
Abstract
We developed a realist program theory describing factors that affect healthcare professionals’ delivery of guideline-based pain care in rural Australia as part of a realist-informed needs assessment. To our knowledge, this project is the first to apply a realist research approach to conducting a needs assessment. We conducted and analysed realist informed teacher-learner cycle interviews with rural healthcare professionals to inform our program theory. In these interviews, we presented participants with a summary of guideline recommendations for the assessment and management of chronic pain. We asked participants which recommendations they found easy and challenging to implement in their local setting, and discussed why, how, and in what circumstances this was the case. We detail how we analysed interview transcripts retroductively in NVivo and how the authorship team abstracted from the clinical scenarios provided by interviewees to generate theories at a ‘middle level’ of abstraction. Our discussion details lessons learned from the utilised methods with recommendations for how we would adapt these methods in the future.
Introduction
Healthcare is complex. It is comprised of many types of providers practicing in diverse settings dynamically, and interacting with other actors including politicians, funders, bureaucrats, managers, and patients (Braithwaite et al., 2021). Given the multiple dynamic interdependencies of actors and relationships, healthcare resists simple solutions (Braithwaite et al., 2021). Realist research is well suited to health research capable of informing policy because it is designed to handle complexity by investigating what works, for whom, in what circumstances, how, and why (Pawson et al., 2005; Wong, 2018). Although realist studies are becoming more common, there is considerable variation in how they are being conducted (Pawson & Manzano-Santaella, 2012). The Realist and Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) project generated standards and training materials to improve the quality of realist research (Wong et al., 2016; Wong, Greenhalgh, et al., 2013). Alongside these standards there is a need for more transparent reporting of methods used in realist research (Marchal et al., 2012; Wong et al., 2016; Wong, Greenhalgh, et al., 2013). In response to these calls for transparent reporting, we report on the methods utilised in this realist study. Additionally, we will describe a novel application of realist research – a realist-informed needs assessment.
Study Background
Chronic pain affects 15%–20% of Australian adults (Henderson et al., 2013; Miller et al., 2017), with a higher prevalence in rural, regional, and remote settings than metropolitan areas (Deloitte Access Economics, 2019). Common guideline recommendations for the management of chronic pain include delivering patient centred care with shared decision making, thorough assessment taking, provision of education, and supporting patients to engage in non-pharmacological self-management strategies (e.g., exercise) (Lin et al., 2020). The implementation of guideline-based pain care is variable around the world (Hagen et al., 2016; Zadro et al., 2019). Guidelines often encourage providers to consider their individual patient’s circumstances when implementing recommendations (Wyatt et al., 2014). Deviations from recommended care may be considered necessary in some circumstances due to guidelines often not accounting for or providing guidance on how to manage patient preferences (Krahn & Naglie, 2008), patients’ socio-personal context, and patients with multi-morbidities (Wyatt et al., 2014). When treating patients with multi-morbidities, the degree to which providers deviate from recommended care and the reason informing these deviations have been found to vary according to disease (Cohen-Stavi et al., 2021); with primary reasons being that the provider did not perceive a clinical need to implement recommended care and/or their patient preferred not to follow recommended care (Cohen-Stavi et al., 2022). Additionally, guideline-recommended care may not align with local service delivery models or resource access, which may indicate circumstances when guidelines could be contextualised or adapted for better fit (Dizon et al., 2016). Further investigation into how, why, and when providers deviate from recommended care for chronic pain could help inform future guideline development and implementation initiatives.
Systematic reviews have investigated barriers to guideline-based care for chronic pain, with findings including lack of required knowledge or skills, desire to maintain a good patient relationship, prior training not aligned with guideline recommendations, and short appointment times (Ng et al., 2021; Slade et al., 2016). A previous realist review found that pain care quality is affected when patients receive care through income support systems that dictate what care is funded, that add administrative burden to providers, and that require patients to prove how disabled they are (Di Donato et al., 2020). Other realist reviews have reported that providers implement guideline-recommendations to taper chronic pain patients’ long-term opioid use when providers’ co-workers manage opioid tapering in the same way, when patients and providers have trusting relationships and similar expectations of care, and when providers have supportive resource access such as services to refer patients to and mentors supporting their opioid tapering (Bhattacharya et al., 2022; Lieschke et al., 2020). A strength of realist studies is that they have been able to thoroughly investigate how variable outcomes occur within the complex landscape of healthcare for chronic pain, leading to the generation of policy-relevant recommendations for strengthening programs seeking to improve pain care (Bhattacharya et al., 2022; Hunter et al., 2023; Sud et al., 2020).
