
Abstract
Keywords
Background
Cancer is a major public health problem in Europe, accounting for over 4 million new cancer cases and 1.9 million cancer-related deaths in 2020 (Dyba et al., 2021). It has been estimated that around 40% of cancer cases could be prevented and mortality reduced (Brown et al., 2018) by adopting primary and secondary prevention actions and interventions (Vineis & Wild, 2014). Therefore, prevention offers tremendous public health potential and the most cost-effective long-term cancer control strategy (Espina et al., 2018).
Successful cancer prevention requires evidence-based, effective preventive measures at the individual level and public policies at the population level that create healthy environments and the healthcare system infrastructure needed to prevent cancer (Feliu et al., 2023). Although knowledge is often not enough to change behaviour, for individuals to successfully engage in preventive measures, they must understand why they need to adopt them.
The European Code Against Cancer (ECAC) is a set of cancer prevention recommendations that informs the public about how to avoid or reduce exposure to established causes of cancer, adopting healthy behaviours to reduce cancer risk, and participating in vaccination and screening programmes under the appropriate national guidelines (Schüz et al., 2015). European health authorities and civil society organizations have also used the ECAC as a key tool to improve the population’s health literacy about cancer prevention (Feliu et al., 2023).
The ECAC is an European Commission (EC) initiative, first launched in 1987 and updated thrice. The last edition of the ECAC (fourth ed.), launched in 2014, was coordinated by the International Agency for Research on Cancer (IARC/WHO) with the participation of experts in cancer prevention, epidemiology, behavioural change and communication across the European Union (EU). This edition consisted of 12 recommendations covering the following topics: smoking and other forms of tobacco use; second-hand smoke; healthy body weight; physical activity; healthy diet; alcohol consumption; exposure to ultraviolet radiation; occupational carcinogens; radon; breastfeeding; hormone replacement therapy; human papilloma virus and hepatitis B virus vaccinations; and bowel, breast and cervical cancer screening. In 2021, the EC adopted the Europe’s Beating Cancer Plan (European Parliament and the Council, 2021) and announced the update of the ECAC to improve health literacy on cancer risk and its determinants and preventive measures. IARC was commissioned to coordinate the update of the fifth edition that will be launched in 2025.
The last EU Joint Action on Cancer (Innovative Partnership for Action Against Cancer, iPAAC) concluded that an update of the ECAC monitoring and follow-up strategies is needed (Espina et al., 2021). In 2017, Ritchie et al. evaluated for the first time the impact of the ECAC (fourth ed.) and found that, although the awareness of the ECAC was low among the public, their willingness to make behavioural changes for cancer prevention after reading the recommendations was over 60% (Ritchie et al., 2021). However, further research is needed to understand the internal and external contextual factors conditioning the uptake of cancer prevention measures.
In all, the commission to develop the fifth edition of the ECAC offered the opportunity to conduct a formative research study to inform the ECAC’s update by describing the perceptions of the target audience about the ECAC, fourth edition, understanding the factors that influence changes in behaviour and investigating the best ways to reach the public.
Aim and Main Research Questions
This study explores individuals’ perceived capability, opportunity, and motivation to adopt cancer prevention measures recommended by the ECAC (fourth ed.), and to identify the barriers and facilitators to adopt the recommendations among a sample of the population in selected EU Member States (MS). The main research questions are: ⁃ What are individuals’ main barriers and facilitators to adopting cancer prevention measures? ⁃ What are the main motivations for changing unhealthy behaviours to adopt the recommended cancer prevention actions? ⁃ Are there differences in the perceived barriers, facilitators, and motivation factors across countries, social groups, or age groups?
Theoretical Framework
Understanding behaviour and behavioural change is crucial to maximise the potential impact (Davis et al., 2014) of the ECAC’s recommendations. Theoretical frameworks identify factors believed or found to influence behavioural change outcomes. Indeed, the COM-B Model of Behaviour has been widely used to identify what needs to change for a behavioural change intervention to be effective. This model identifies three factors that need to be present for any behaviour to occur: capability (C), opportunity (O), and motivation (M) (Michie et al., 2011). In other words, it states that in order for individuals to perform a particular behaviour (i.e., to adopt a cancer prevention measure), they must feel that they are both psychologically and physically able to do so (C), have the social and physical opportunity for the behaviour (O) to happen, and want or need to carry out the behaviour more than other competing behaviours (M) (Michie et al., 2014).
