
Abstract
Background
There is a need to identify why multiple sclerosis exercise research is not translating into real-world participation. To lay the foundations of strong clinical research, considering the translational element of implementation science at the feasibility phase of a trial is vital.
Methods
Document analysis was used to examine document sources on exercise activity interventions designed for people living with multiple sclerosis. Document sources focused on multiple sclerosis research that incorporated exercise prescription elements and behaviour change and were feasibility studies incorporating aspects of implementation science.
Results
Implementation science should come much earlier than the efficacy or effectiveness research pipeline. An alternate view is outlined where feasibility and implementation science should meet based on case examples that have not yet shown strong efficacy or effectiveness. Findings from our key themes indicate a need for a cyclical iterative approach to the translational process. Multiple aspects of feasibility and how it can be assessed using an implementation science lens to support more successful interventions are provided. The determination of feasibility in behaviour change should involve implementation science as feasibility is drawn on for theory development, optimising the intervention design and quality of implementation strategies, and identifying those delivering the intervention before conducting efficacy and effectiveness research.
Conclusions
Document analysis methodology is underused in qualitative research and was appropriate to use as it was a very resource, time-efficient and an unobtrusive process that could track change and development to explore the integration of implementation science at the feasibility phase, with the findings indicating the earlier implementation science is introduced into multiple sclerosis exercise interventions the better.
Keywords
Background
Multiple sclerosis (MS) is a disorder of the central nervous system (CNS) characterised by neural inflammation and destruction of myelin tissue, resulting in CNS scaring and inefficient neural activity (Dobson & Giovannoni, 2019). Exercise interventions improve health outcomes in people living with MS and other neurological conditions, and exercise, a subset of physical activity, is considered the single most effective non-pharmacological symptomatic treatment for MS (Dalgas et al., 2019; Learmonth & Motl, 2021). Evidence from Randomised Controlled Trials (RCTs) has been evaluated, and guidelines for minimal levels of exercise for persons with mild to moderate disability resultant from MS are available (Kim et al., 2019; Latimer-Cheung, Pilutti, et al., 2013).
Yet, the evidence from exercise activity in MS RCTs does not translate to real-world activity increases. People living with MS are typically less active than the general population (Kinnett-Hopkins et al., 2017), and around one-quarter of persons with MS may not do any physical activity at all (Learmonth et al., 2022). Two decades of RCTs have indicated the multitude of benefits of exercise in MS, such as improvement in strength, physical fitness, walking performance, fatigue, balance, and quality of life (Motl & Pilutti, 2012; Motl et al., 2017). However, there is a need to identify why the research is not translating to real-world participation.
The concern of research findings not translating into real-world changes is being investigated from several perspectives (Rapport et al., 2018, 2021). In exercise and MS, one proposal is to include behaviour change theory in the design of exercise programs and exercise promotion (Motl, Pekmezi, & Wingo, 2018; Riemann-Lorenz et al., 2021). Another proposal identifies consumer barriers to exercise participation including environmental and personal barriers (Learmonth & Motl, 2016). Lastly, a recommendation on educating healthcare providers in the ongoing promotion of exercise in MS is being developed (Motl, Barstow, et al., 2018). However, one area lacking focus is the systematic study of research methodology that underpins exercise research in MS. This study must be undertaken as a priority to address the lack of MS exercise research translating into real-world participation (Riemann-Lorenz et al., 2021).