To our knowledge, existing research has not investigated factors affecting the delivery of guideline-based pain care in rural settings. We aimed to gain a better understanding of chronic pain care in rural Australian settings by undertaking a needs assessment. As part of this needs assessment, we conducted interviews seeking to understand how chronic pain was managed in rural Australia from the perspectives of a sample of rural healthcare professionals (HCPs) and consumers (Grant, Westhorp, Mardon, et al., 2024). We found frequent reports of guideline concordant provision of providers encouraging exercise and poor use of some guideline-based first line management strategies (such as addressing sleep, nutrition, and social connection), and differences between HCP and consumer reports. While most general practitioners (GPs) and physiotherapists interviewed in this study reported delivering education to patients and generating care and support plans, consumers did not commonly describe receiving these guideline-based aspects as components of their pain care. Contrary to guideline-based care, many consumers reported receiving referrals for medical imaging and described seeking treatments with uncertain benefits. It should be noted that the consumer participants were not patients of the interviewed HCPs, which may have contributed to the differences in reported care. Nonetheless, this study identified gaps between the care recommended by guidelines and the care provided for chronic pain in rural Australian settings.
We chose to apply a realist approach to gain a deeper understanding of these gaps. Specifically, we sought to gain an understanding of how rural-based factors affect the delivery of guideline-based pain care in rural Australia. We informed our planning of this realist study through early work on a formal realist review investigating factors affecting the uptake, implementation, and sustainability of increased access to pain services in rural settings (Grant, Westhorp, Murray, et al, 2024). This review included input from two interest-holder groups comprised of academic researchers and representatives from organisations supporting provision of rural Australian healthcare services. Work on this realist review helped us to identify how rural Australian pain care is negatively affected by local resource access, busy practice environments, short appointment times, and specific patient challenges including financial hardships and multi-morbidities. Further, factors positively affecting rural Australian pain care included providers having an interest in chronic pain and positive patient relationships. This information helped us develop early realist hypotheses, or program theories, regarding how rural-based factors affect the delivery of guideline-based pain care in rural Australia. In this manuscript we will describe the methods we utilised to further develop our realist program theory. A future article will report our further refinement and consolidation of this program theory.
Methods
Research Design
Needs assessments (1) investigate gaps between what is presently happening and what is desired to be happening, (2) gain an understanding of what is contributing to these gaps, and (3) generate recommendations for addressing these gaps (Sleezer et al., 2014; Stefaniak, 2020). We sought to develop a realist approach addressing aims two and three of conducting a needs assessment because realist methods enable researchers to develop an understanding of how and why things work differently in different circumstances. Traditionally, realist research seeks to evaluate programs (Pawson et al., 2005). For this study, we did not evaluate a program, rather we utilised realist principles to understand how, why, for whom, and in what circumstances rural HCPs implement guideline-based pain care, and how, why, for whom, and in what circumstances they do not.
In line with much realist research, we utilised context-mechanism-outcome (CMO) configurations for analysis (Pawson et al., 2005). Contexts (C) are the circumstances affecting which mechanisms operate (Wong, Westhorp, et al., 2013), and mechanisms (M) describe responses to resources in specific contexts that generate a certain outcome (O) (Pawson & Tilley, 1997). For example, when a mobile vaccine clinic is offered to consumers in a rural setting with minimal access to other vaccine services (C), the rural consumers perceive the mobile vaccine clinic to be convenient to access (M), so they visit the mobile clinic to get vaccinated (O) (Wong, 2018). This convenience mechanism is context-dependent because in another setting with greater service access, consumers may not perceive the same benefit from the convenience, thus may not visit the clinic to get vaccinated (Wong, 2018). A traditional realist study develops a program theory of CMOs describing both expected and unexpected outcomes of the program and the factors causing these outcomes (Wong, Westhorp, et al., 2013). For this realist needs assessment, we developed a program theory of CMOs describing both guideline-based and non-guideline-based pain care treatment decisions and the factors affecting these decisions. Program theories are the assumptions, ideas, and hypotheses that inform program planning and relate to how a program needs to be structured to generate desired outcomes (Pawson & Tilley, 1997). Theory-driven research approaches, such as realist approaches, start by identifying these program theories and then testing them. We chose to refer to our generated theory as a ‘program theory’ despite not evaluating a ‘program’ because of the common use of this term in realist work.
