contexts; for example, cross-cultural diversity exists between each island (Samoa, Tonga, Fiji etc.). Pictured metaphorically, Talanoa uplifts and includes Pacific voices: “Why hound me with a question when you don’t care for an answer, why play for a pair when there is only one dancer” - (Vaioleti, 2006, p. 21).
Grounded Theory
This multi-ethnic, multisource GT methodology adhered to the tenets of GT by keeping in step with the four core principles of GT as described by Timonen with explanations below of how this study specifically applied these principles in the research (Timonen et al., 2018): 1) Ensuring the study is appropriately “grounded” a. Analysis began as soon as data started being collected. b. Investigators remained open to new and unanticipated findings through the application of a steering group and accountability partners for the lead researcher. c. Codes emerged from the data and can be traced back to this data through documentation. d. Existing knowledge helped make sense of evolving data from the empirical study arms. 2) Capturing and explaining context-related processes and phenomena a. As per GT, data is generated with the aim of understanding the action-interaction and how this comes about in different conditions and contexts. b. Researchers remained attuned to the complex interactions at play. c. Probing of how the phenomena is affected by context and social processes over time was undertaken. d. All of the above were practically outworked through a draft unstructured study protocol, becoming more structured as it became informed through developing ideas. 3) We are pursuing theory by engaging with the data. a. Theorizing can be brought back to and justified by the data. b. Record keeping and documentation of memos and relationships alongside evolving concepts is clear. c. Tentative relationships become more solid when additional confirmatory data is identified. 4) We are pursuing theory through theoretical sampling. a. The theory is sought to explain all processes and phenomena under study. b. Theoretical sampling guided the theory development. c. Theoretical sampling evidenced on how it was applied to gain further insights into emerging categories and concepts in the data.
The way this study was grounded in the iterative data collection and analysis whilst undergoing constant comparison, memoing and diagramming to generate new theories grounded in empirical evidence is outlined within three sequential phases (Glaser et al., 1967; Timonen et al., 2018) (Figure 2). Process of Explicating the Grounded Theory
Methods
Three methods of data collection were applied in this research: semi-structured interviews, demographic and health data collection in a retrospective cohort study, and literature reviews. The mixture of quantitative and qualitative methods gives a deeper insight into complex relationships within larger systems, such as human interactions, and the socio-political landscape they function within. However, when traditional mixed-method approaches are applied, critical cultural nuances are lost. Indeed, integrating multisource data in GT beyond a mixed-method framework has been described, where inductive knowledge builds (or is constructed) through multiple data modes (Sommer, 2021). The three key data sources drawn on for this study method will now be described in more depth.
The first step was collating and synthesizing the current evidence with a specific intent to confirm known knowledge and identify current gaps in the literature before the interview and case data collection, contrary to prevailing methods that delay this step. Although contentious and a potential source of bias, we argue that completing the literature review first clarified our initial codes (Ramalho et al., 2015). Furthermore, the scoping review produced a preliminary conceptual framework, whilst the systematic integrative literature review revealed key themes about patient and health professional experiences in the area of interest to streamline our approach to qualitative inquiry. As the literature was predominantly set in the United States of America, undue biases of how this was interpreted could be minimized since the research of interest was taking place in a unique context (NZ). Further biases were limited through a multi-ethnic steering group, which offered individual insights and accountability.
Scoping Review Method
A scoping review method utilising a narrative format was used to investigate the following research question: What contributes and to what extent do inequitable infant outcomes by race and ethnicity occur in CCHD? Keywords were used to search multiple databases. Eligible articles were those that reported race or ethnicity and included infant outcomes for CCHD. Limits were those published within the last 10 years available in English. The limits were applied to incorporate the most up-to-date knowledge to assist English-speaking researchers. Reviews, conference abstracts, preliminary results, case studies, commentaries, viewpoints, expert opinion articles and those irrelevant to the research question were excluded. The final articles included underwent data extracted in relation to the review question. Moreover, these studies were quality assessed subjectively by SW as outlined by (Al-Jundi (2019); Al-Jundi & Sakka (2017); Page et al. (2021)). After that, papers were grouped by emergent key findings presented in a contextual model.
