
Abstract
Informed consent is essential in research involving people with disabilities to protect their rights and ensure ethical conduct. Individuals with communicative vulnerability, such as those living with deafblindness, face difficulties when the research process is not accessible. Our team has developed methodological expertise where this vulnerable population is concerned. To formalize recommendations that can improve their inclusion, we utilized an observational, retrospective design to address three questions: What are procedures that facilitate recruitment in a lab specializing on working with individuals living with deafblindness? What are optimal procedural adaptations to obtaining informed consent? and What training can best prepare researchers working with individuals living with deafblindness? First, we conducted a textual narrative synthesis of our eight most recent protocols and procedures that required in-person interaction with adults living with deafblindness. Second, we conducted semi-structured discussions among our team members, and third, we engaged in a validation procedure of the synthesized recommendations with our external partners. Procedural adaptations require flexibility in all aspects of recruitment and consent to accommodate communication needs. These include additional time, and accessible formats. Adaptations should consider vision (e.g., large-print, braille) and hearing (e.g., sign language, communication strategies) as well as aspects unique to deafblindness (e.g., intervener support, tactile communication). Consent can be documented in hand-written, electronic, audio or video-recorded format, and may be facilitated by third parties. Team training should include proficiency in plain language, basic knowledge about deafblindness, and awareness of accessibility features for mainstream devices. We present simple steps that can improve inclusion and increase accessibility for participants living with deafblindness, and that can improve the capacity of the research team by developing flexibility, patience, respect, and trust. This information can further inform institutional ethics review boards that are unfamiliar with the logistics of obtaining informed consent when working with participants living with deafblindness.
Keywords
Informed consent is a critical ethical principle in research involving human participants that is rooted in documents such as the Declaration of Helsinki (World Medical Association, 2023). It refers to the process through which individuals are fully informed about the nature and purpose of a research study before they decide whether to participate or not. This process is important for a variety of reasons, including respecting the autonomy of individuals to make their own decisions, thereby reducing the possibility of coercion; protecting participants' rights and welfare by making them aware of the potential risks and benefits associated with the research; ensuring transparency and accountability to foster trust between researchers and participants; and ensuring compliance with ethical and legal standards for the protection of all parties involved (Nijhawan et al., 2013). Efforts to balance and clarify the ethical and legal interpretation and definitions of consent are ongoing (Moulton et al., 2013); however, while these efforts are focused on what makes consent informed, additional challenges exist in the process of administration and obtaining consent, especially in the context of persons that are considered vulnerable (Gordon, 2020).
The most common standard of informed research consent is the participant’s signature on a consent form that was approved by an institutional review board. It should be provided in an accessible level of language complexity, whereby the participant has taken the time to read its content, has had the opportunity to ask clarification questions, and has the cognitive capacity to comprehend its content and implications. In the case of individuals that present with communicative vulnerability (Gordon, 2020), such as those with sensory impairments or those that use a tactile or signed language, difficulties start emerging when any one aspect of this process is not feasible for, or accessible to, the potential participant. This is the case for persons living with sensory disabilities that interfere with visibility and/or audibility of any information or materials that are part of the consent process.
The Nordic Definition of deafblindness is widely accepted and best summarizes its distinct functional implications (Centre for Welfare and Social Issues, 2016). It highlights how the combined impairments of vision and hearing limit an individual’s ability to be active and participate in society, thereby making it necessary to provide adaptations and services, environmental adjustments and/or assistive technology and devices to overcome these limitations. The barriers to communication and to access information that are experienced by persons living with deafblindness have been extensively documented. For those born with congenital deafblindness, these challenges are often rooted in language acquisition and literacy (Bruce et al., 2016); for those living with acquired or adult-onset deafblindness, communication adaptations are often required, such as the acquisition of new communication techniques (Hersh, 2013); finally, for older adults that develop age-related impairments in vision and hearing, their ability to rely on audio-visual aspects of communication must be supported by assistive technologies, environmental and inter-personal adaptations to restore receptive and expressive communication abilities (Saunders & Echt, 2011). All these variables can make it challenging to explain a research study and obtain informed written consent.