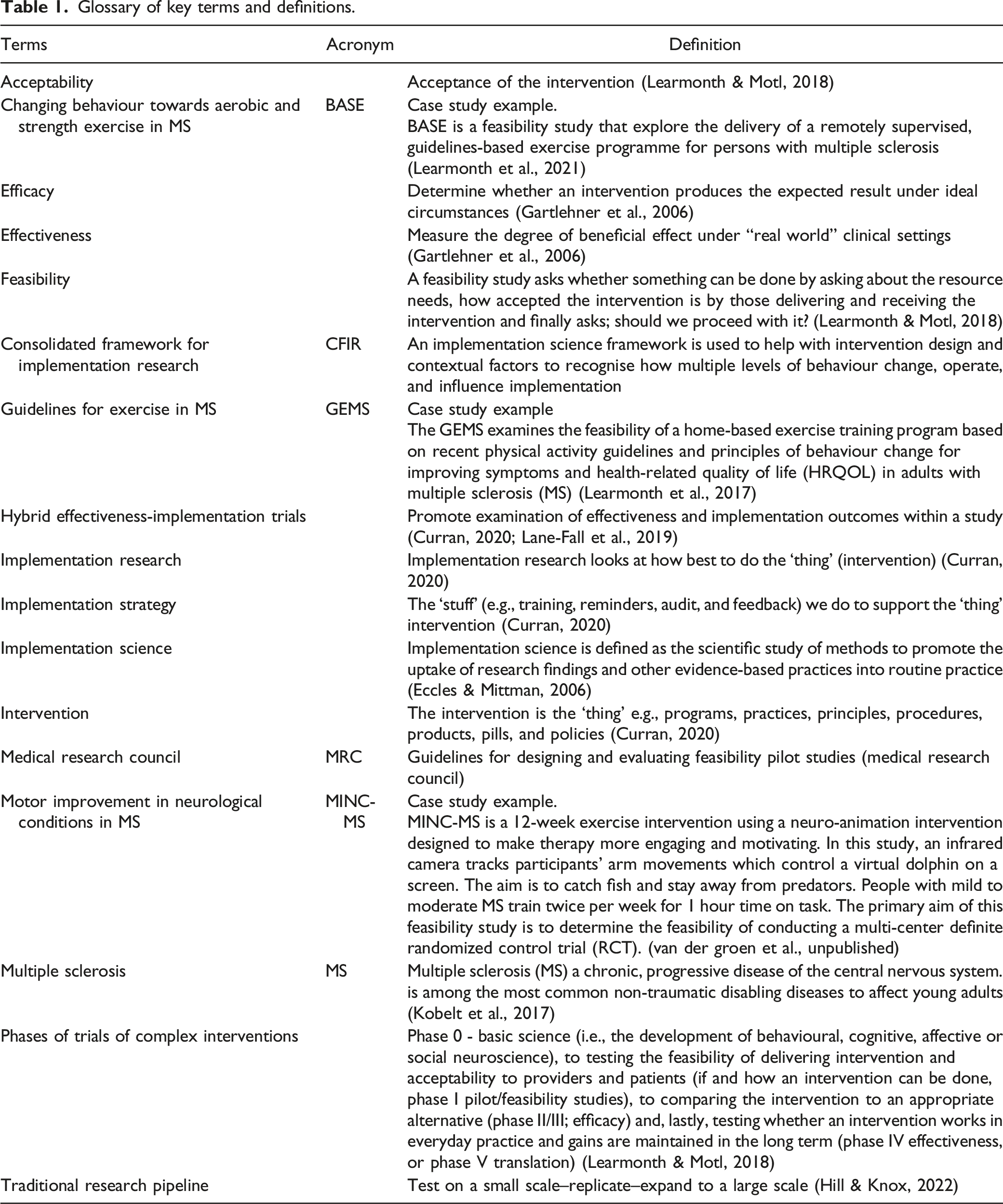
Implementation science is “the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice, and, hence, to improve the quality and effectiveness of health services and care” (Eccles & Mittman, 2006). We must consider the work of implementation science when considering the feasibility of MS exercise research. Building on implementation theories, models, frameworks and evaluation will allow refinement in the execution of research through implementation strategies to support and improve uptake of exercise and optimise their impact for people living with MS (Hallingberg et al., 2018). Our study lays the foundation for research on how feasibility from an implementation science lens can play an important role in addressing the valley of death, the phase between research and successful innovation (Hudson & Khazragui, 2013), and ensuring later implementation trials can be more translatable by acknowledging potential bottlenecks at the feasibility phase and before real-world environment research.
Feasibility plays an essential role in improving the conduct and quality of a RCT (Learmonth & Motl, 2018). Feasibility within the implementation science literature was initially conceptualised more than a decade ago as an important implementation outcome (Proctor et al., 2011). In this pivotal work, feasibility was highlighted as how a new treatment, innovation, or intervention can be successfully used or carried out (Proctor et al., 2011). Although, Proctor et al.’s (2011) framework has since been widely applied within the implementation science community, there is still a shortage of feasibility indicators within the implementation science literature (Pearson et al., 2020). In addition, there is a need to combine Proctor et al.’s (2011) framework of feasibility as an implementation outcome and position it within the broader feasibility literature (Hallingberg et al., 2018; Learmonth & Motl, 2018; Teresi et al., 2022).
