
Abstract
This article examines the influence that digital life stories (DLS) can have on cancer research, using the PARCA1 project as an example. After describing the theoretical framework of DLS, we present the PARCA1 project. The PARCA1 project was anchored in the French context (Grand Est region) and aimed at producing knowledge on patients’ experience of the cancer pathway through DLS. It involved 10 patients chosen to favor heterogeneity in profiles and experiences of illness. The paper describes the digital tool and the life stories methodology used to accompany the DLS. Next, it presents the methods and strategies used by participants to complete their DLS and the relationship between people with cancer and the accompanying researcher. Following this, we present (1) the impact of DLS on people with cancer, i.e., their progressive engagement in research, and (2) the impact on research, i.e., the methodological impact of people with cancer on research. In the discussion and conclusion, we explore how DLS can impact individuals who engage in them and their role in research.
Context
Interest in understanding the experiences of individuals affected by illness has grown significantly over the past half-century (Gualandi et al., 2019; Tourette-Turgis et al., 2019; Pierret, 2003). Narrative research allows for the exploration of an individual’s life and is, therefore, suitable for generating knowledge about the experiences of individuals affected by illness (Clandinin, 2007; Renjith et al., 2021). Narrative research is based on ‘storytelling’ (Renjith et al., 2021). With the term ‘storytelling’, researchers refer to a multitude of narrative forms and data collection procedures (Rieger et al., 2020). In this article, we focus on narrative research based on a specific type of storytelling known as life story and, precisely digital life stories (DLS). Life stories are personal narratives in which a person tells an episode of their own experience to another person (Bertaux, 2016). DLS are life stories facilitated by digital tools, such as applications or online plateforms. The aim of this paper is to explore the impact of engaging in DLS, in terms of both its effects on the person who engages in it and the interaction between the person who engages in the DLS and the researcher who accompanies the DLS. We will describe how the experiences of people engaging in DLS can influence the progression of a research project. We will build our exploration on an ongoing research project based on DLS done with people with cancer.
Life Stories
Life stories are personal narratives in which a person tells an episode of their own experience to another person, either in writing or orally (Bertaux, 2016). The nature of this event may be spontaneous, as seen in personal blogs, or solicited by a reasercher to produce scientif knowledge (Delory-Momberger, 2014; Legrand, 1993). In such case, the researcher ‘asks’ those who know a given context ‘how it works’. Life stories can also have a self-formative effect (Delory-Momberger, 2014; Pineau et Marie-Michèle, 1983): people engaging in life stories do not simply recount their experience but also engage in self-analysis of what happened to them. Life stories enable ‘to emphasize the resources of the person by valuing their power to act (...). This approach takes into account the aspirations of individuals by privileging partnership and multidisciplinarity which are rooted in a bottom-up perspective' (Hardy & Eneau, 2017). They therefore create the conditions for a reflexive return of the persons in regards to their experience, allowing increased awareness of their power to act and to develop an evaluation of themselves, of their capacities to think and act on an individual and collective scale.
Digital Life Stories
Digital life stories (DLS) are life stories told with the support of digital tools, such as applications or online plateforms. DLS originate from digital storytelling, a method developed in the nineties (de Jager et al., 2017; Gubrium, 2009; Hessler & Brooke, 2018; Rieger et al., 2018) which involves creating 3–5 min videos where the storyteller records the story and uses images and sounds to convey messages (Lambert, 2012). Digital storytelling enables people from various backgrounds to share their narratives (Fiddian-Green et al., 2019; Miettinen, 2019; Rieger et al., 2018). Ultimately, digital storytelling refers to any personal narrative created and shared using digital tools, such as digital stories (West et al., 2022), digital narrative medicine (Cenci, 2017; Cenci & Mecarelli, 2020) and digital life stories. A systematic review of digital storytelling in health research highlights that ‘Incorporating digital storytelling in research has resulted in varied impacts on participants, research processes, and knowledge development’ (West et al., 2022, p. 17). This method enables the collection of rich data in innovative ways, while allowing participants to articulate and understand their traumatic experiences (West et al., 2022) and facilitating the expression of patients’ fears and convictions more freely (Cenci, 2017). Topics explored through digital storytelling in the past include mental health, sexual health promotion, refugee health and oncology (West et al., 2022).
In terms of research design, the person engaging in the digital storytelling can chose the digital device – smartphone, tablet or computer – with which they are familiar and comfortable (Cenci, 2017). Digital storytelling can be told through an asynchronous modality and the person telling the story will therefore be able to choose to tell it at the moment that is most suitable for them.
The PARCA1 Project
The PARCA1 project - New care pathways: a qualitative exploration of the experience of people with cancer 1 - was an emerging project aimed at producing knowledge on patients’ experience of the cancer pathway. The pathway approach to patient care has been introduced, in France, by the healthcare legislation (LOI n° 2016-41 du 26 janvier 2016 de modernisation de notre système de santé 2016). It followed the national strategy for cancer care: successive cancer plans (Le Plan cancer 2003–2007, s. d.; Le Plan cancer 2009–2013, s. d.; Le Plan cancer 2014–2019, s. d.) were designed to mobilize public health stakeholders around prevention, screening, organization of the research, support for patients and their families, and post-cancer care. The pathway approach aims to provide comprehensive, structured, and continuous care for patients as close to their homes as possible.
Healthcare pathways are implemented at the regional level by regional health agencies. The Grand Est region, where the PARCA1 project was implemented, has developed 10 pathways, including the ‘Cancer Patients’ pathway. The PARCA1 project was set up within this national and regional context to explore the cancer patient’s experience with care organization by pathway.
The PARCA1 project was led by the collaboration of three researchers in human and social sciences from the University of Lorraine (France), along with a medical oncologist, who are the authors of this paper. The data processing related to the PARCA project has been registered by the Data Protection Officer at the University of Lorraine’s data register.
The PARCA project was structured into several phases: preparation of the DLS production, realization of DLS, and analysis of the data collected through the DLS. After having described the implementation of these phases, we will show how the DLS have impacted the individuals involved in the project and the project itself.
Population
Socio-demographic of Participants.