To overcome these challenges, however, researchers have taken steps to ensure that the informed consent process is accessible, understandable, and free from coercion. For example, a recent eBook (Janssen et al., 2021) on the development and wellbeing of individuals living with deafblindness provides an intriguing example of the variability to how consent is not only obtained, but also how this process can be reported by researchers that specialize in this field. As would be appropriate for children or individuals with reduced cognitive abilities, some studied involved legal representatives or next-of-kin to provide consent (Damen et al., 2021; de Vaan et al., 2020; Peltokorpi et al., 2020; Wolthuis et al., 2020). Several studies reported that informed written consent was obtained from deafblind participants, but the authors did not provide any details on how this was accomplished (Wahlqvist et al., 2020b; Wanka, 2020). The presentation of such procedural information would have been especially informative in a study that focused on participants that used signed or tactile communication techniques (Gabarró-López & Mesch, 2020). Some authors provided limited information related to the consent process, such as the provision of a comprehensive information letter (Vreeken et al., 2020), or written and spoken information and the opportunity to ask questions (Jaiswal et al., 2020c; Wahlqvist et al., 2020a). In contrast, some authors provided detailed aspects of the information and consent process, including the availability of information materials in preferred accessible formats, such as braille and print, in advance, and in-person direct communication with participants to provide informed approval to participate (Jaiswal et al., 2020a; Raanes, 2020). One study included an exemplary online appendix with details on the consent process, all available formats and features (e.g., font size and paper color) as well as the provision of signature guides and high contrast black pens (Parker et al., 2020).
Even though the need for such accommodations and adaptations for persons living with a disability during consent are generally recognized (The Adult Advocacy Centers, 2020), the details of what format these adaptations could or should take often remain elusive. This is especially the case when the potential participant is affected by a unique and complex condition, such as deafblindness. Individuals with deafblindness themselves have called for more accessibility and inclusion in research (Watharow & Wayland, 2022), and have specifically pointed out that the process of informed consent poses an important barrier to participation and patient engagement (Skilton et al., 2018). Given that our research group has developed extensive expertise in working with this population, including the process of recruitment, and obtaining informed consent, we decided to ask the following questions: (1) What are our procedures that facilitate optimal research recruitment in a lab specializing on working with individuals living with deafblindness? (2) What are the adaptations to the procedure of obtaining informed consent that are used by members of our group? and (3) What type of training do we recommend to research staff and trainees, to properly prepare them for conducting research with individuals living with deafblindness?
Methods
Research involving persons living with deafblindness remains relatively infrequent, in part due to intuitive barriers to recruitment and communication (Jaiswal et al., 2020a). Their lack of representation has previously been pointed out in research on assistive devices designed to overcome combined functional limitations of vision and hearing (Wittich et al., 2021). Lack of inclusion and representation is also apparent in the development of research design (Roy et al., 2020), and in the limited research conducted using co-creation (Dyzel et al., 2020; Watharow & Wayland, 2022). Through local, national, and international collaborations with specialists in the field of deafblindness and with persons with lived experience, our research team has been able to develop extensive expertise in aspects of methodology where participants living with deafblindness are concerned (Jaiswal et al., 2020a). Therefore, we utilized an observational, retrospective study design with three methodological approaches to address our research questions.
Characteristics of Participants Living With Deafblindness.