To start the program theory generation process, the authorship team generated initial hunches of factors they predicted may cause rural HCPs to deliver guideline aligned and guideline divergent pain care. The authorship team includes experts in pain care [GLM, PhD, Distinguished Professor], realist research [GW, PhD, Professorial Research Fellow], implementation research [PDH, PhD, Program Manager], and social determinants of health [ELK, PhD, Postdoctoral Research Fellow], as well as a rural Australian GP [CR] and an early career researcher with advanced knowledge regarding the role of pain-related education [AM, PhD, Postdoctoral Research Fellow]. This team was led by a PhD candidate investigating rural Australian pain care [ARG, MCogBehavTherapy]. Initial theorising was informed by early work on the previously described realist review investigating factors affecting the uptake, implementation, and sustainability of increased access to pain services in rural settings (Grant, Westhorp, Murray, et al, 2024), and by authorship team discussions informed by each team member’s relevant knowledge and expertise. This program theory informed our study planning.
Ethics
This project received ethics approval from the University of South Australia Health Research Ethics Committee (application #204795).
Recruitment
We recruited rural HCPs through networks of our research team. HCPs were eligible if they (1) worked in healthcare as a medical or allied health provider in the last 12 months, (2) worked in or near a town with a population between 15,000–50,000 for a minimum of three months in the last 12 months, and (3) supported chronic pain patients in a rural, regional, or remote setting in the last 12 months. We scheduled respondents for either a telephone or video-based interview. Prior to this interview, we sent participants an online survey hosted on the Qualtrics platform (Qualtrics, 2020) to confirm their eligibility, provide their consent to participate, and to record their demographic details.
Data Collection
We conducted semi-structured interviews and referenced a topic guide of questions that we sent to participants prior to their interview [Supplemental File 1]. We followed recommendations for conducting realist interviews by utilising teacher-learner cycles (Manzano, 2016; Pawson & Tilley, 1997). Specifically, we taught participants about our present program theory and then the participants taught the interviewer about their experiences that aligned with, or diverged from, this program theory (Manzano, 2016). At the start of the interview, we asked participants about their work environment and the extent of their experience treating chronic pain patients to gain an understanding of their expertise and experience.