Integrative Review Method
A systematic integrative review approach was applied to synthesize the available evidence exploring the families’ (nuclear and wider family) and healthcare workers’ experiences of CCHD diagnosis and management (Watkins et al., 2022). Integrative review uses a systematic approach to incorporate studies with diverse methodologies to draw upon a wide range of evidence (Cronin & George, 2020; Whittemore & Knafl, 2005). The resultant thematic synthesis of information aimed to comprehensively deepen the knowledge and understanding of a particular healthcare phenomenon (Cronin & George, 2020; Whittemore & Knafl, 2005).
Qualitative Study Method
Semi-structured interviews were conducted on a national cohort of purposefully sampled parents and health professionals with experience of CCHD in NZ (Watkins et al., 2024). Parents were recruited prospectively after a fetal CCHD diagnosis and offered two interviews at least 3 months apart; multidisciplinary fetal and cardiosurgical health professionals were interviewed once. Interviews were recorded and transcribed verbatim before coding, categorization and conceptual analysis using GT methodology (without the production of a theory) (Watkins et al., 2024).
Quantitative Study Method
The objective was to identify the factors associated with CCHD infant mortality to 1 year (in cases where the pregnancy was chosen to be continued) and to examine how ethnicity influences this outcome within a national cohort in New Zealand (NZ) over 14 years (2006–2019) (Watkins et al., 2025). The study design was a retrospective population-based cohort study of CCHD patients performed nationally through dataset linkage (Watkins et al., 2025). The participants included individuals born with CCHD in NZ from 2006–2019. Terminations were excluded. The main outcome measure was all-cause mortality within the first postnatal year.
Talanoa and Kaupapa Interwoven into the Method
From a methods perspective, Talanoa and Kaupapa data-gathering techniques were incorporated through the co-creation of knowledge (Cammock et al., 2021; Cram & Adcock, 2022); for instance, the qualitative aspects of the project included participatory and inclusive dialogue and storytelling with Māori and Pacific peoples and culturally matched interviewers for Māori and Pacific participants. Hence, holistic wellbeing and spiritual and cultural considerations could be respectfully understood. For the quantitative aspect, there was analysis using the Indigenous Māori and European ethnic groups as the comparator, presenting results to a perinatal committee and feedback from Māori researchers external to the project. Further, all research processes and analysis included cultural oversight, dialogue, and discussion with senior researchers of Pacific and Māori ancestry on the research steering group.
Overarching Grounded Theory Development
All sources of data were coded according to GT methods (Birks & Mills, 2015; Chun Tie et al., 2019; Glaser et al., 1967). A code is a summary word or phrase applied to a segment of data. The lead researcher (SW) wrote a personal position statement and undertook reflexive notetaking and peer accountability throughout these steps to mitigate presuppositions and reduce researcher subjectivity (Olmos-Vega et al., 2022).
Theories encompass enough explanatory power to understand the relationships within data produced through the research methods (Varpio et al., 2020). We used disparate data sources to construct an extant theory advancing the understanding of why inequities in health outcomes occur for infants with CCHD in a multi-ethnic setting of NZ (Charmaz, 2014). This way, sophisticated analytical concepts were promoted with increased richness based on the added nuances of multiple data sources and dialogue.