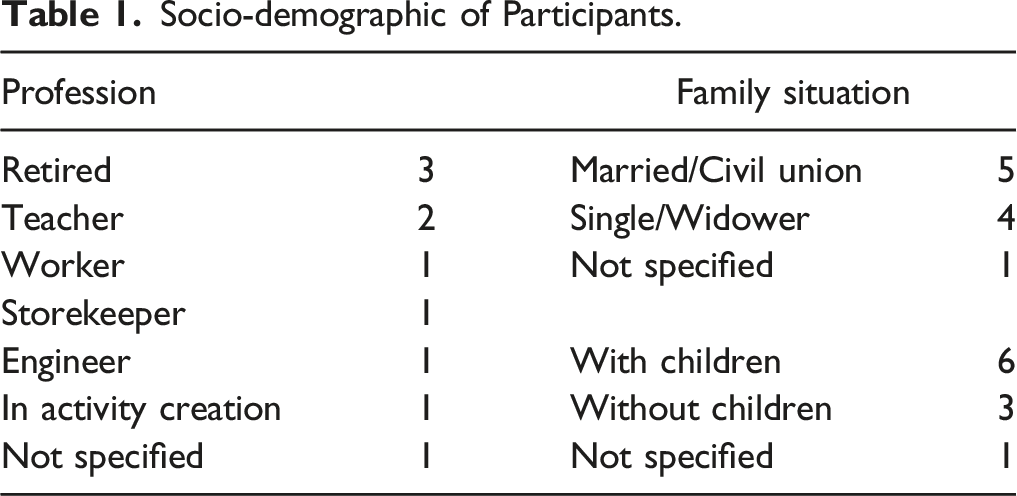
The types of cancer were varied (breast, lung, pancreas cancer) and participants were at different stages of their care journey: one patient was at the beginning of their care pathway, five were in the middle and four were at the end. They were chosen to represent the different treatments commonly used in the field of oncology: surgery, radiotherapy, chemotherapy, immunotherapy, hormone therapy, and innovative treatments (for example, cyberknife).
Seven participants were recruited through the clinical team of the Institute of Cancerology of Lorraine, located near Nancy (Grand Est region, France), and three participants were recruited through the local committee of the League Against Cancer (Comité 54, Grand Est, France). This type of recruitment led to a diversity of profiles by involving patients as well as resource patients. Resource patients are people who have or have had cancer and who wished, after training, to share their experience with patients, relatives and healthcare professionals. In our specific case, resource patients were trained through the national patient partner programn of the League Against Cancer.
Data Generation
Digital Tool
Life stories were told via PandaLab© (https://www.pandalab.fr/), a secure digital platform designed for communication among healthcare professionals and between healthcare professionals and patients. While the platform’s primary purpose is not to collect patient stories, it includes a chat feature that allows users to send messages orally by recording audio or video messages, or in writing by typing or using photos (Figure 1). PandaLab© was selected for its robust data protection measures, ensuring compliance with security standards for processing, storing, and archiving health data, unlike other instant messaging services or email exchanges. Moreover, the PandaLab© manager is a partner in the project, and we had the possibility of using it free of charge. This partnership is disclosed in the conflict of interest section of this paper. The PandaLab© messaging space.
Research participants were introduced to PandaLab© during the inclusion meeting, before signing the consent form. The platform was explained by comparing it to WhatsApp©, and a document detailing the installation and usage of PandaLab© was sent via email to participants. Participants were required to download PandaLab© on their own devices, such as computer, tablet or smartphone. In case of difficulties with downloading or installation, participants could contact the researchers for technical support. A face-to-face or telephone meeting was then arranged to provide technical support. After downloading PandaLab© onto a computer, tablet or smartphone, exchanges between the participants and the researchers took place via PandaLab©. Only the person engaged in the DLS and their accompanying researcher had access to the exchanges. The diagram below summarizes the initial phases of the PARCA1 project (Diagrams 1 and 2). The initial phases of the PARCA1 project. Process of producing DLS.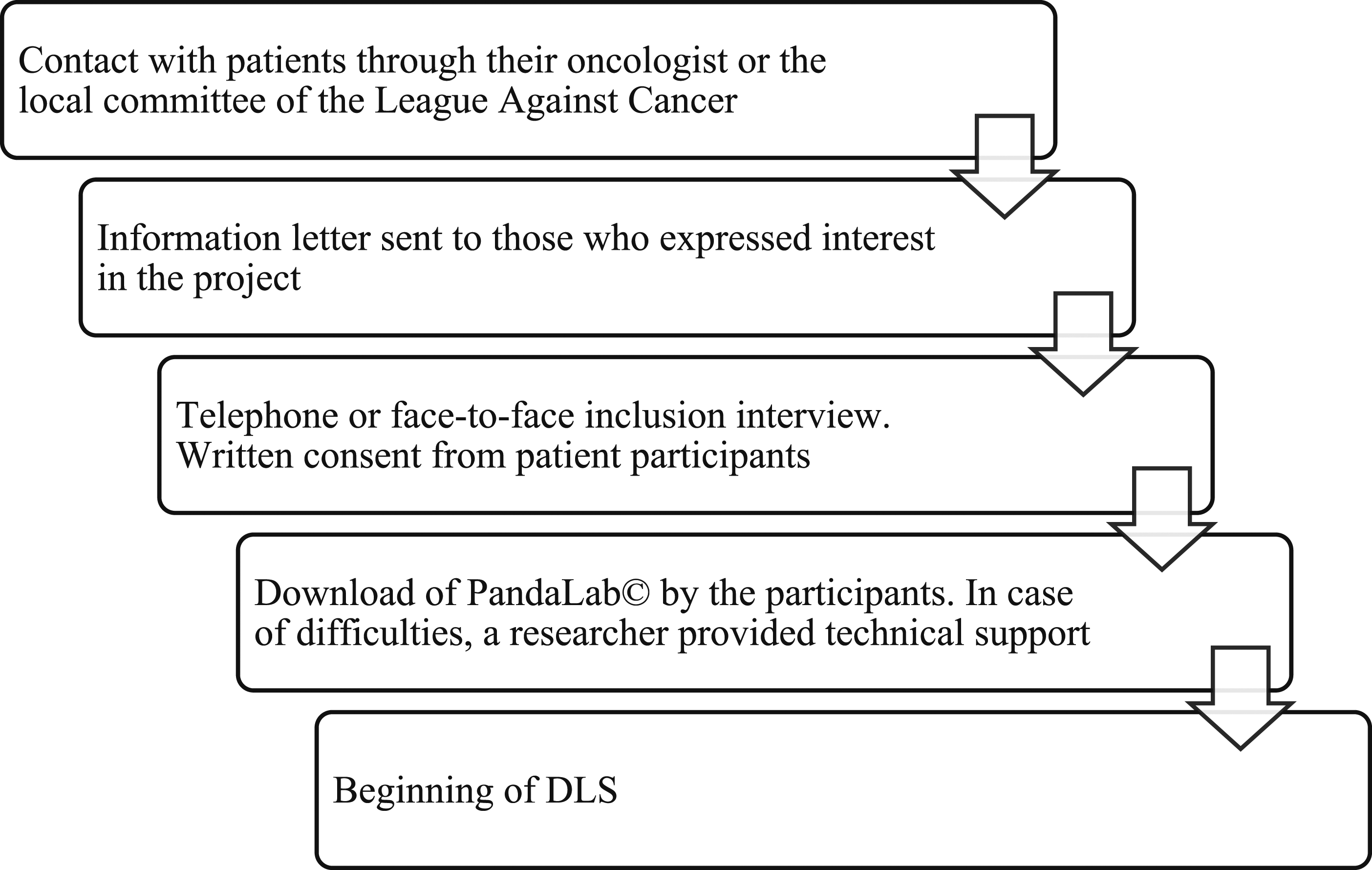