A paradigm shift within implementation science happened with the introduction of a simultaneous assessment of effectiveness and implementation, described as Hybrid effectiveness-implementation trials. Hybrid effectiveness-implementation trials (Type 1, 2, 3) are used to distinguish between implementation and clinical trials (Curran et al., 2012; Lane-Fall et al., 2019). Hybrid effectiveness-implementation trials outlined in the literature have focused on real-world environment research which has shown effectiveness or at least very strong efficacy (Curran et al., 2012; Lane-Fall et al., 2019) and incorporate questions about implementation simultaneously into studies of effectiveness (i.e., Type 1) or simultaneously test the impact of one or more implementation strategies alongside the effectiveness of one or more interventions (i.e., Type 2) (Proctor et al., 2022).
Embedding feasibility and pilot studies within Type 1 and Type 2 effectiveness-implementation trials are worthy of attention. However, despite the methodological advances of hybrid designs this does not resolve the fact that the effects of implementation strategies have only ever been modest (Lewis et al., 2018; McIntyre et al., 2020; Pearson et al., 2020; Powell et al., 2011; Powell et al., 2015). To improve the effectiveness of implementation strategies and improve the uptake of exercise in real-world participation, we turn to the broader feasibility literature (process, resource, and management) together with implementation science for answers.
Glossary of key terms and definitions.
Methods
Ethics approval and consent to participate was not applicable to our study. Conducting a document analysis has been documented to eliminate some of the ethical concerns associated with other qualitative methods (Morgan, 2022). For example, document analysis is a form of qualitative research whereby the researchers understand the actual documents to give voice and meaning through the analysis of the documents (Bathmanathan et al., 2018). Document analysis can include peer-reviewed, grey literature or a combination of both, as such, sourcing and selecting documents used for systematic evaluation in our particular study are presented in the form of peer-reviewed published or unpublished documents (Adamson et al., 2016; Learmonth et al., 2017; Learmonth et al., 2021; van der Groen, Learmonth, van Rijn, Smith, and Edwards, Unpublished). The analytic procedure entails appraising, and synthesising data contained in documents by coding text into themes and subthemes (Bathmanathan et al., 2018). Our study also adheres to the consolidated criteria for reporting qualitative research (COREQ) (Tong et al., 2007) reporting guidelines.
Document Sources
Case Study research on a range of feasibility studies critically examined.

Analysis
The case examples we draw upon are considered together by using document analysis methodology combined with other methods such as the One Sheet of Paper (OSOP) method (Ziebland & McPherson, 2006) that summarises data. In addition, we present a simplified account of the data through a visual qualitative mapping method (VQMM) (Smith, Lee, Ellis, Ijaz, & Yin, 2021) to facilitate an understanding of our qualitative results (See Figure 1). This process was supported by NVivo 12 Plus (QSR, 2019). Displaying the data
Table of Results.