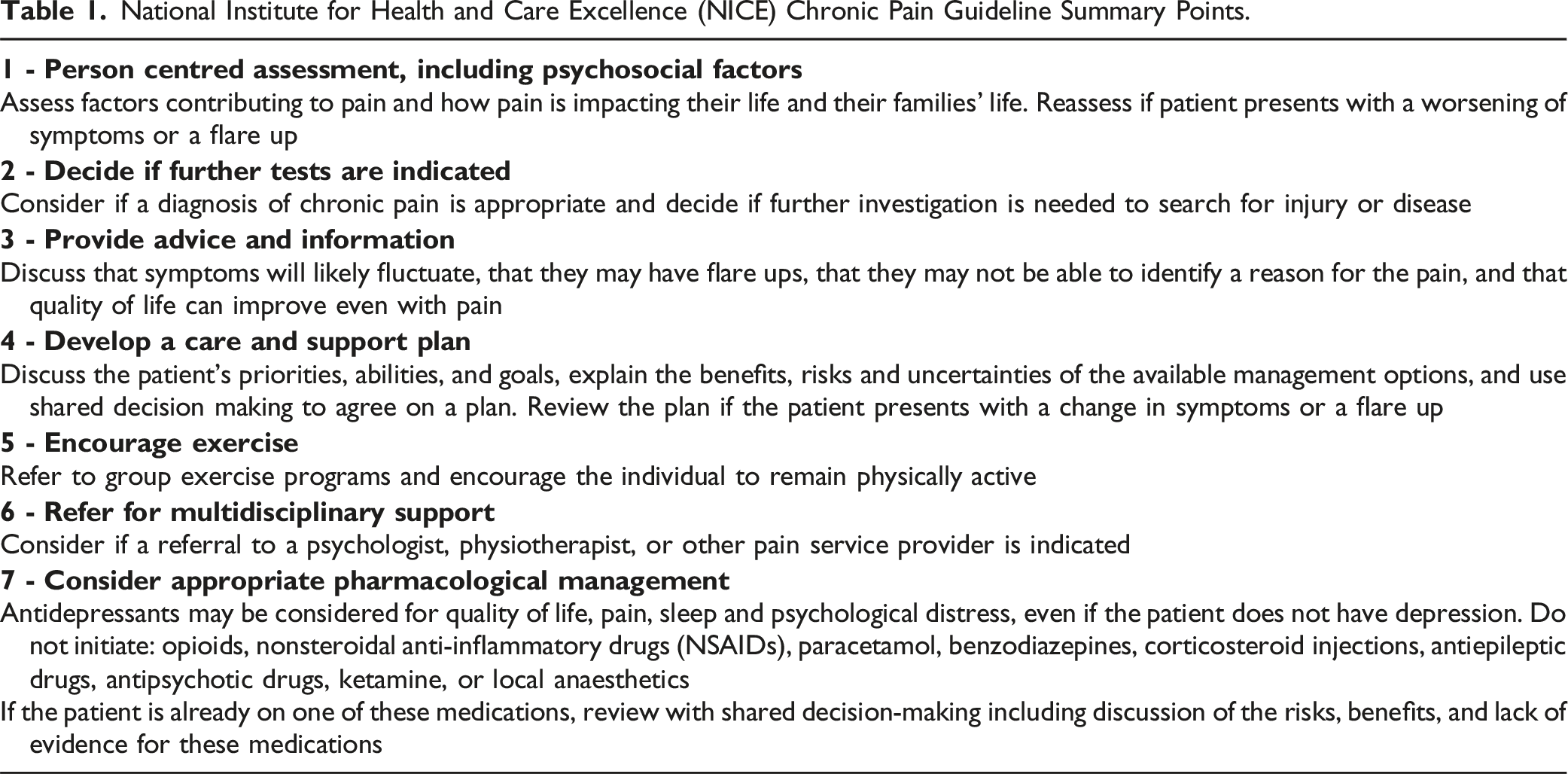
National Institute for Health and Care Excellence (NICE) Chronic Pain Guideline Summary Points.
One author [ARG] conducted all interviews. This author is a PhD candidate investigating rural chronic pain management. She has prior experience in qualitative research methods and training in realist research methods (provided by GW and a course delivered online). We audio recorded all interviews with participants’ informed consent and a transcription service transcribed the recordings verbatim.
Data Extraction and Analysis
We descriptively analysed quantitative demographic survey data in Excel and conducted qualitative realist analysis in NVivo (Lumivero, 2020). In line with recommended realist theorising, we utilised retroductive analysis (The RAMESES II Project, 2017). Specifically, we relied on inductive reasoning to generate new CMOs when new elements or linkages were identified in the data, deductive reasoning to code to existing codes, and incorporated informed hunches generated using the authorship team’s diverse expertise (The RAMESES II Project, 2017). At the start of coding, authors ARG and AM extracted and analysed data from 30% of interview transcripts to incorporate two perspectives on the initial raw data analysis. AM contributed knowledge of guideline-based pain care and prior qualitative research experience. After individually extracting and collaboratively analysing data from 30% of the transcripts, author ARG independently extracted data from remaining transcripts. Authors ARG and AM held regular meetings to review data coded to new CMOs and to discuss uncertainties regarding data extraction and analysis.
We utilised NVivo by adapting the processes described by Dalkin et al. (2020) and Gilmore et al. (2019). We supported our coding by generating a document detailing how to utilise NVivo and what information to look for when coding interview transcripts [see Supplemental File 2]. We generated top level codes for each of the seven guideline summary points and generated second level-codes for CMOs under each summary point. When we combined multiple CMOs, we generated a new second level-code, nested the superseded CMO codes underneath, and turned on ‘aggregate coding from children’. We present an example of our NVivo coding structure in Supplemental File 3.
Adaptation of Gilmore et al.’s (2019) linked memo structure for analysing coded data.