Digital Life Stories Guide
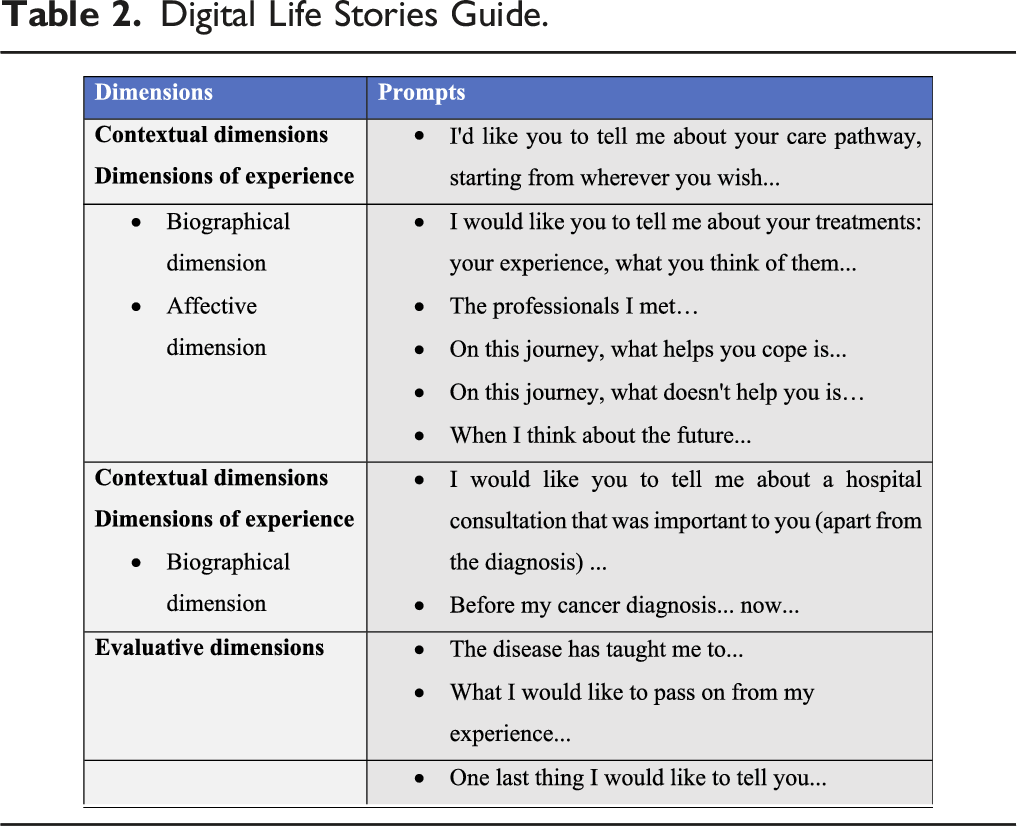
The production of the DLS was guided by narrative prompts (Charon, 2006). Narrative prompts are brief, open-ended invitations to writing. They don’t say what to write or how to write it, or specific points to cover in the writing. To identify our prompts, we relied on Bichi’s methodological proposal (Bichi, 2004). We chose this methodology because it allows us to explore the patients’ experience of the cancer pathway through different dimensions: contextual, experiential, and evaluative.The contextual dimensions help specify the social spheres in which the studied phenomenon is visible - including family, professional spheres, as well as relationships linked to the sociability of the disease, such as contacts with health professionals, other patients, associations, etc. The experiential dimensions were further broken down into affective dimensions (feelings, emotions...) and the biographical journey (first symptoms, diagnosis, treatments...). Finally, the evaluative dimensions concern the retrospective evaluation that the patients made of their care pathway, its interpretation and its evaluation in terms of learning.
Digital Life Stories Guide.

All the DLS were accompanied by the same researcher in human and social science. The prompts were written in the PandaLab© chat, and once people engaged in DLS replied, the researcher evaluated if clarifications were necessary, similar to during a semi-structured interview. The researcher used three questions: ‘Can you tell me more?’, ‘That is to say?’, and ‘For example? ‘, to delve into a particular point, to ask for explanations, or examples. These follow-up questions were sent in writing via PandaLab©.
To adhere to the research calendar, participants were given six months to complete the DLS. Although no specific deadline was set for responding to each prompt, the researcher followed up if there was no contact from participants within two weeks.
Writing DLS
Methods and Strategies from Peopole with Cancer
Nine patients involved in the project completed their life stories and one patient died before their life story began. The first life story started on March 3, 2021 and the last on July 5, 2021. In order to respond to the needs of the PWC 2 engaged in DLS, adaptations in the design study have been made. Only three life stories were completed as planned in fewer than 6 months. Additional time was negotiated between the remaining six participants and the researchers. The longest life story took 10 months and 26 days to complete.
Regarding the data collection tool, eight stories were completed entirely with PandaLab©. One story was half completed with PandaLab© with the other half in a face-to-face interview. The interview was then transcribed by the researchers. The lengths of the life stories varied from 14,697 characters (about 5 pages) to 286,555 characters (about 77 pages).