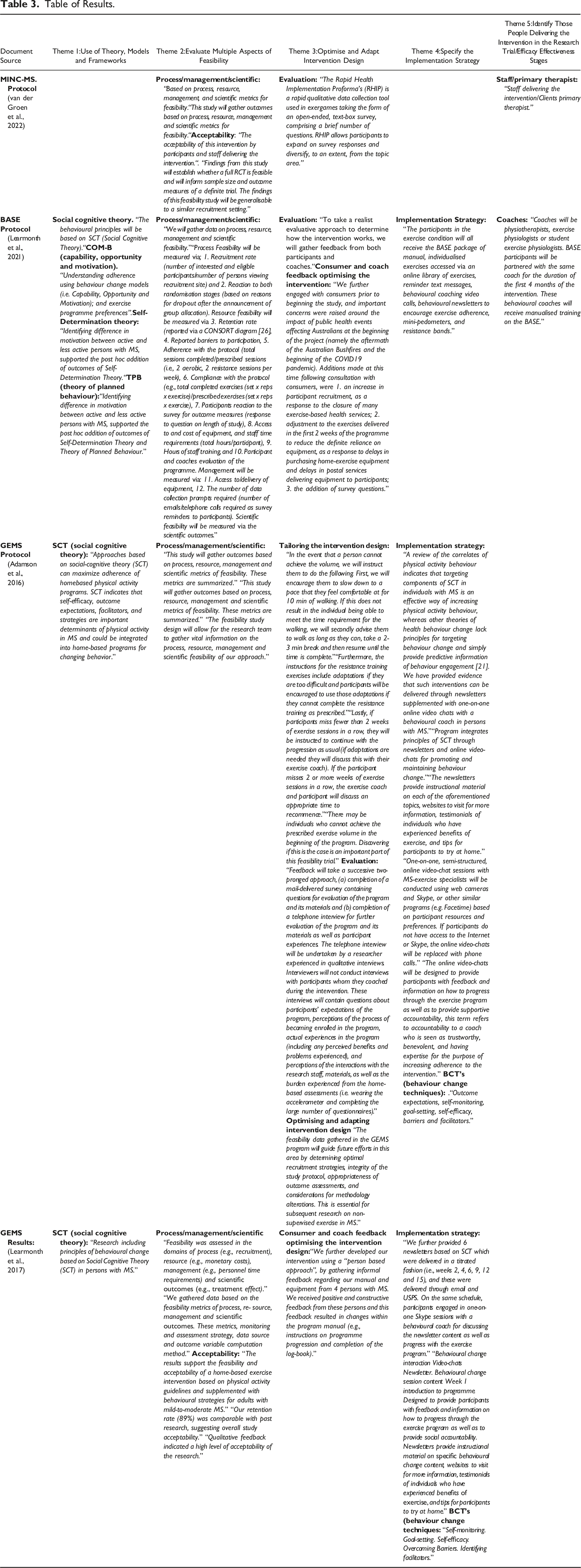
Results
Five Themes
Summarising results by using a matrix to show how an implementation science lens can complement feasibility studies based on MS document sources.

Visually displaying results combining the OSOP and VQMM.

Key.
X = Implementation science gaps.
✓ = Implementation science aspects identified.
Our evidence from the document sources demonstrates how some aspects of implementation science are already being integrated much earlier at the feasibility phase in MS (Phase I) research, rather than implementation science assumed to only start at phases of strong efficacy or effectiveness (e.g., Phase II/III testing). By using implementation science at the feasibility phase (Phase I), some barriers are pre-identified, anticipated, and understood before subsequent strong efficacy (Phase II/III), and effectiveness research (Phase IV). Such practice could improve the on-going fit and quality of implementation strategies, an important finding based on real-world case study examples in MS and exercise that are yet to establish strong efficacy or effectiveness (Adamson et al., 2016; Learmonth et al., 2017; Learmonth et al., 2021; van der Groen et al., Unpublished).
Discussion
We document case examples to map and develop the idea of a cyclical model (Hill & Knox, 2022; Knox et al., 2018) providing real-world needs outlined by our document sources, highlighting where feasibility meets implementation science. We herald that in health conditions such as MS, the benefits of participation in exercise are vital for symptom management, and may offer much benefit to the disease progression, yet exercise participation is still low within this population (Marck et al., 2020). Our proposed cyclical model of feasibility and implementation science outlined below may offer an important sea change. Our findings, therefore, present a critical step in preliminary testing of the intervention design, delivery, and implementation strategies and methods. There are five clear themes that have been visually represented as an alternative qualitative approach that offer actionable guidance to future studies (Pfaff & Schmitt, 2021). Via case examples of exercise research in MS, we have shown a comprehensive picture of the interaction between testing clinical feasibility and adopting principles of implementation science that can be harnessed together when testing research for clinical practice.