According to the COM-B model developed by Michie et al., each factor is described as follows: ⁃ Capability is an individual’s psychological (knowledge, comprehension, reasoning, psychological strength) and physical (skills, abilities) capacity to perform or engage in the behaviour concerned. ⁃ Opportunity is defined as all the external factors outside an individual that make a behaviour possible or prompt it, including physical (resources, time, location) and social factors (cultural norms, social cues). ⁃ Motivation is the reflective (plans) and automatic (desires, impulses) brain processes that energise and direct behaviours, not just goals and conscious decision-making. ⁃ Behaviour is any action a person takes in response to internal or external events.
As illustrated in Figure 1, these factors interact over time to generate behaviours that may, in turn, affect these factors. Hence, behaviour is part of a dynamic system (Willmott et al., 2021), in which motivation is a core part, with positive and negative feedback loops. COM-B Model from Michie S et al. [12].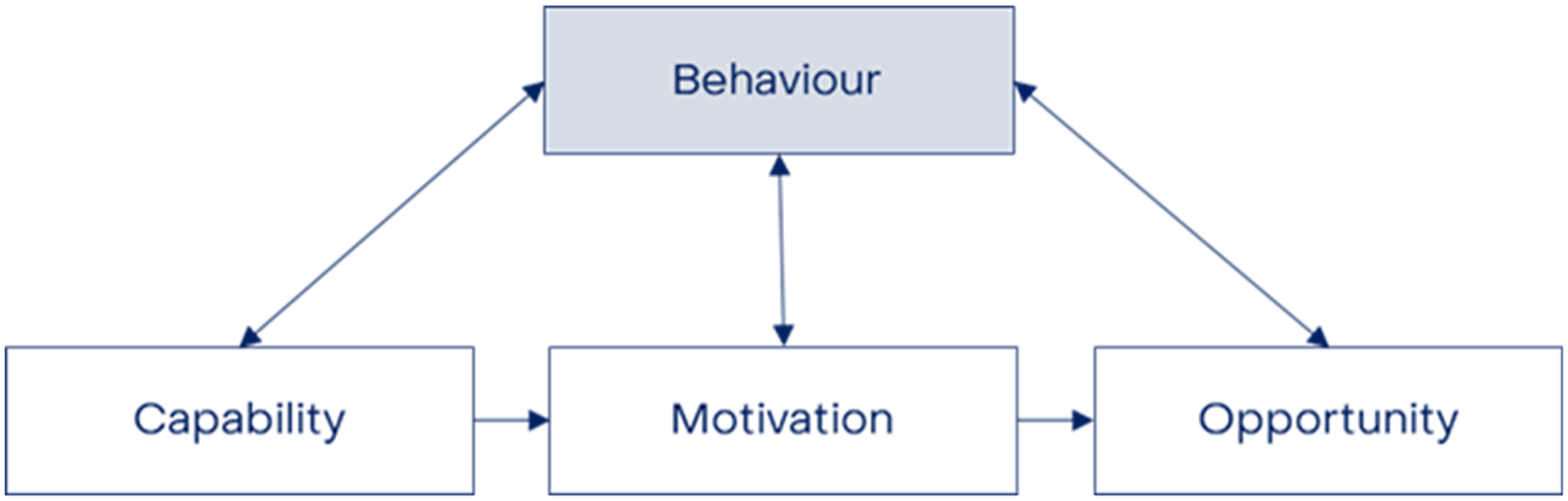
Methods
Study Design
An exploratory research multi-country qualitative study with a narrative approach (Butina, 2015) is conducted to understand how individuals perceive the messages of the ECAC (fourth ed.) and make sense of their previous and future experiences (capabilities and opportunities) and motivation towards adopting the cancer prevention individual measures recommended in the ECAC.
Study Population
Participants
Participants are 18 to 65 years old adults with no previous diagnosis of cancer living in one of the nine participating EU MS (Bulgaria, Croatia, France, Germany, Ireland, Poland, Portugal, Romania, and Spain). EU MS were selected to cover all the EU regions (Southern, Northern, Central and Western) and having a representation of MS with different population sizes.
Recruitment Process
In each EU MS, the local research team decides which of the proposed channels and settings are adequate in their context to recruit people who meet the inclusion criteria. An informational leaflet summarizing the study is being disseminated through different channels, including but not exclusively social media, newsletters, and word of mouth. It is also being distributed in different settings (e.g., at churches, local markets, supermarkets, malls, gyms, universities, community centres, etc.) to reach participants in the community.
Researchers provide all potential participants with an information sheet about the study in its entirety (i.e., purpose, methods, data management) and offer them the possibility to participate. Potential participants can freely decide whether they want to participate or not during the interaction with the interviewers without rushing them to make a quick decision and allowing them to ask any questions regarding the study. Afterward, an appointment is set to interview with those individuals who agreed to participate.