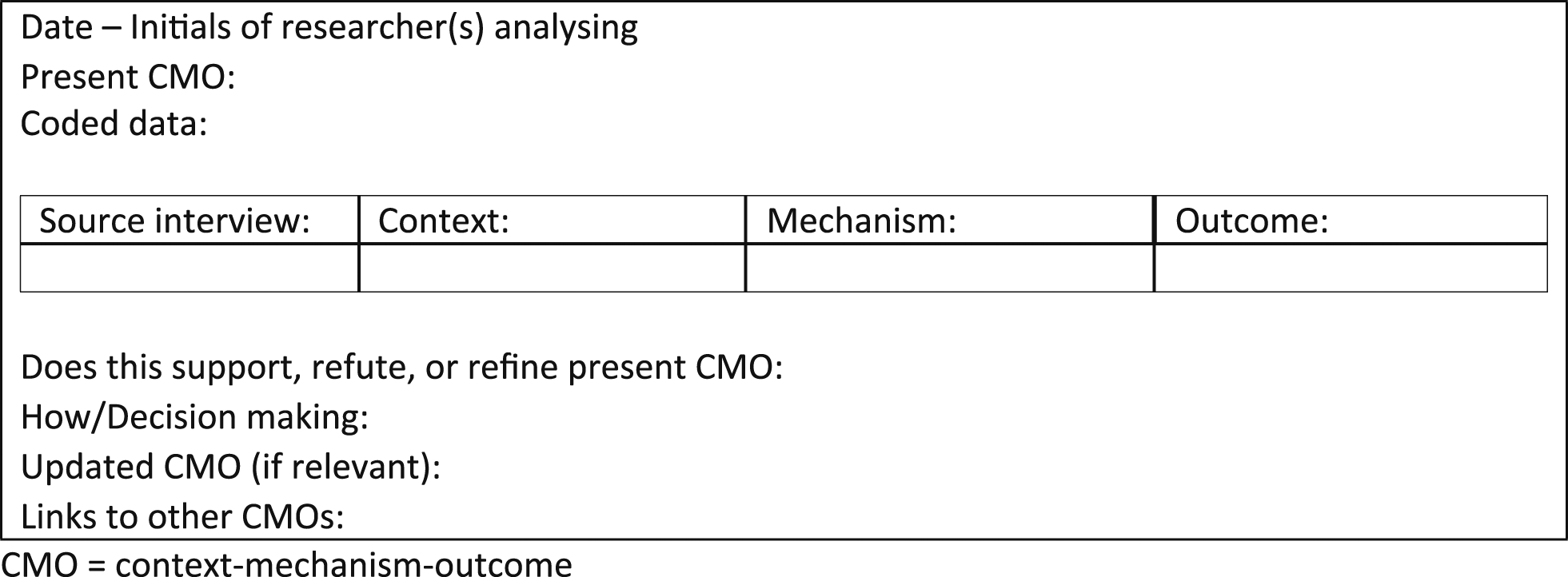
Linked memo structure for combining context-mechanism-outcome configurations into a new context-mechanism-outcome configuration.


After an initial review of all interview transcripts, we printed the linked memo for each CMO. This allowed us to physically group CMOs describing similar concepts and to review CMOs alongside the data informing each CMO in authorship team meetings. We utilised the authorship teams’ diverse expertise to abstract out, from the individual clinical scenarios that the interviewed providers described, to theorise more generalisable mechanisms driving the clinical scenarios. Realist expert GW repeatedly reviewed the CMOs to ensure consistency with principles of realist research.
Abbreviated example of final phase of analysis of context-mechanism-outcome configurations for the program theory.


Results
Demographics
We interviewed fifteen HCPs. Most were male (80%), and the mean age was 43 years (SD 8.38). HCPs included GPs (n = 9), physiotherapists (n = 4) and hospital doctors (n = 2), with a minimum of 5 years clinical experience, and more than a quarter with 20+ years of experience (27%). These HCPs worked in South Australia (73%), Western Australia (20%), and Victoria (7%), and the majority lived in the setting in which they worked (93%). All interviewees worked in medium to large rural towns, and the majority (60%) had worked in a rural, regional, or remote setting for less than 10 years. A detailed demographics table is presented in Supplemental File 4.
HCPs' Perspectives on Ease of Implementing Guideline Recommendations
The guideline summary points most frequently described as easy to implement included taking a person-centred assessment (n = 3), deciding if further tests were indicated (n = 4), and providing advice and information (n = 4). The recommendations most frequently described as challenging to implement included reviewing patients’ previous diagnostic history to decide if further testing was indicated (n = 3), developing a care and support plan (n = 5), and referring for multidisciplinary support (n = 11). Encouraging exercise was relatively often mentioned as easy to suggest to a patient but challenging to get the patient to action (n = 5). Further discussion of how, why, and when it was challenging to implement guideline-based care is provided in the presentation of the program theory section.