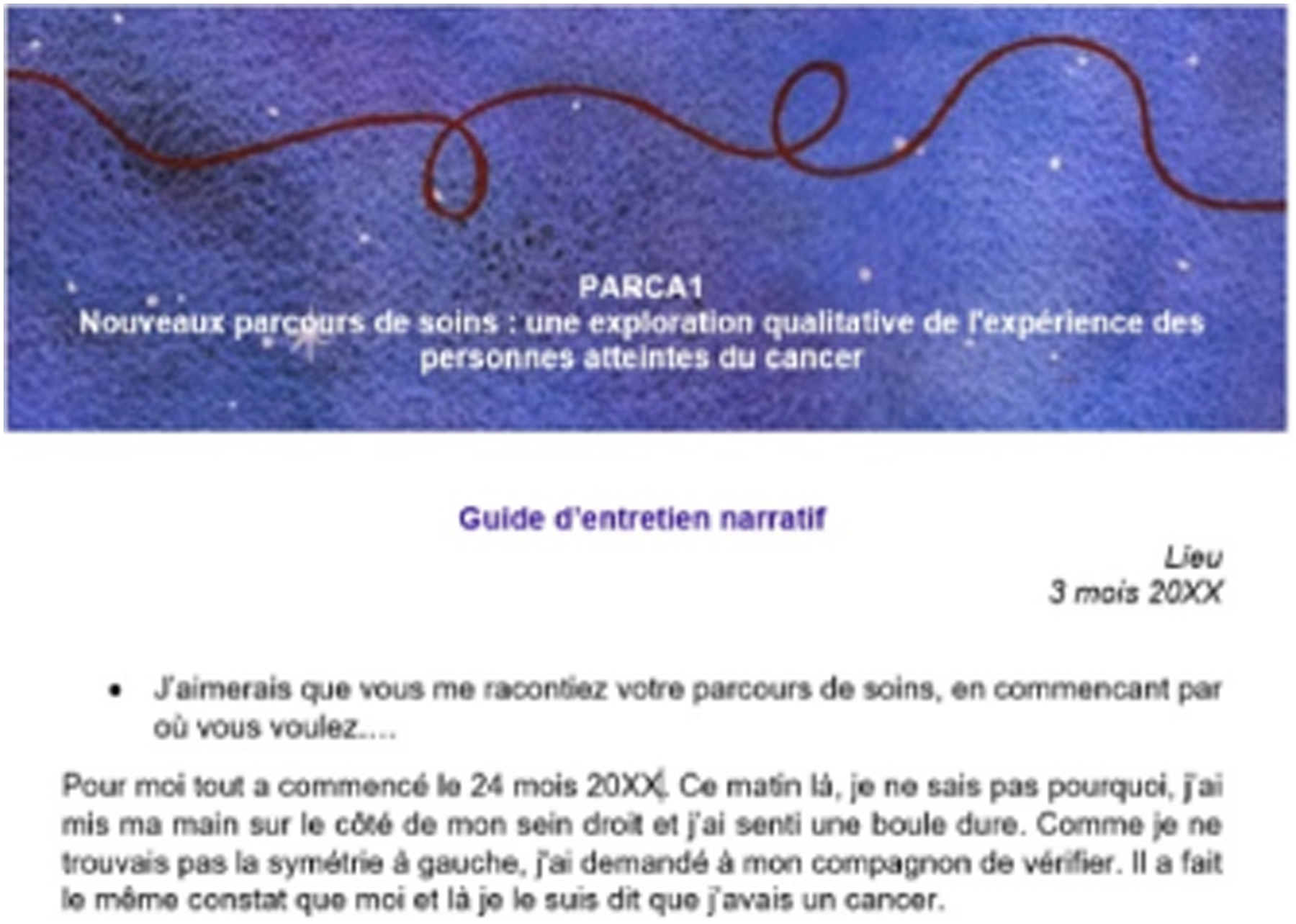
All of the life stories told via PandaLab© were written and transmitted either directly in the chat or as an attachment, in Word or PDF (Figures 2 and 3).
3
The DLS were complemented by photos, documents related to the PWC’S medical journey, or their involvement in community activities, as well as screenshots of Facebook personal pages. The chosen modality was generally maintained throughout the life stories. says: Good morning Madam You ask me what I think of my illness and my treatment, here is what I can say about it. After my examinations, I met the doctor. He was very friendly and seemed to take a great interest in my case and having gathered a lot of information about the evolution of my cancer, he suggested a treatment that was less heavy than chemotherapy. I find this treatment easier to accept, as it allows me to live at home and receive injections from nurses I already know, who are very friendly. says: For me, it all started on Month 24, 20XX. That morning, I don’t know why, I put my hand on the side of my right breast and felt a hard lump. As I couldn’t find the symmetry on the left, I asked my partner to check. He made the same observation as me, and that’s when I told myself I had cancer.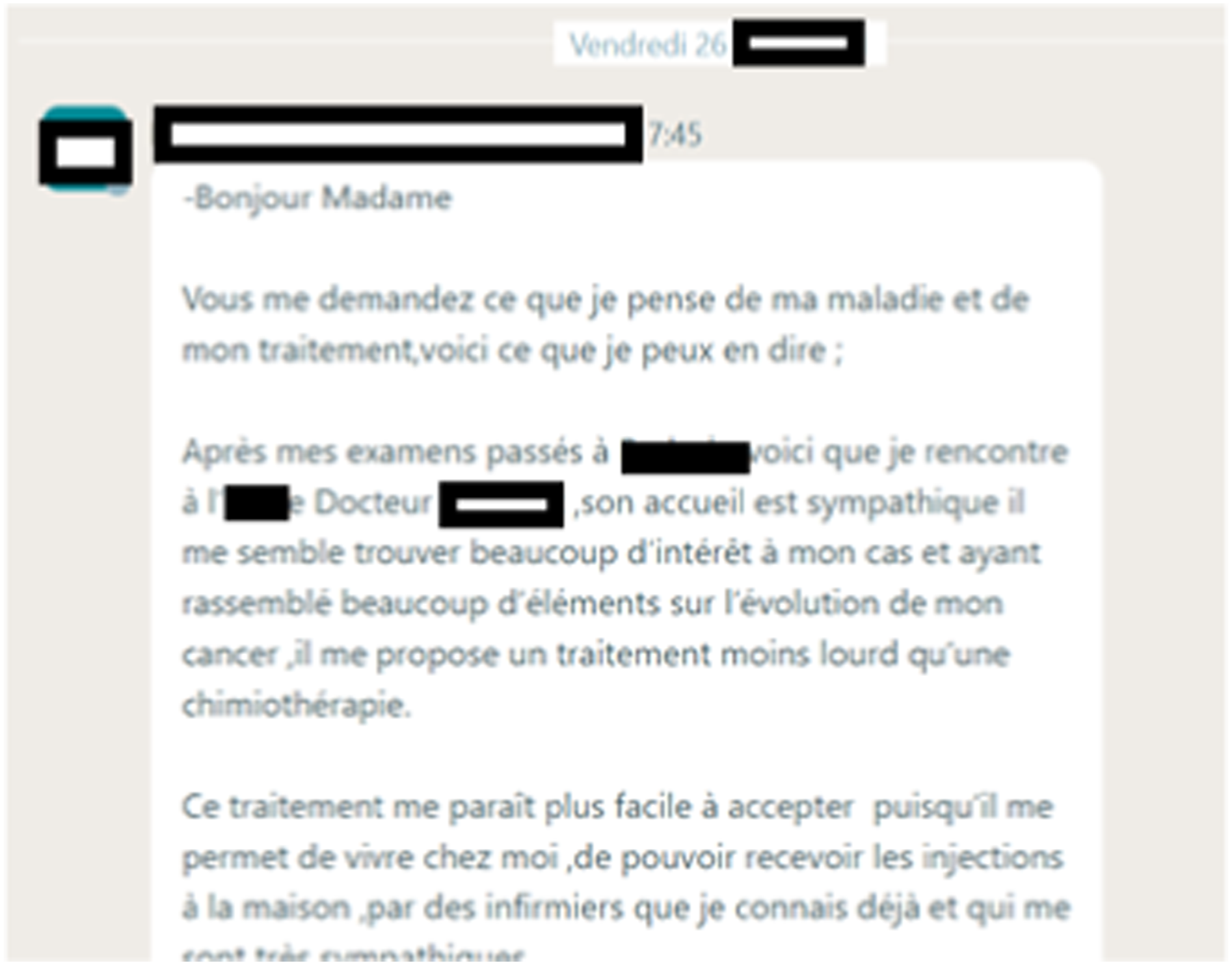