Within the tenets of GT, the constant comparative method was used to analyze each datum within four phases after coding the data: comparing codes applicable to each category, integrating and relating categories, delimiting the theory within a framework, and writing the theory (Glaser et al., 1967). The data handling or coding of the data was done iteratively, and re-coding took place when the patterns in the data and categories were becoming more refined, alongside the traditional open, selective, and axial coding (Glaser et al., 1967). Each data element was coded separately first. Secondly, diagramming all codes to identify the relationships between codes resulted in emergent categories (Charmaz, 2000, 2014, 2017). Definitive theory generation occurred via in-depth analysis of the categories collated from all data points, which was interwoven into a conditional GT conceptual framework outlined by Corbin and Strauss in 1998, assessing where, what, who, why, how and the consequences (Corbin, 1998; Corbin & Strauss, 2010). Theory building was tracked via memos and dialogue with co-researchers, and phases of theory development remained fluid and iterative as per the GT approach. After that, the final analysis culminated in a theory-guided by multiple perspectives, cultures, values, principles, techniques, and procedures within the tenets of GT (Figure 3) (Charmaz, 2014; Cooper, 2017; Bechhofer & Paterson, 2012). Resultant Grounded Theory Framework.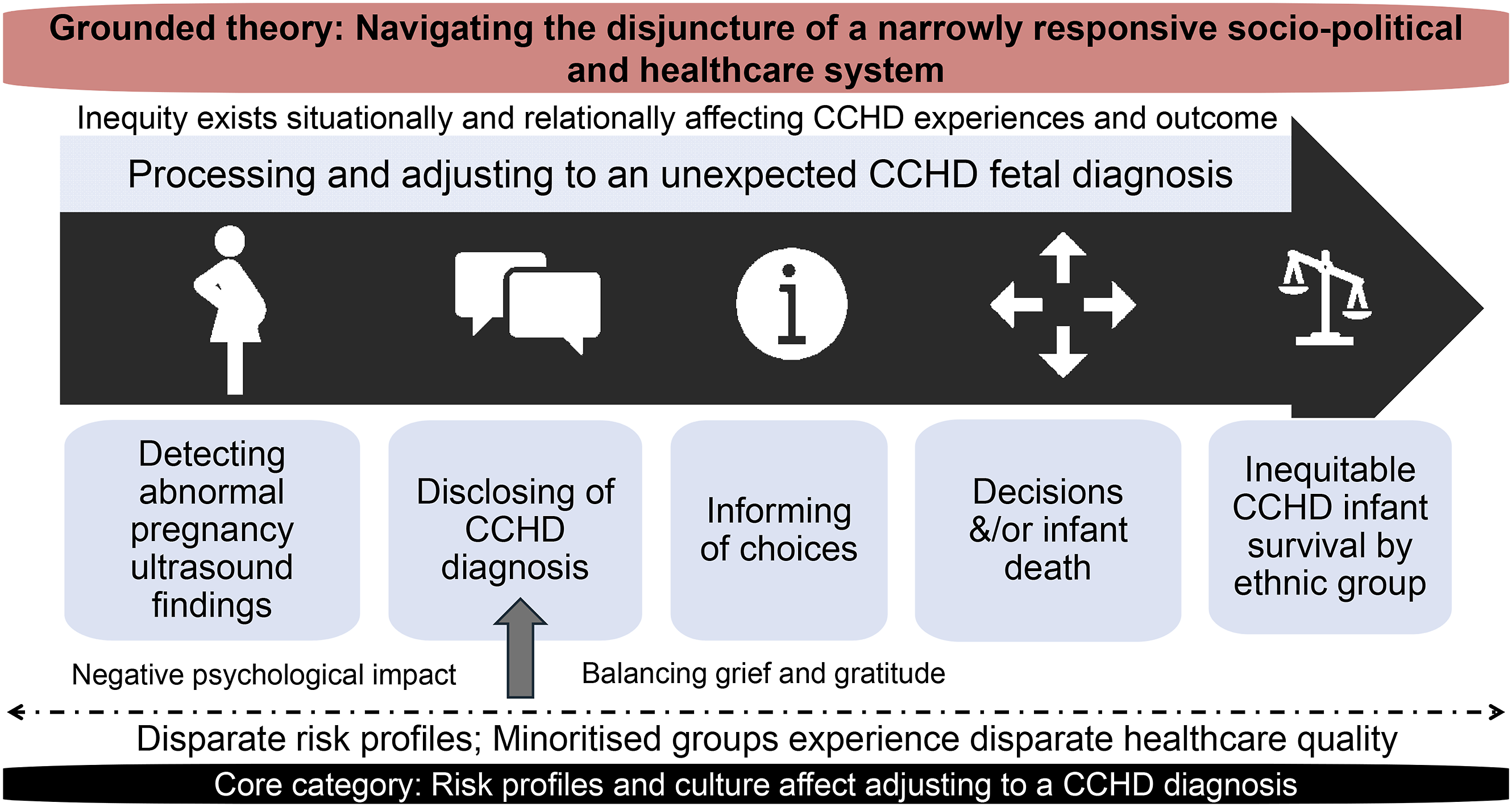
Theory and Findings
Grounded theorists assume participants share a social challenge, which, in the context of this study, was inequitable survival by ethnic group for infants with CCHD. The theory developed was that participants engaged in the social process of navigating the disjuncture of a narrowly responsive socio-political and healthcare system, which was grounded in the multisource data (Figure 3, Supplemental material). Theoretical saturation was achieved where no new insights were added to the data through novel or unique codes or categories.