Program Theory Generation Process
Example of Combining Context-Mechanism-Outcome configurations From One Guideline Summary Point That Share a Common Underlying Mechanism.

CMO = context-mechanism-outcome.
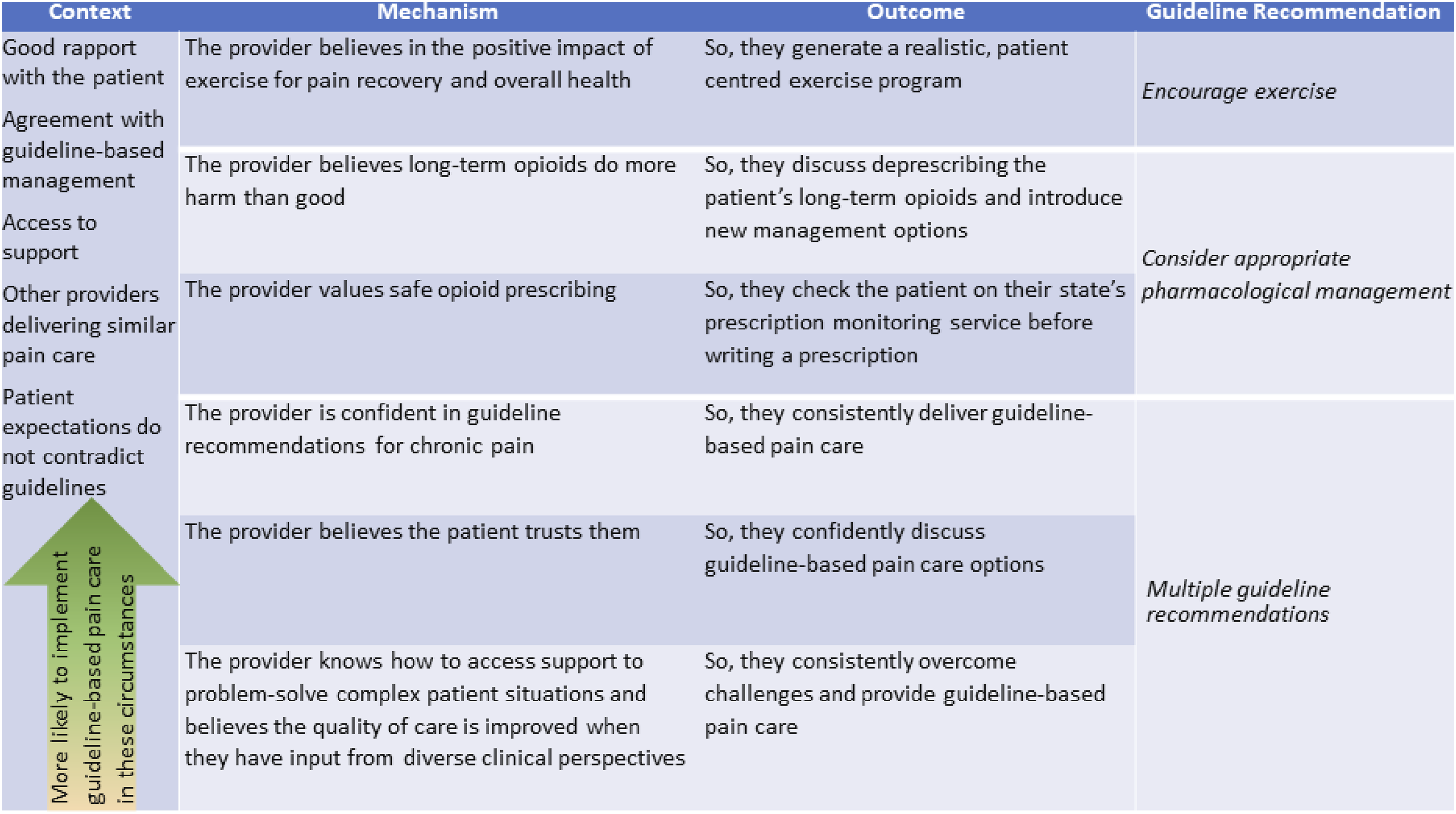
Example of Combining Context-Mechanism-Outcome configurations From Multiple Guideline Summary Points That Share a Common Underlying Mechanism.

CMO = context-mechanism-outcome.