All the participants chose to recount their life stories in writing, but the chosen forms were different. In one case, the response to the first prompt was handwritten, photographed and sent as an attachment. Successive prompts were written directly into PandaLab© (Figure 4). The response to a prompt was handwritten, photographed and sent as an attachment. It says: This morning, as I went to the pharmacy to order my third injection of SOMATULINE, I remembered the stages of my life over more than a year ago!
In another case, the first part of the life story consisted of a table with the dates and locations of medical care described in medical terms (Figure 5). Table showing the stages of medical management. The promt says: I’d like you to tell me about your care pathway, starting from wherever you wish.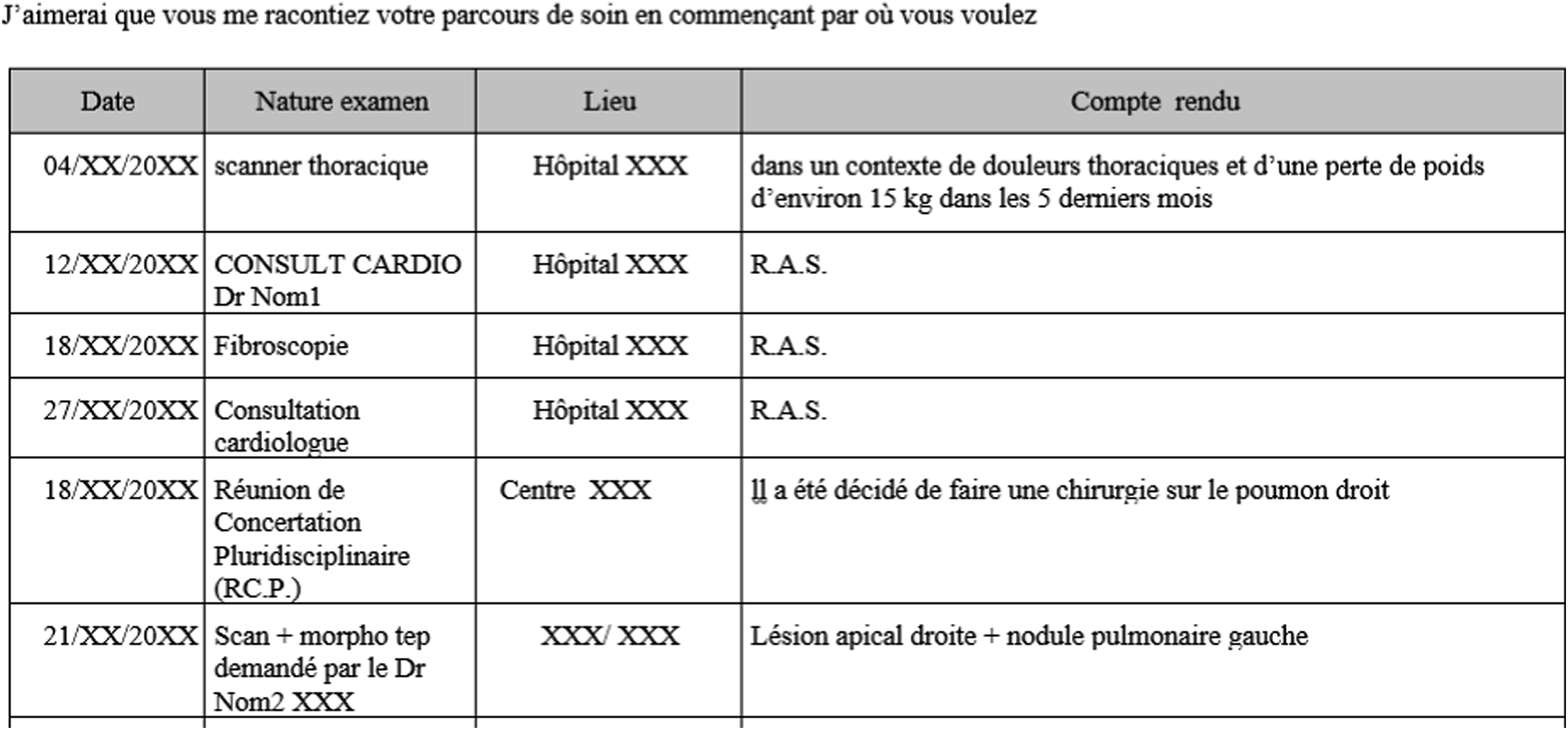
The table indicates the date, type of examination (scanner, cardiological consultation, fibroscopy, etc.), the place where the examination was carried out (name of hospital) and the report (‘in a context of chest pain and weight loss of around 15 kg in the last 15 months’, ‘nothing to report’, etc.)