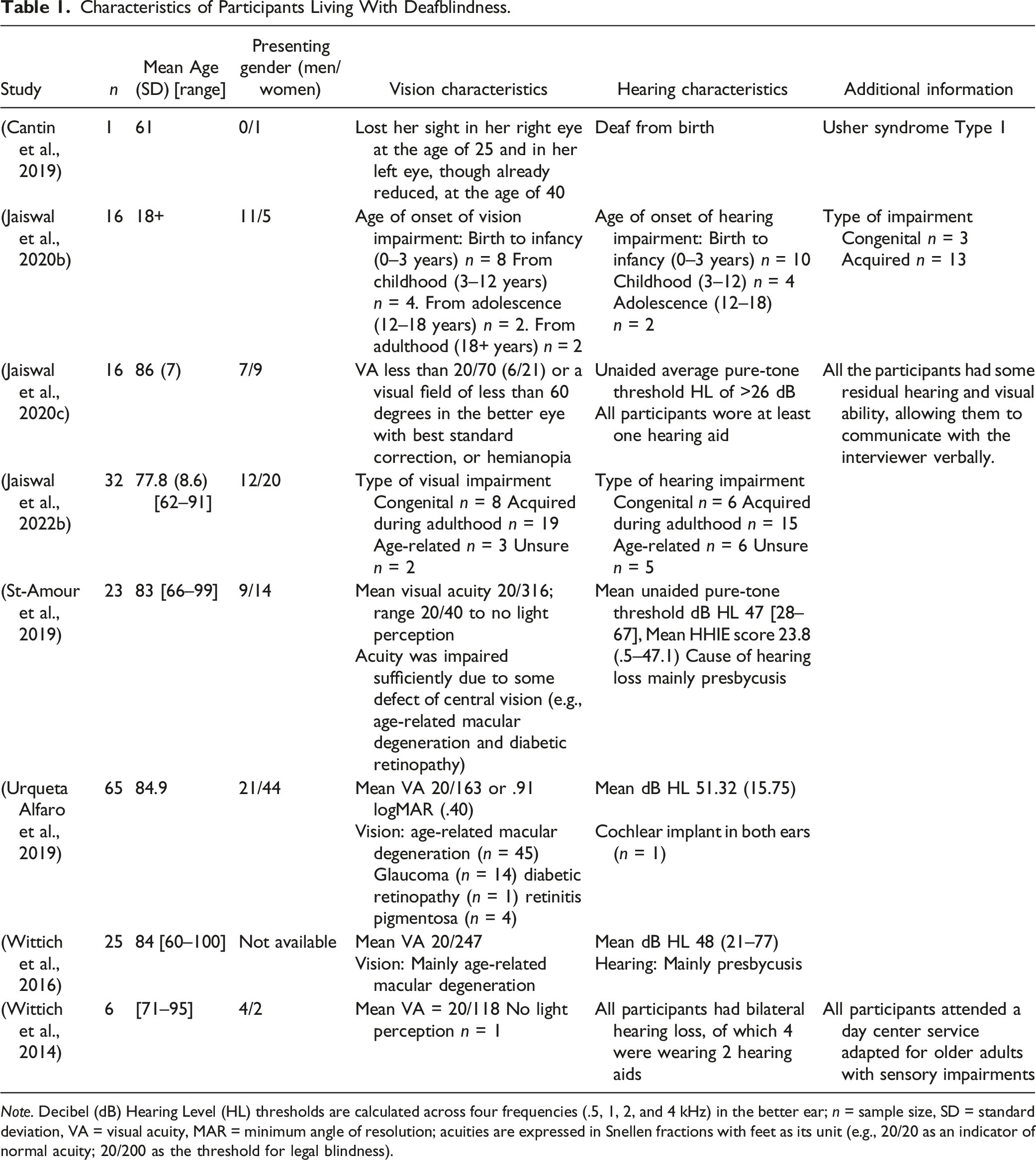
Note. Decibel (dB) Hearing Level (HL) thresholds are calculated across four frequencies (.5, 1, 2, and 4 kHz) in the better ear; n = sample size, SD = standard deviation, VA = visual acuity, MAR = minimum angle of resolution; acuities are expressed in Snellen fractions with feet as its unit (e.g., 20/20 as an indicator of normal acuity; 20/200 as the threshold for legal blindness).