Presentation of the program theory
Realist theory is refined iteratively. In this stage, we synthesised the initial 53 CMOs to arrive at 16 CMOs. Figures 1 and 2 provide a simplified presentation of these CMOs, organised according to the seven guideline-summary points. We chose to present the program theory in this simplified format because we identified that many of the contextual factors positively and negatively affecting the delivery of guideline-based pain care in rural Australia were consistent across the CMOs. Additionally, the aim of this paper was to describe the program theory generation process, rather than the content of that theory. A more detailed, and more realist, presentation of each CMO is presented in Supplemental File 5. This iteration of the program theory was then refined using subsequent focus groups with rural HCPs. Presenting the refined program theory in detail is beyond the scope of this article and will form the focus of a subsequent publication. Context-mechanism-outcome configurations for factors negatively affecting the delivery of guideline-based pain care. Context-mechanism-outcome configurations for factors positively affecting the delivery of guideline-based pain care.
Discussion
This paper describes our generation of a program theory for a realist-informed needs assessment. We started our program theory generation with a base level of knowledge informed by authorship team hunches and prior work on a realist literature review. We evolved our understanding through teacher-learner cycle interviews with rural HCPs that we analysed in NVivo. Our initial NVivo coding relied primarily on inductive and deductive reasoning and resulted in a large number of CMOs based on specific clinical experiences. These CMOs were refined by abstracting out to more generalisable mechanisms through printing and physically grouping documents and incorporating the authorship team’s diverse expertise. This program theory will now undergo further refinement through focus groups with additional rural HCPs. The resultant program theory produced by this realist-informed needs assessment will detail the final mechanisms that we identify as causing, or contributing to causing, our outcome of interest: the implementation or non-implementation of guideline-based pain care. This program theory will be utilised to generate recommendations for supporting the delivery of guideline-based pain care in rural settings.
Realist research offers a framework for investigating the complexity that comes with real-world implementation, which allows realist investigations to focus both on what works and what does not work to enable learnings to be drawn from both successes and failures (Rycroft-Malone et al., 2012). A realist program theory seeks to identify the processes causing and contributing to causing these successes and failures, which helps uncover insights that remain hidden by other experimental research designs (Porter & O’Halloran, 2012). A further strength of the realist approach is that the generated program theory is abstracted such that it can be applicable to other topics and settings than those that the original study sought to investigate (Pawson & Tilley, 1997). The findings and recommendations generated by the present study will be most relevant to the provision of guideline-based pain care in rural Australian settings but may also be relevant to other types of guideline-based care in rural Australia, to pain care in rural settings outside of Australia, and/or to other low resource settings. It is important to note that contexts and the mechanisms that they trigger may be disrupted or enhanced by differences in social influences, such as political, legal, economic, moral, religious, and cultural climates. A criticism of realist program theories is that they may overlook some of these and other important social influences (De Souza, 2015; Porter & O’Halloran, 2012). Realist research does not seek to present findings that are representative of all circumstances, rather realist research seeks to identify essential causal processes that are transferrable to other circumstances (Pawson & Tilley, 1997). This is done through studies abstracting theories that can be refined and tested through further investigation.
Lessons Learned
Interview and Analysis Timing
We found it beneficial that the researcher conducting the interviews possessed relevant knowledge derived both from the literature and the expertise of the authorship team prior to conducting the interviews. This aligns with recommendations for realist theory gleaning interviews to be informed by “tentative theories” (Manzano, 2016, p. 354) or assumptions of what the researchers think is happening. Further, our use of a consistent interviewer allowed this individual to query content from previous interviews, thus continually evolving their understanding with participants.
One of the weaknesses of our interview process was that we conducted all interviews over one month and did not start data analysis until all of the interviews were completed. This may have impeded the depth of our interviews because the interviewer was unable to query gaps in our understanding that were not identified until formal analysis. Additionally, the novice interviewer’s realist understanding and interviewing skills improved as the study progressed. Thus, conducting interviews over a longer period of time could have improved the quality of questions asked in subsequent interviews. For this study, we accepted these weaknesses because we planned to conduct subsequent theory refining focus groups, involving participants from these individual interviews. In future studies, we could consider conducting several, iterative rounds of interviewing and analysis.