Before starting the interview, participants are asked to provide their oral consent stating that they have been informed about the study, participate in it voluntarily, and agree to be audiotaped. Considering that they understand the aim of the interview and made an informed decision to participate, they are also made aware of their entitlement to withdraw at any stage of the interview for whatever reason, to withdraw data just supplied, and/or not to answer specific questions.
Recruitment kicked off in February 2023 and is still ongoing in Bulgaria, and Romania.
Sampling and Data Collection
Description of Pre-defined Interviewee Profiles.

For data collection, in-depth semi-structured interviews with open-ended questions (Busetto et al., 2020) are being conducted to understand and capture participants’ points of view about the cancer prevention measures recommended in the ECAC (fourth ed.) (Patton, 2015). Each participant is interviewed by a trained interviewer using a topic guide designed for this project, including a list of general questions organized in broad areas of interest to help them structure the conversation.
Interviews take place in person in participating organizations’ facilities, if possible, or in other available public places where participants feel comfortable and safe. If in-person interviews are not possible, they are conducted using online communication software [i.e., Zoom or Microsoft Teams].
Rigour
Application of Qualitative Rigour (Lincoln & Guba, 1985).

Data Management and Confidentiality
Interviews are recorded using an audio digital encrypted recording device. The interviewer will download the audio and send it to the leading research team via an encrypted site designed for sharing documents with external collaborators, totally anonymized and identified only with the corresponding profile number and country. No information identifying participants will be recorded since the only personal variables that will be registered will be the EU MS where participants live, sex, age group (18 to 30, 31-45, and 46–65 years old), and level of education (high, secondary, and primary or less).
Encrypted audio will be manually transcribed and then translated into English using an Artificial Intelligence (AI)-aided software for analysis. English translations will be backchecked by the local research teams in each EU MS to ensure accuracy. Once transcribed, all audios will be eliminated, and transcripts stored at the local servers of the leading research team for the length of the study (24 months).
Data Analysis
A two-stage analysis of the data will be conducted: (1) a thematic content analysis (TCA) to descriptively present the data by identifying common themes or thematic nodes in the texts provided for analysis (Anderson, 2007; Braun & Clarke, 2006). All data are imported to Atlas.ti V24 to facilitate data organization and analysis. Transcribed data in English will be coded with one or more short descriptors [keywords] of the content of a sentence or paragraph to sort data into specific “theoretical” terms using qualitative data management software. These codes will be grouped, summarised, and classified (coding frame) to achieve data abstraction and synthesis. After coding is completed, codes will be clustered into themes or narratives based on the COM-B Model of Behaviour (Michie et al., 2011). The first round of text screening and data codification will be conducted using an AI-assisted tool due to the substantial number of interviews included in the study. This AI-based natural language processing tool uses linguistics and machine learning to comprehend, interpret, and produce human-style language. Two independent researchers (AF, BB), before proceeding with the thematic analysis, will check AI-proposed codes to guarantee validity and reliability of the results, and ensure interpretative control (O’Connor & Joffe, 2020). If discrepancies emerge, divergences will be solved by discussing them with a third researcher (CE). All authors will discuss identified common themes to refine the analysis.
In the second stage, (2) a critical analysis of participants’ discourse (CDA) to examine the processes underlying discursive production, dissemination, and assimilation (Johnson & McLean, 2020) will be conducted. CDA investigates both the content of communication and how it is conducted, including the socio-political and cultural context, social dynamics, and ideologies surrounding the use of language. Researchers from the leading team will identify the discursive practices in the text. Once all discursive practices are identified, together with the research team in each EU MS, the larger social context that bears upon the text and the discursive practices will be discussed to understand and explain the power and social relations, norms, practices, and structures that influence the actual production of the text (Mogashoa, 2014; Mullet, 2018) in each of the participating EU MS and at EU-level, if possible.
Ethical Consideration
The key ethical concerns of the study are: (1) data anonymity and confidentiality, (2) informed consent and (3) inclusion of vulnerable groups.
No information identifying participants will be recorded and encrypted voice recording devices will be used to ensure complete anonymity and confidentiality of participants. The audio files will be sent via an encrypted site following the “IARC File Transfer Protocol”. In addition, once transcribed, all audio recordings will be eliminated and transcripts will be stored at IARC local servers, exclusively for the length of the study. This data will be only used for the purpose of the study and will be accessible exclusively by the research team. Information about data management and storage have been added to the Information sheet.