In another case, the prompt ‘During your care pathway, what helps you cope is... ’ is composed of successive screenshots taken from a Facebook personal page used by the patient to communicate with loved ones about the cancer experience (Figure 6). Screenshots of a private Facebook personal page used by the patient to communicate with loved ones. The first post is an account of a hospitalization for an operation. The patient tells of fasting, showering with betadine, waiting in front of the TV... the patient ends by saying ‘it shouldn’t be long now, I hope’. The following posts refer to the post-operation phase. The patient indicates steps 1 and 2: the removal of the drain and the X-ray that says ‘ok’.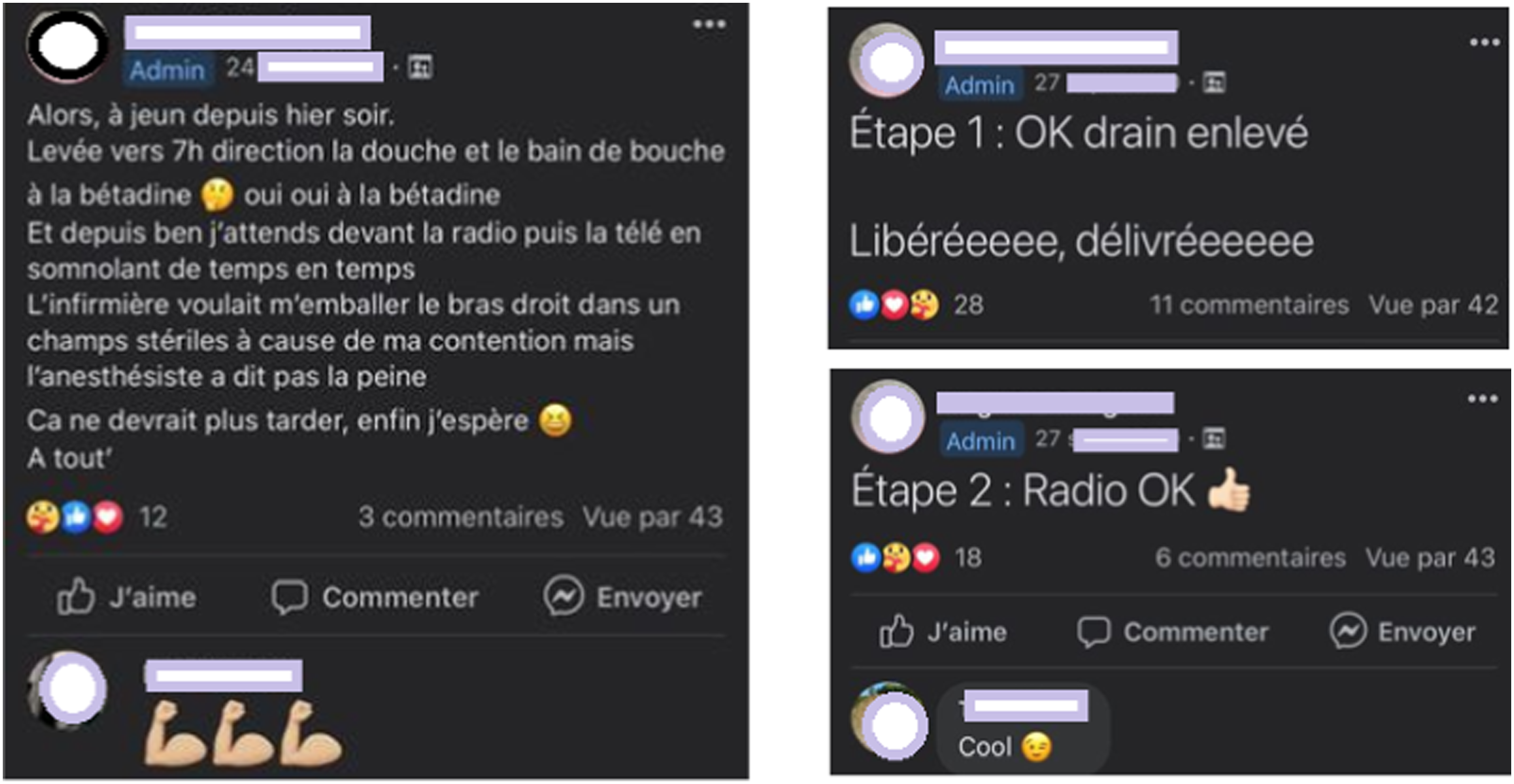
PWC and Researcher: The Beginning of a Relationship?
The time used to complete the life stories ranged from 5 to 10 months. The time between sending a prompt and receiving feedback from participants varied from a few days to several weeks with the pace of writing becoming faster as the deadline approached. In addition, there was a certain routinization regarding the time to write.
Submissions of life stories via PandaLab© sometimes provided additional information about the pace of writing: On Tuesday, I’m going to go to the south coast of France with my son. I am spoiled. I have adorable children! I don’t know if I can reach you via PandaLab©. I will try. If not, I’ll get in touch when I get back
4
(PWC2
5
)
In this case, PWC2 informs the accompanying researcher that their writing pace might slow down during a vacation period. They also add information about the vacation conditions and the sensation it evokes (‘I am spoiled. I have adorable children!’). These unsolicited pieces of information within the research context suggest a shift in the relationship: from patient to researcher, it becomes person-to-person. Hello Silvia, I am finally coming back to you. I apologize for the delay in responding, I started intensive training in sophrology in September which required more personal investment than I foresaw. This is not an excuse but an explanation. (PWC 10) Dear Silvia, I apologize for my long absence. I haven’t forgotten about the study at all, but I’ve had a lot to do and deal with (worries, for one) in my personal life and, as I told you, I wanted to take the time to get it right, so I've put off this essay several times. (PWC 5)
As in the first example, these two messages explain the reasons for taking a break from writing: a busy schedule owing to a career change and personal concerns. These paratexts made it possible to note familiar relationships between patients and the researcher who accompanied them, in particular with the use of first names, rather than family names preceded by the title ‘madam’ or ‘doctor’, as was the case during the inclusion interviews and the first prompts.