Diverse Input into Program Theory Generation
The diverse backgrounds of our authorship team strengthened our theorising, as did having two authors extract initial data, which enabled two interpretations of raw interview data. We incorporated perspectives from authors with expertise in pain science and care, implementation science, social determinants of health, and realist research, as well as a rural HCP. This rural HCP initially participated in an interview and was later invited to join our authorship team based on their demonstrated extensive knowledge and experience implementing guidelines for chronic pain in rural settings. Involving members of the relevant population in research processes is important for increasing the relevance of health research, improving public confidence in health research, and producing results that meet the needs of the community (Cochrane, 2017; Consumers Health Forum of Australia & National Health and Medical Research Council, 2016; World Health, 2015).
An area of weakness in our research team was that the researchers who extracted and analysed the interview data were new to realist analysis. This likely reduced the depth and quality of our realist analysis. We combatted this weakness through ensuring the oversight of a realist expert [GW], who regularly revised the program theory and provided guidance. Additionally, the document we generated that detailedo how to conduct realist analysis helped to guide these realist novice researchers. Another weakness was that we only interviewed one population group – rural HCPs. In future studies, we could consider recruiting participants with more diverse backgrounds, such as policy makers and rural consumers, to gain more diverse viewpoints on the topic. This would align with recommendations for realist interviewing of gathering interest-holders with diverse viewpoints (Manzano, 2016).
Use of NVivo
Our adaptation of the processes described by Dalkin et al. (2020) and Gilmore et al. (2019) for using linked memos enabled easy tracking of and reference to theory refinement decisions. It was particularly helpful that we copied data from superseded linked memos when combining CMOs because this improved ease of reference to all data coded to each final CMO. Similarly, organising extracted and analysed data into the interview source, context, mechanism, and outcome tables enabled clear visualisation of data for each CMO.
We found it challenging to continue updating the linked memos after we printed them and started utilising Word documents. It was necessary to use Word documents for team review because the full authorship team did not have NVivo access. Additionally, it was easier to see the large number of CMOs when printed. In future studies, we could trial uploading all generated Word documents, including versions with comments from co-authors, as well as all email correspondence discussing theory refinement, into NVivo. This would enable us to keep all records in one place, improving ease of reference. Additionally, this could enable coding of author theory refinement comments to the relevant CMO codes, then analysis of these coded comments in the linked memos using the same methods applied for all other coding.
Conclusion
We developed a realist program theory describing factors that affect HCPs’ delivery of guideline-based pain care in rural Australia as part of our realist-informed needs assessment. To our knowledge, the overall project will provide the first reported realist-informed needs assessment. This paper contributes to that goal by describing the theory generation process in detail. We have described how we incorporated diverse inputs from participants and the authorship team into our program theory generation, our use of NVivo for data analysis, lessons learned and recommendations for future methods considerations. Through providing a transparent report and evaluation of our process, this paper provides a useful guide for novice realist researchers.
Supplemental Material
Supplemental Material - Realist Needs Assessment Investigating the Factors Affecting Implementation of Guideline-Based Care for Chronic Pain in Rural Australia: Program Theory Generation
Supplemental Material for Realist Needs Assessment Investigating the Factors Affecting Implementation of Guideline-Based Care for Chronic Pain in Rural Australia: Program Theory Generation by Ashley R Gran, Gill Westhorp, Amelia Mardon, Emma L Karran, Peter D Hibbert, Christopher Roeger, and G. Lorimer Moseley in International Journal of Qualitative Methods.
Footnotes
Author Contributions
ARG contributed to Conceptualization, Methodology, Investigation, Resources, Formal analysis, Visualization, Writing - original draft, Writing – review & editing, Project administration, Revisions for journal. GW, ELK, and PDH contributed to Conceptualization, Writing - review & editing, Supervision. AM contributed to Formal analysis, Writing - review & editing. CR contributed to Data curation, Formal analysis, Writing - review & editing, GLM contributed to Conceptualization, Writing - review & editing, Supervision, Funding acquisition.
Declaration of Conflicting Interests
GLM has received support from Reality Health, ConnectHealth UK, AIA Australia, Institute of Health, California, Kaiser Permanente, Workers’ Compensation Boards in Australia, Europe and North America, and various sporting clubs. GLM receives royalties for books on pain and speakers’ fees for talks on pain. GLM has received support from professional societies and government agencies to present research findings at scientific meetings and to government representatives. ELK receives support from professional societies to present research findings at scientific meetings. ARG, AM, GW, CR, and PH declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Rural Doctors Workforce Agency; National Health and Medical Research Council; 1178444.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.