As interviews will be completely anonymous, the informed consent will be provided orally as asking participants to fill in and sign a written informed consent would be contrary to anonymity. Therefore, after providing the Information sheet, at the beginning of the interview, participants will be asked to provide their consent by explaining them the aim of the interview and making sure they know that they can ask any further questions to make an informed decision to participate. They will also be made aware of their entitlement to withdraw at any stage of the interview for whatever reason, to withdraw data just supplied, and/or to not answer specific questions. Their consent is contained in their participation; yet we will ask participants to orally state that they have been informed about the study and that they participate in it voluntarily.
Finally, to ensure inclusion of vulnerable groups, we are using a quota sampling strategy to actively engage low educated groups to ensure voices from the most deprived are also heard. As this community often has low engagement level in qualitative research, in each country a specific recruitment plan has been developed to identify the more adequate channels and settings to find and involve this population and strategies to boost their participation.
Discussion
This study is original because, unlike previous studies, it aims to explore and understand the facilitators and challenges people face when adopting a set of key primary and secondary cancer prevention measures as a package (the 12 recommendations of the ECAC, fourth edition) rather than individual recommendations (e.g., on increasing physical activity). Therefore, this is the first study to assess how the public perceives the ECAC (fourth ed.) recommendations and to identify and map factors influencing their adoption under the framework of the COM-B Model. The advantage of using this model rather than a single theory of behaviour is that several different explanatory components are outlined, allowing us to consider additional or combined potential influences on behaviour. Moreover, this study aims to explore the factors mentioned above across all socio-demographic groups in nine EU MS, allowing for a more comprehensive analysis of the challenges EU citizens face in adopting measures that would reduce their cancer risk or cancer-related death.
However, our aim to reach all socio-demographic groups across the EU has presented challenges in engaging minorities who are often less likely to agree to participate in research studies (Allison et al., 2022). In this study, the population groups that have been more difficult to engage with are men, individuals of older ages, and individuals with low SES or low education levels. Accordingly, to boost participation from these groups, we decided to offer participants financial incentive of a maximum of €30.
We expect our findings will provide insights into how the EU citizens perceive the ECAC fourth edition cancer prevention recommendations and whether they successfully motivate people to change their habits and adopt healthier behaviours. In addition, we expect to identify the main perceived or already met facilitators and barriers related to their capabilities and the opportunities (as described by the COM-B model of behaviour) to adopt these cancer prevention measures. Yet, due to the exploratory nature of this study, further research will be needed to design population-based interventions to lessen identified barriers and foster perceived facilitators for cancer prevention.
This study was conceived as a formative research study to inform the update of the ECAC (fifth edition) by including the findings in the development process of the new recommendations. The pathway for this inclusion will be clearly laid out in the process towards the fifth edition of the ECAC [manuscript currently under preparation]. Consequently, we are confident that our findings will also be important to assist the cancer prevention, health promotion, and education research communities in the design of evidence-based behavioural change interventions. Furthermore, civil society organisations may use our findings to advocate for healthier environments and resilient healthcare systems in the EU that will enable cancer prevention.
Limitations and Strengths of the Study
Our study may have some limitations. A potential limitation of the study is the fact that the fieldwork has been conducted by different researchers in each country as qualitative research is heavily dependent on interviewers’ individual skills and more easily influenced by different personal biases and idiosyncrasies. Yet, to minimise this effect, we ensured that all interviewers had previous experience with qualitative research and provided a topic guideline aimed at guaranteeing interviews were all conducted following the same scheme. Another limitation could be desirability bias that occurs when respondents give answers to questions that they believe will make them look good to interviewers, concealing their true opinions or experiences, and affecting their responses. Despite we recognize this potential bias, researchers’ presence during data gathering in qualitative research is often unavoidable.
Despite these limitations, this study has also strengths. It is—to our knowledge, the first study to explore perceptions to adopting a multi-risk factors cancer prevention educational tool, the ECAC (fourth ed.), using a qualitative approach, which offers a powerful and compelling technique to obtain reliable and transferable data based on human experience. As a result, the complex issues can be understood easily (Shidur Rahman, 2020). In addition, the inclusion of one third of EU MS (9/27), representing all European regions, except for Northern Europe, and with different population sizes and political, economic and social context ensures a broad understanding of the needs of the target audience of the ECAC: EU citizens.
Footnotes
Acknowledgements
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article, and they do not necessarily represent the decisions, policies, or views of the International Agency for Research on Cancer/World Health Organization.
Authors contributions
Conceptualization: AF, CE; Methodology: AF, CE; Investigation: all authors; Resources: AF, CE; Writing – Original Draft: AF; Writing - Review & Editing: all authors; Project administration: AF; Funding acquisition: AF, CE.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has been funded by the Cancer Prevention Europe (CPE) consortium and was additionally supported by the IARC's Environment and Lifestyle Epidemiology Branch budget.
Ethical Statement
Trial Registration
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.