Expounding Categories Informing Theoretical Model
The parents undergoing a CCHD diagnosis were identified as navigating the disjuncture of a narrowly responsive socio-political and healthcare system as characterized by the elements laid out in Figure 3 – the inter-relationships between risk profiles and culture while relationally and situationally placed in different, unique settings as the parents adjust to the unexpected CCHD diagnosis and balance their grief. These categories are also informed by how the healthcare was perceived and how appropriate families feel the information, relations, support, and self-determination in decision-making was received; this makes up how families perceive the quality of CCHD care. The theory is limited to the time and context in which it was developed and bound within the CCHD healthcare journey. Furthermore, family members of the CCHD child beyond the nuclear family unit were not involved in this study; overseas residents who come to NZ for CCHD management and palliative and intensive care specialists. Thus, the results should be interpreted while keeping the theory’s boundaries in mind.
Key Categories and Codes for Final Grounded Theory.

LR = literature review; CS = cohort study; IP = interview study (parents); IH = interview study (healthcare professionals).
The categories comprised three major categories and one core category underpinned by six sub-categories and multiple codes: • Core category: Risk profiles and culture affect adjusting to a CCHD diagnosis. • Major category: Inequity exists situationally affecting experiences. • Major category: Inequity exists relationally affecting experiences. • Major category: Processing and adjusting.
This grounded theory was informed through the core category of ‘Risk profiles and culture affect adjusting to a CCHD diagnosis’. “Because of the complex situation, [the doctors told us] we’re not gonna do ventilator stuff… the first question he asked me when I told him [his brother] she passed away, he said, ‘Why didn’t the doctors put her on the vent and try to save her?’” - Asian father (P1) “I think they try to [listen to my requests], but for them, it’s a lot like science-based, doctor based and then the family come afterwards, what the mother thinks.” - Māori mother (P21)
The core category explains the overarching social process undergone by the families with the CCHD diagnosis, where immense grief post-diagnosis is balanced by their gratitude for services and options available in NZ, all viewed through unique and individualized cultural lenses. Culture in this context was identified through the data as a fuller indicator of healthcare experience, particularly as models of health and cultural coping strategies and norms were differently developed, as evidenced within the data. “I was talking to my husband, saying, ‘I think he’s [their terminated fetus] a fish from the past life… That made me feel peaceful.” - Asian mother (P18) “We had a prayer… And then we came straight from there [hospital] to the funeral home… It was a tough time ‘cos we didn’t work like we didn’t have enough money to cover all the costs, but his aunty help us pay all the stuff [for the CCHD newborn who died].” - Pasifika mother (P19)
Moreover, the underlying categories of inequity existing situationally and relationally affecting CCHD experiences and outcome was informed through the disparate risk profiles identified through evidence of increased socioeconomic deprivation, alongside birth weight and timing of the CCHD infant. The quote above highlights the financial pressures disproportionately affecting some parents on the CCHD journey, mirrored within the quantitative results.
Context is also vital to document and appreciate within grounded theory, and in this study, the context primarily consisted of the tertiary healthcare system in NZ and the community of the parents of the CCHD infant, including the cultural norms and societal expectations intrinsically linked to these communities. This was important as these contextual conditions affected the adjustment of families and the quality of care experienced, particularly for those belonging to minoritized ethnic groups. Moreover, appreciating the representation of bereaved families within the data was vital, as the experiences were heterogenous – from termination of pregnancy (death), infant death and those with surviving infants.