Second, we engaged in semi-structured discussions among our team members to identify priority topics for successful recruitment and consent procedures when working with persons living with deafblindness. These discussions included the lead researcher who has conducted investigations on deafblindness for the past 13 years, a post-doctoral fellow whose PhD and post-doctoral work both focused on deafblindness, a post-doctoral fellow who lives with blindness and is an accessibility expert, and a research assistant who has conducted qualitative interviews (remotely as well as in person) with over 30 participants with various levels of deafblindness. In addition, the team consulted with its two PhD and six master’s students, all of whom have been involved in relevant methodological aspects of conducting research with individuals living with deafblindness. These discussions included reflections on training and practical skill development for novices in the field.
Finally, we engaged in a validation procedure of the synthesized results. We presented the content of Figure 1 and Table 2 to representatives of two of our external partners that provide services to individuals living with deafblindness. Their feedback was incorporated into the results presented here. In addition, we increased the rigor of our study by engaging our team members in reflexivity, individually and as a group (Barry et al., 1999). Reflexivity is an important component of this analysis process because all members of the team have extensive and often personal experience with individuals living with deafblindness; therefore, while maximizing on our topic expertise, we provide content checking for each other when interpreting and summarizing the available information (Olmos-Vega et al., 2022). This overview describes the process of obtaining informed consent from adults living with deafblindness. Additional details describing each step are provided in the results section. The process requires collaboration among the members of the research team, staff of community partners and rehabilitation centers, persons living with deafblindness as well as their trusted family members, friends and/or communication facilitators, such as interveners or sign language interpreters. Adaptations for the Consent Process With Persons Living With Deafblindness.

Results
To answer the question ‘What are our procedures that facilitate optimal research recruitment in a lab specializing on working with individuals living with deafblindness?’ we pooled information that emerged from the textual narrative synthesis as well as the practical experience of our team and feedback from our external partners. The flow chart in Figure 1 provides an overview of the steps leading to obtaining informed consent involving any research participant living with deafblindness. (1) The research team initiates the recruitment process by providing the community partner (e.g., a rehabilitation centre) with eligibility criteria for the study. Such collaborations with organizations that work with and for persons with deafblindness provide access to the population of interest, open the door to co-creation, and facilitate opportunities for knowledge translation once the studies are completed (Wittich et al., 2022). (2) These criteria are used by the archives, admission services or program managers to internally generate a list of potential participants. (3) The initial contact with the person living with deafblindness is then made by a representative of the community partner, such as a research coordinator (Kengne Talla et al., 2023). This initial contact may be direct with the person living with deafblindness, if communication preferences allow for such an approach, or may be facilitated by members of the family, or a professional (e.g., intervener, interpreter). The person living with deafblindness, or his/her representative, can pose questions, and (4) a decision is reached whether there is preliminary interest in knowing more about the project. The person living with deafblindness gives permission to the community partner (5) to share their contact information and communication instructions with the research team.
It is worth noting in this context that the research team does not have access to, and is not directly involved in, the communications that occur between steps (2) to (5) because of confidentiality regulations and laws around access to medical and personal information. Therefore, the research team and the community partner want to develop a relationship of trust and communication that can bridge these steps. Researchers may find that this recruitment process takes more time than what they are used to in other circumstances, and they need to trust that this process is diligently pursued by the partners, given the unique communication needs and administrative realities of organizations that serve persons living with deafblindness.
Once the contact information of potential participants has been received by the research team, (6) a trained research assistant contacts the person living with deafblindness and/or their communication facilitator to explain the project in more detail, and what participation implies specifically. (7) Should the person living with deafblindness choose to participate, the process of obtaining consent begins (see approaches and adaptations in Table 2). This is also an appropriate time to explore participant’s preferred mode of access to information and communication and create strategies tailored to facilitate their autonomy in the consent process. Once consent is obtained, (8) the research team may be asked to inform the community partner which clients decided to become part of the research project, for internal statistical reasons.