This closer relationship between the individual and the researcher, illustrated by a less formal vocabulary, modified the individual’s perception of research and their role within it. Indeed, the DLS led by prompts and requests for clarifications enabled reciprocal socialization (Lyet, 2011; Petit et al., 2022) of patients and researchers to the care pathway and disease. Listening and mutual respect are key to overcoming pre-established roles and establishing a relationship of trust (Houllier et al., 2017). Gradually, participants came to realize that their story was part of the research and that had gone from being informants to contributors. The openness of the prompts, allowing a great deal of free expression, as well as the long response time, encouraged such research contributor position.
As the PARCA1 project was initially designed as a qualitative exploration of the experience of people with cancer, no other involvement of patients was foreseen in the project or its possible follow-ups. However, PWC sharing their life stories for a few months, becoming more familiarized with PandaLab© and more comfortable in personalizing their contributions, acted as a lever for researchers to consider PWC as moving from being just involved to being more engaged in the research. Researchers thought that the participants would be interested in learning more about the results of the research project and would be willing to dedicate some time to provide feedback on their research experience. Consequently, we (the researchers) invited them to a workshop. This step marked the first impact DLS had on the continuation of the project.
Cross-Impacts
On the PWC Side: From Participating to a Restitution Workshop to Taking Part in the Project Follow-up
Eight patients expressed interest in participating to a restitution workshop. The chosen date for the event, February 2, 2022, coincided with a wave of COVID-19 but we could keep the workshop in person, wearing masks and maintaining physical distance. Six patients could attend the workshop. Two patients were unable to attend on the chosen date and they asked to be informed of the progress of the work. The workshop was recorded and transcribed after obtaining consent from all participants. The transcription was sent to them for review.
We structured the workshop in three parts: (1) feedback from the participants on their experience of participating in the study and on the digital tool used; (2) discussion regarding the analysis of the data; (3) discussion regarding the continuation of the project.
The first objctive of the workshop was to collect feedback from the participants on their experience of being involved in the study and on the digital tool used.
First of all, PWC evaluated the use of the PandaLab© tool which they described as ‘handy’ and ‘not bad at all’. To tell the story, four PWC reported writing with a computer, 1 PWC with a tablet, 1 PWC partly with his or her smartphone and partly with their computer. Participants said they needed to be alone and in a quiet place to write. The stories were usually written in a living space (office, kitchen, bedroom or living room) and occasionally in the workplace or in a health professional’s waiting room (two PWC).
Then, PARCA1 participants were able to express themselves regarding the use of life stories. They appreciated the fact that they were given a voice and that the prompts offered them the opportunity to express themselves freely: The prompts you gave were really broad (...) you didn’t set a limit to what we wanted to say. (PWC8) It's good to be able to give patients a voice, how they experienced it, the terms that are used, the hospital world, how they feel about things... and then the principle of the prompt, to be able to respond to it, either with long texts or with short ones, I found that good. (PWC9)
Difficulties were also reported: Overall, I think the study is really well done (...) the prompts are very open-ended which can be a little destabilizing... At first, I said to myself, ‘Well, what are we waiting for?’ And then finally, we let ourselves go. (PWC5)
The time and commitment required were described as barriers to writing: And then the fact that I wanted to do this very seriously, to invest myself. So, that’s why I was backing off and saying, well, I’m going to get my head around. (PWC5)
Patients spontaneously made a proposal for methodological improvement by suggesting that a deadline be given for each prompt. This proposal was considered useful by three other patients who said that they were ‘quickly overwhelmed by other things’ or work or other activities. A deadline would free up time for writing. In contrast, one patient indicated that they preferred not to have a deadline ‘because it’s when you need it that you express yourself, that you can write what you want, what you feel.’
During the workshop, researchers also exchanged on how PWC accomplished their task. Several of them reported needing to return to the notes taken during previous phases of illness, whether they were personal notes (PWC10), shared on a personal Facebook page (PWC4), or notes from a loved one (PWC3). This approach demonstrates both the commitment and the willingness of the PWC to recount an experience that is partly forgotten as comprehensively as possible. This commitment and the process of recalling the illness through writing had both positive and negative effects on individuals engaged in a DLS. Negative effects were linked to the writing exercise described as emotionally difficult (PWC5) or plunging the person writing into a sort of confusion (PWC2). The emotional burden, perhaps that’s why I often put off doing it because it’s heavy, it’s heavy, especially when, for example, you’re told you’ve had recurrence. It took me a long time to do it. (PWC5)
Recalling the illness through writing also had positive effects because of the possibility of taking a reflective look at their pathway: On the one hand, it plunged me back into it, but on the other hand, it gave me time that I hadn't taken to say to myself, here I am in the aftermath (...) it allowed me to see the story at once. I tried not to do that when I was in it because if I looked at it all at once, it was too big. A bit like hiking, if I look at the summit right away, it cuts off my legs. (PWC10)
The second part of the workshop was a discussion regarding the analysis of the data. The three researchers in human and social sciences conducted a triple thematic coding of the collected data. During the workshop, the researchers presented several points of their analyses, particularly regarding the temporality of the care pathway and the articulation of the care pathway with the life journey, and discussed them with the PWC. We will not address this point further: the results of the analysis of digital life stories will be described in another article.
Finally, the third part of the restitution workshop was a discussion regarding the continuation of the project. The researchers asked PWC if they wished to be involved in successive phases of the PARCA1 project. Five PWC responded affirmatively to this proposition and they actively participated in disseminating the results of the PARCA1 project. This collaboration for dissemination took two forms. Four patients collaborated with researchers on designing a website that presents the PARCA project (https://parca.univ-lorraine.fr/). Several online meetings were held during this process. The design of the website was created by PWC and a researcher. The website is now live with content provided by both PWC and researchers. However, the project is currently on hold. As this project was not prioritized, the researcher’s solicitation of PWC was irregular, and the maintenance of the website was slowed down. This situation aligns with Charlebois et al.’s observation that researchers’ ability to support patient involvement proved to be a crucial factor in co-construction (Charlebois et al., 2014). This project will be prioritized and resumed in the coming months.
Another dissemination action is the participation in scientific conferences. Two PWC volunteered for this activity. We started by attending together, PWC and researcher, at local events, such as the seminar ‘Patients and Citizens as Partners in Health Research: What Status?’ in Nancy on November 8, 2022, and eventually reached the international symposium at the 90th Acfas Conference ‘Involving Patient Partners in Cancer Research and Care: Perspectives from France, Quebec, and Belgium' in Montreal, Canada, on May 9, 2023.