The 25–31% proportion of deaths in the Māori, Pacific and Asian cohorts with CCHD in the retrospective study compared to 19% in the European group was evidence supporting the overrepresentation of bereavement experienced by non-Europeans in the semi-structured interview study. In addition, the quality of care perceived through suboptimal interactions with healthcare workers was more frequently documented in the Māori, Pacific and Asian parent interviews.
Finally, it was clear that parents underwent a progression of processing and adjusting post-CCHD diagnosis, particularly as it came as an unexpected shock in the pregnancy for both parents. “He [the child’s father] was up all night. He was having panic attacks and anxiety [crying].” - Māori mother (P5)
This journey and decision-making was different for all the families depending on their cultural worldview, diagnostic understanding, location, life stage, and support network, as well as previous experiences with grief and loss. “Sometimes I feel down about it. When the first one passed in 2013, it took me ages to stop, but this one, cos she was born on the same day and she passed away on the same day, so it’s all fine… I'm still finding a way.” – Pasifika mother (P16) “I think they [grandparents of the baby] were relieved when I told them I was about to stop the pregnancy because they were worried that I insist on giving birth because they told me that they know the people around them that had sick baby, but they still gave birth and it’s such a burden for the whole family, not financially, but emotionally.” - Asian mother (P18) “I think that especially with pregnancy and women, miscarriages and all that, we forget that we have feelings and emotions.” –European mother [who had experienced multiple miscarriages] (P4)
Discussion on the Evolved Methodology
The utility of multi-ethnic, multisource GT beyond mixed-method inquiry or traditional GT approaches contributes to the active dialogue on advancing equity through research. Specifically, through ensuring research practice is safe for all ethnic groups participating and represented by the research through incorporating Talanoa and Kaupapa Māori within it. As many ethnic groups access health services in NZ and increasingly within other research settings internationally, this discussion describes the use of this version of GT; this is important because the appropriate inquiry into health equity to inform responses is a pressing global issue.
We suggest that unique knowledge development in the domain of health equity by ethnicity and race requires culturally appropriate guiding philosophical research frameworks, methodology and methods. We present a more expansive take on classical grounded theory, applying multi-ethnic, multisource GT to understand why critical congenital heart disease outcomes differ by ethnicity in NZ. The resultant theory integrated multiple data points within a framework that incorporated elements of Indigenous (Kaupapa Māori) and Pacific (Talanoa) research approaches alongside dominant Western approaches to guide research philosophy and resultant analysis (Goodyear-Smith & Ofanoa, 2022; Johnson, 2017; Martel et al., 2022).
Recent evolution in GT research modes has primarily occurred in social sciences, education, and nursing, with NZ presenting a unique position in advancing different research approaches, as in this medical-orientated study (Goodyear-Smith & Ofanoa, 2022; Martel et al., 2022; Williams et al., 2022). Additionally, GT has the versatility and legitimacy to intentionally integrate multiple cultural views and data types in research, which was perceived to be lacking in contemporary GT or mixed methods approaches available.
Therefore, despite the use of cultural lenses in GT research practice identified previously, to our knowledge, none have incorporated more than one non-Western research methodology and approach into a research design. This research combined mutually respectful worldviews and culture-informed understanding (albeit in tension at times) to enhance learning and inform an innovative research methodology within dialectical pluralism (Johnson, 2017).
We agree with a 2022 report by Lett and colleagues that acknowledging the multidimensional facets involved in research by race should be embedded into quantitative research practices and, in this report, extend this into qualitative research (Lett et al., 2022). Lett supports the need to place more emphasis on the sociocultural landscape and intersectionality of micro to macro factors that impact racial outcomes in research, such as interpreting data through the lens of systemic racism, quoting: “Systemic racism encapsulates all manifestations of racism which may then be further subdivided to individualized and structural racism. Structural racism therefore refers to the compounding impacts of the cultural norms, policies, laws, and practices that produce racial inequity whereas individualized racism refers to the individual and interpersonal manifestations of racial discrimination” (Lett et al., 2022, p. 158).