Similarly, the synthesis to answer the second question ‘What are the adaptations to the procedure of obtaining informed consent that are used by members of our group?’ relied on integrated information from our three methodological approaches. Table 2 provides a detailed overview of actions that can be taken by members of the research team to facilitate the consent process with persons living with deafblindness. The aspects of adapting the consent process that emerged from the data were chronologically separated. First, procedural adaptations need to be considered by the research team before first contact with a potential participant. These include adaptations that may be necessary when planning interactions with potential participants, such as allowing for additional time, or for the inclusion of other individuals that will facilitate communication. Please note that confidentiality needs to be addressed in such cases, whereby these additional individuals are required to sign separate consent forms, and they become participants in the research themselves. In the case of paid communication facilitators (e.g., interpreters) they are additionally bound by their professional standards of ethics. Second, preparations need to be considered during obtaining informed consent when making the content of the consent form itself accessible. The research team needs to be ready to prepare a variety of adapted documents that adhere to accessibility formats, including braille, large print, but also content adaptations and simplifications that may be required for signed or tactile interactions (e.g., video-recorded version of content in sign language or availability of Protactile interpreters). Providing a multitude of electronic formats has the advantage that such formats give participants access to utilize their own physical or electronical magnification or amplification, screen reader, or electronic braille devices at home. It also allows individuals living with deafblindness to combine accessible formats for their preferred interaction with the content. Finally, we summarized consent format options that can be considered when recording or obtaining consent. Table 2 includes a list of consent formats, in addition to the traditional signature on paper, that can be considered as acceptable by institutional ethics review boards, if storage of this information is encrypted, password protected and/or stored separately from any data that are collected at the same time.
The final question asked, ‘What type of training do we recommend to research staff and trainees, to properly prepare them for conducting research with individuals living with deafblindness?’. As is often the case in research, a senior researcher (whose focus is not deafblind research) may have some knowledge and motivation to conduct a project that includes people living with deafblindness; however, most of the time most of the direct contact with participants will fall to research assistants and graduate students who complete the hands-on work of obtaining consent and data collection. Therefore, it is important to consider what type of training is recommended to research staff and trainees to properly prepare them for this experience. Based on our practice in the lab with novice students and research assistants, our interactions with experienced and new staff members at the partner sites, and the teaching experience of the team leaders, the data synthesis indicated that an elementary understanding of deafblindness, the use of plain language, as well as familiarity with basic communication strategies, accessibility skills, and knowledge of mainstream technology communication features are a good starting point for training a competent team.
Elementary Understanding of Deafblindness
The heterogeneity of individuals living with deafblindness makes it a challenge even for specialists to understand this population. However, some essential information about the assessment of vision and hearing difficulties, as well as their functional implications should be known to everyone who interacts with persons living with deafblindness. Various sources can provide a starting point to learn about this population (e.g., Wittich et al., 2012; Wittich & Simcock, 2019), and we suggest spending time volunteering in a local rehabilitation center that provides services to the type of individuals that are of interest for the research team.
Using Plain Language
The research community is notorious for utilizing language complexity that is inaccessible for research participants, specifically during the consent process (Jefford & Moore, 2008). Therefore, the use of plain language is recommended, especially for communications where literacy and education levels of the participants may not necessarily be comparable to the general population (Green et al., 2003); its purpose is to make communication more accessible and understandable for a wider audience. Plain language involves using clear and concise language, avoiding technical jargon and unnecessary complexity, and organizing information in a logical way. This skill becomes especially important when information needs to be interpreted into a visual or tactile language.
Basic Communication Strategies
When interacting with persons that are hard of hearing, some simple and basic communication guidelines can greatly facilitate verbal communication. Rooted in the concepts of aural rehabilitation (Boothroyd, 2007), communication can benefit from simple strategies such as reducing environmental noise, engaging in clear speech, facing the listener while speaking, providing context at the start of communicating, and taking the time to explain information in plain language. The provision of a personalized amplification device with binaural over-the-ear headphones can easily provide on-the-spot amplification when needed.