Participating in these dissemination events facilitated mutual understanding between PWC and researchers. From the perspective of PWC, gaining a better understanding of the research context, its requirements, and rules, allowed for a demystification and provided them with a sense of legitimacy. From the point of view of the researchers, recognizing the interest of the contribution of PWC’s perspective and their skills has prompted considerations for including them in future research.
On the Research Side: Impact of DLS and PWC Commitments on New Research
The PARCA2 project - Improve the cancer care pathway: an intervention co-constructed by researchers, patients, healthcare professionals and institutional stakeholders6 was a broader research project whose aim was to improve the experience of the cancer care pathway through a participatory intervention. It was led by researchers in human and social sciences and co-constructed with patients, healthcare professionals and institutional stakeholders. The first step of PARCA2 was to explore the healthcare professionals’ experience of cancer pathway. We worked with healthcare professionals in the same way we did with PWC, i.e. using DLS. PWC positive feedback confirmed our intention to use the PandaLab© tool in PARCA2, and the prompts proposed to the healthcare professionals were an adapted version of the ones given to PWC.
The comments regarding the interest of a deadline were incorporated into PARCA2 through the decision to ask each participant if a deadline would help them allocate time to recount their life story and if they desired the researcher to provide it.
These comments, which highlighted the challenges of finding time and the commitment required to participate in the project, along with the experience of the PWC who completed their life story through an interview, convinced us that it would be beneficial to offer participants in the following project, PARCA2 a choice between using DLS or opting for an oral interview.
Methodologically feeding PARCA2 was not an aim of PARCA1 and of the workshop. PWC were initially involved in PARCA1 ‘only' to share their experience of the cancer pathway. The relationship created through the project made this additional contribution possible, which had a significant impact on the design of PARCA2 (Diagram 3). The diagram below summarizes impact of PWC feedback on PARCA1 and 2.
Discussion
The Interest of DLS for PWC
In the PARCA1 project, researchers explored the cancer patient’s experience with care organization by pathway. They employed life stories to gain insight into the experiences of PWC to generate scientific knowledge. However, scientific literature shows that life stories serve a dual purpose: contrubuting to scientific knoledge and enabling those who share them to engage in self-analysis, recognize their agency, and develop self-evaluation (Delory-Momberger, 2014; Legrand, 1993; Pineau & Marie-Michèle, 1983). These two approaches are complementary rather than mutually exclusive endeavors.
In this project, life stories are a self-formative process: the restitution workshop has highlighted that DLS enabled patients to become aware of what has happened to them, of what they have been through and helped them make sense of their experiences. This self-awareness allows PWC to understand the interest of their experience for research and put them in a position to choose to engage more in research projects.
New role in Research: Toward Participative Research
In PARCA1, the involvement of PWC was not limited to their identity as patients and the stereotypes that could be associated with it: they participated in research as a whole person, not just as patients. Over time, collaboration and information sharing between researchers and patients were established, leading to the exploration of new forms of working together. PARCA1 allowed to start a co-construction process that continued in PARCA2 and had driven reseracher to imagine other forms of collaboration in the continuation of the project.
This process continues with the project Improving the cancer care pathway through partnerships between patients and healthcare professionals: from multi-site experimentation to interventional research (4P). 7 4P pursues the scientific objectives begun in the PARCA projects, i.e. proposing improvements in cancer care pathways through a multi-centre intervention.
From the beginning of the 4P project, the researchers included PWC in the project management. A research consortium was established, bringing together researchers, PWC, and healthcare professionals. The purpose of this research consortium is to guide and to contribute to the development of the research. Two of the PWC who participated in the PARCA1 project have joined the research consortium of the 4P project. These two PWC are among the participants who participated in the restitution workshop and are involved in the dissemination of the results. Therefore, we observe a progression in patients’ involvement in the research projec: from data production and providing feedback on the research design in PARCA1 to actively engaging in a steering committee in 4P (Diagram 4). The diagram below summarizes the evolution of the engagement of PWC in research.
Conclusion
The PARCA1 project was an exploratory research aimed at gaining a deeper understanding of the experiences of individuals living with cancer. In alignment with this objective, we opted for a narrative methodology based on DLS. Throughout our research, patients’ roles evolved from recounting their illness experiences to a more active involvement in the PARCA1 project and its subsequent phases and an intervention research project co-constructed with PARCA participants (4P project) is underway.
Patient engagement is highly suitable. The involvement of the players with expertise other than scientific has demonstrated its interest (Charlebois et al., 2014; Flora, 2013; Howe et al., 2017), but the involvement of the populations concerned has often been limited (Charlebois et al., 2014; Ives et al., 2013).
While digital storytelling has been acknowledged as an emerging method in participatory health research (Rieger et al., 2018; Sitter et al., 2020; Wilson et al., 2015), no research has yet delved into the specificities of DLS and its impact on participatory health research. Existing evidence primarily focuses on digital storytelling as a method to capture and share participants’ lived experiences (Rieger et al., 2018) or used as a narrative intervention in health promotion, for exemple, to increase socioemotiona well-being and bolster positive health outcomes (Fiddian-Green et al., 2019). The structure of DLS, their temporality, and the relationship developed with accompanying researchers distinguish DLS from other forms of storytelling. This not only broadens the utility of sharing experiences but also enables them to elevate engagement to a higher level on the continuum. As illustrated by the PARCA1 project and its follow-up, DLS is a method that can foster participatory research (Ligue contre le cancer, sd).
Footnotes
Acknowledgments
The authors wish to thank participants who so generously shared their time and energy. We also wish to thank organizations that supported recruitment, including La Ligue contre le cancer (Comité 54, Meurthe et Moselle, Grand Est, France), the NEON-NEtwork ONcologie- network, the URPS Pharmaciens du Grand Est and the URPS Masseurs-Kinésithérapeutes du Grand Est.
Author Contributions
All the authors contributed to conception or design of the project. S.R. drafted the manuscript. F.C., A.L., J.K. critically revised the manuscript. All the authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Aurélien Lambert, co-author of the article, is manager of PandaLab©; PandaLab© has been made available free of charge.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cancéropôle Est, Strasbourg, France [Emergence, 2020] and the INCa, Paris, France [RISP-21-008, 2020].
Ethical Statement
Data Availability Statement
Anonymised narratives and interview transcripts from participants who consented to data sharing, plus other supporting information, are available from the University of Lorraine’s Data Service.