Lett goes on to outline three key recommendations in undertaking research by race and considering the racist systems and structures at play: 1) use theoretical frameworks that appreciate social and structural influences, 2) co-create research with those being researched, and 3) accommodate systemic racism elements in quantitative and qualitative analysis (Lett et al., 2022). These principles align with the concepts presented in this paper, which champion co-creation, cultural respect through acknowledging different groups ways of knowing and being, and theoretical framing.
We contend that the proposed methodology allows for valued co-creation of research knowledge through partnerships with health consumer groups (particularly those minoritized and marginalized) to enrich insights and translate knowledge into ‘evidence-experience’ practices that service the needs of all societal groups, such as those belonging to different cultures (Archibald et al., 2021; Arumugam et al., 2023; Regnault et al., 2018; Williams et al., 2022). Globally, the frequency of constructionist health research, which partners with patients and the public, has increased (Arumugam et al., 2023; Cornwall & Jewkes, 1995; Smits et al., 2020; Vaughn & Jacquez, 2020). Traction gained from the notion of “nothing about us without us” has propagated the integration of researchers with those being researched as co-creators of knowledge (Charlton, 1998). This further exemplifies the need for the methodological design highlighted here.
Indeed, the difficulty of incorporating a cross-cultural approach must be acknowledged, with tensions and discourses ever-present. Whilst the benefits of GT have been outlined above, these can also be orientated as limitations due to the GT approach’s relative subjectivity, fluidity, and adaptability. Consequently, GT holds the potential for data to be misconstrued, reductive, or misrepresented, although this bias can be reduced by following valid quality measures of qualitative research (Yadav, 2022). What also adds to the rigour of multisource GT is the extra perspectives drawn from diverse data types, theoretically building a more robust theory to capture complexity at a higher level.
In the future, research promulgating an acceptable way of intertwining appropriate cultural lenses in other inequity-laden research settings outside NZ is critical (Cullen & Brennan, 2021; Johnson, 2017; Personal et al., 2022; Sommer, 2021). Furthermore, developing future ethical guidelines that allow for expanding knowledge in a flexible and dynamic format whilst not compromising on data integrity in a multi-ethnic framework will be challenging. We perceive a multi-ethnic research lens reaching beyond biculturalism boundaries is essential to utilize going forward so minoritized groups, such as those representing diverse cultural, religious, abilities, genders, and philosophical contexts, can be respectfully reflected in research findings. We argue that the methodology presented could ensure that the data collected is appropriately analyzed, translated, and applied to challenging areas to advance, such as health equity by ethnicity (Levrau & Loobuyck, 2018).
Conclusion
A re-interpreted approach to grounded theory is described, utilizing a culturally inclusive lens and drawing on disparate data to advance analytical insights into complex multidimensional phenomena such as health inequities. Multi-ethnic, multisource GT was developed as an avenue for respectful and inclusive future health equity research within multination populations.
Supplemental Material
Supplemental Material - Multi-Ethnic, Multisource Grounded Theory: Illustration From a Study Investigating Why Inequities in Survival Occur By Ethnicity
Supplemental Material for Multi-Ethnic, Multisource Grounded Theory: Illustration From a Study Investigating Why Inequities in Survival Occur By Ethnicity by Simone Watkins, Rachel Brown, Sue Crengle, Teuila Percival, and Kim Ward in International Journal of Qualitative Methods
Footnotes
Acknowledgements
Thank you to the members of the ECHO steering group: Professor Frank Bloomfield, Professor Tom Gentles, Dr. Elza Cloete, Dr. Lynn Sadler, Dr. Ruth Gorinski, and Dr. Monique WM de Laat.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by the Health Research Council (HRC) of New Zealand grants, HRC 20/1516 and HRC 21/203. The Health Research Council of New Zealand had no role in the data collection, analysis, interpretation, study design, participant recruitment, or any aspect of the research study. There has been no pay from any pharmaceutical company or agency to write this article.
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.