Accessibility Skills & Knowledge of Communication Features
While it is not reasonable to ask a research assistant to produce a consent form written in braille, the ability to generate an accessible Word document is within reach. Therefore, we encourage research staff and trainees to explore online resources that provide a basic overview of accessibility features for software (e.g., how to make a consent form as a Word document accessible to screen readers) or how to save existing documents in alternative formats (also see Table 2). Over time, a research team can build a list of external resources and partners with the necessary expertise, such as local braille providers, agencies for sign language interpreters, and rehabilitation centres that specialize in working with and for persons living with deafblindness. In addition, the recent development of remote communication tools, such as Zoom and Teams, have greatly facilitated communication; therefore, students and research assistants should be familiar with how to activate automated captioning features, link communication facilitators that provide transcription services, or how to give sign language interpreters control of pining their camera image so participants can view them as a larger image during a group call.
Discussion
The purpose of the present study was to synthesize and present concrete information about the process of obtaining informed consent when recruiting participants living with any severity or form of deafblindness. The resulting recommendations are based on the practical experience of a team of researchers that specializes in research that includes in-person interaction with persons living with any type and severity of deafblindness. The intuitive communication barriers that researchers face when interacting with this marginalized population are likely part of the reason why the number of studies with deafblind participants remains comparatively small, and why representation of persons living with deafblindness in research is even rarer. While it cannot be expected that researchers in general have the knowledge and skills to make all their protocols accessible to persons living with deafblindness, there are some simple steps that can be taken to improve inclusion. In the examples of the studies whose procedures were reviewed here, it has been our qualitative observation that these approaches and adaptations improved the quality of the experience of our participants, while increasing the capacity of our team by developing skills centered around flexibility, patience, respect, and trust. It has also been our experience that this approach improved communication and empathy, while facilitating equity, diversity, and inclusion in research through accessibility.
Researchers in any domain more easily take the logical step to provide auditory and tactile information to a blind participant, or to offer written or signed instructions to a Deaf individual. Interacting with persons living with deafblindness however is less intuitive and may scare researchers away or overwhelm them. When considering sensory variables in research, adaptations for a single impairment (vision OR hearing loss) are more widely known, more familiar to researchers outside the sensory field, and often more available or accessible. Accommodations for one impairment can then rely on the availability of the other sense for compensating during interactions. For example, standardized screening measures for cognitive functioning of adults, such as the Montreal Cognitive Assessment/MoCA (Nasreddine et al., 2005) have been adapted and validated in versions that do not require vision (Wittich et al., 2010) or hearing (Lin et al., 2017). Even though there are tactile formats of measuring cognition (Bruhn & Dammeyer, 2018; Papagno et al., 2017), a tactile version of the MoCA that would be accessible to individuals living with deafblindness does not currently exist. Even once developed, the process of validating such a test will require substantial resources, necessitating a priority and cost-benefit analysis to justify such an investment.
There is, however, much to be gained by making research participation more accessible and inclusive for marginalized populations, such as persons living with deafblindness. Selection bias may lead researchers to come to conclusions that do not extend to individuals that are commonly excluded from research recruitment and study design, simply because the protocols cannot be administered in a standardized format. Therefore, a large body of work that includes persons living with deafblindness is qualitative in nature, making this the approach of choice for inclusion. Interestingly, qualitative methods have demonstrated to be very flexible and adaptive to the presence of deafblindness, at times in surprising ways. For example, Jaiswal and colleagues (2020) conducted in-depth semi-structured interviews with participants living with deafblindness in India using social media software. Given the heterogeneity of the participants and their communication abilities and styles, the team utilized Facebook Messenger or Skype (without video) with some of the participants as the optimal low-cost and accessible communication technology. The team relied on some of these technologies during the process of obtaining consent as well. Another remarkable example is presented by Arndt (2011) who explored the intricacies of video-recording and transcribing qualitative interviews that were conducted with college students living with deafblindness. She describes how her expertise as sign language interpreter who is fluent in American Sign Language allowed her direct access to the signed information of her participants. This ability required her to then navigate between hearing and Deaf culture during transcription, a process that she describes with intricate attention to detail.
A recent scoping review of consent, assent, and dissent strategies for research participation by individuals living with complex communication needs presented a summary of techniques that are specifically useful when working with children and young adults (Paramasivam et al., 2021). The authors reviewed work that included magnified pictograms during the consent process that are specifically useful in cases where language and/or cognitive development of potential participants was impaired or delayed. Importantly, relationship building and communication training on the part of members of the research team were mentioned as priority steps to making the research experience a success for all involved. Such an approach may take some additional time but is key to determining the most positive and effective strategies to communication and interaction, thereby likely resulting in high quality data. Researchers do, however, need to invest time and effort into becoming familiar with accessibility requirements and a rudimentary understanding of assistive technology and adaptive strategies. Many of the concepts of universal design (Story, 1998) will become useful tools above and beyond use in studies involving persons living with deafblindness.
Our synthesis and presentation of tools and strategies that can facilitate the process of obtaining informed consent from potential research participants living with deafblindness needs to be considered within the context of methodological constraints. Many of the reviewed procedures were developed by members of a team in Canada that has the benefit of collaborating closely with rehabilitation centers, funded by the provincial government, that provide specialized services to this population free of charge (Wittich et al., 2012). Such a network greatly improves the identification and recruitment process and may not easily be replicated elsewhere; however, we have also been able to benefit from similar collaborations in the Global South (Jaiswal et al., 2022a; Jaiswal et al., 2020b; Jaiswal & Gupta, 2016). Furthermore, adults living with deafblindness are a very heterogeneous population (Simcock, 2017; Wittich & Simcock, 2019). For example, older adults may have a congenital impairment in one sense (e.g., congenital cataract) and an acquired or age-related loss in the other (e.g., presbycusis). Both senses may be affected by a congenital condition, or by young- or working-age adult onset (e.g., Usher syndrome) or age-related causes (e.g., macular degeneration and noise-induce hearing loss). This heterogeneity requires a certain tolerance for variability, both in terms of the approach to data analysis, as well as for the design of appropriate research questions and the philosophical approach of the research team. A qualitative or a mixed-method study in the future would allow us to better understand how the different adaptations presented here influence the recruitment and consent experience from the perspectives of persons across this variety of lived experiences.
Given the projected increase in the global number of adults living with vision and/or hearing difficulties (World Health Organization, 2019, 2021), it is well worth the effort, however, to increase the capacity of researchers to include individuals living with sensory impairments. The adaptations and strategies presented here form a basis for such efforts by making the consent process easier and more inclusive. As a results, communication among all stakeholders is improved. Accessible consent procedures are necessary for persons living with deafblindness to understand the nature of the procedure, the risks, and the benefits involved. Researchers will be able to adhere to legal requirements when including this vulnerable population, thereby supporting their independence and dignity (Simcock & Wittich, 2019). In addition, institutional ethics review boards gain insight into the accessibility needs of participants living with deafblindness, providing them with information necessary to make informed decisions about the consent process. Given that everyone has the right to access information and participate in decision-making that affects their lives, facilitating this access will reduce social exclusion, discrimination, and power imbalances.
Footnotes
Acknowledgements
We would like to acknowledge the support of the clients and staff at the Centre de réadaptation Lethbridge-Layton-Mackay du centres intégrés universitaires de santé et de services sociauxdu Centre-Ouest-de-l’Île-de-Montréal, the Institut Nazareth et Louis-Braille du centres intégrés de santé et de services sociauxde la Montérégie-Centre, and Deafblind Ontario Services for their contribution to the development of the procedures presented here.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.