Theme 1: Include the use of Theory, Models, and Frameworks
Theory is often underused, however, determinant frameworks, classic theories, implementation theories, and evaluation can all help to guide implementation practice (Birken et al., 2017; May, 2013). Theories therefore, describe aspects that might be important to evaluate (May, 2013; Nilsen, 2015). This is because a good theory explains how and why specific relationships lead to particular events and therefore how the implementation strategies are thought to work and sustain interventions (Albers et al., 2020; Rapport et al., 2022). Across the case studies, of BASE and GEMS a mixture of different classic behavioural theories were being considered and tested, such as the use of Self-Determination Theory, Theory of Planned Behaviour (individuals attitude, subjective norms, and perceived behavioural control) and Social Cognitive Theory (reciprocal determinism, behavioural capability, expectations, observational learning, reinforcements, and self-efficacy – seen as the most personal factor in changing behaviour) were used (Adamson et al., 2016; Learmonth et al., 2017; Learmonth et al., 2021). Other examples of behavioural theories can be seen in BASE with the COM-B, (capability and/or opportunity and motivation - as three key factors capable of changing behaviour) (Learmonth et al., 2021) that can help explain behaviour change in adopting exercise behaviour for those persons living with MS as they can target correlates of physical activity behaviour and consider the demands of living with MS. Further, in the BASE document source (Learmonth et al., 2021) the importance of including a realist theory approach (Brockschmidt & Wadey, 2022) to programme implementation (a theory that explains how and why particular types of interventions work to generate the outcome/s of interest) was indicated. This can help explain “how the intervention works”, “why does the intervention work”, how strategies bring about intended or unintended results, “for whom does it work” and “in what circumstances does it work” (Pawson et al., 2005).
Theme 2: Evaluate multiple aspects of feasibility
Multiple feasibility aspects from our case examples relate to process, resource, management and scientific outcomes (Adamson et al., 2016; Learmonth et al., 2017; Learmonth et al., 2021; van der Groen et al., Unpublished). These feasibility metrics are invaluable to Phase II or Phase III (Campbell et al., 2000; Friedman et al., 2015). For example, resource feasibility measures the training need and competence of personnel delivering the intervention. Poor training or low competence of personnel may impact the results of the intervention (Chen et al., 2022; Tickle-Degnen, 2013). Further, management feasibility addresses staff time commitments, providing vital information for policy-makers when weighing up which interventions to consider for future research relevant for clinical practice, and this information could further contribute to understanding intervention fidelity (Smith, Braithwaite, O'Brien, Smith, Tyrell, et al., 2022). There is urgency needed in establishing the goals of preliminary studies as research funding applications are assessed based on a varied list of standards which may lack consistency. In addition, the people intended to deliver and receive the intervention need to accept that intervention, if there is low acceptability, it could have an overall effect on the intervention (Smith, Braithwaite, O'Brien, Smith, Tyrell, et al., 2022). Acceptability is, therefore, an important aspect of feasibility (Learmonth et al., 2017; van der Groen et al., Unpublished), and if acceptability is ignored at the Feasibility phase (Learmonth & Motl, 2018), we miss a variety of opportunities to inform later phases of efficacy and effectiveness (Smith et al., 2022).
Individual concepts such as feasibility and acceptability are therefore necessary but insufficient on their own (Klaic et al., 2022). Our findings align with the guidelines that state we must assess multiple aspects of feasibility such as acceptability, intervention design, delivery refinement, optimisation, and modifications before full-scale evaluation (Craig et al., 2008; Teresi et al., 2022). MRC guidelines in 2008 (Craig et al., 2008) and other studies (Learmonth & Motl, 2018) also advocate for this cyclical approach whereby movement between piloting/feasibility and intervention development may sometimes be needed when changes to intervention design may be necessary (Hill & Knox, 2022). The idea of assessing multiple aspects of feasibility (Bowen et al., 2009; Craig et al., 2008; Medical Research Council), has recently been updated and advocated within the latest guidelines (Teresi et al., 2022).
Theme 3: Optimise and adapt the intervention design
Involving consumer and coach feedback, optimising and tailoring the intervention design, and evaluation were subthemes presented to describe the overall theme, which is to optimise and adapt the intervention design. Such a guideline-driven approach to consumer review is critical to understand clinical uptake of our exercise interventions. The intervention design and the fit of the intervention into settings should be considered at the feasibility phase (Craig et al., 2008). This is in line with the MRC guidelines for a full evaluation, where the evaluation is an RCT (Medical Research Council; O’Cathain et al., 2015) together with more recent guidelines advocating, as already discussed, for assessing multiple aspects of feasibility (Teresi et al., 2022), suggesting implementation science can play a central role. We should question why studies would design interventions that ultimately do not fit the context to which they will need to be applied (Chambers et al., 2013; Smith et al., 2020), and ask does implementation science hold the promise of unpacking the link between context and outcomes (Rees et al., 2022) as highlighted with the use of a realist approach in the feasibility study of BASE (Learmonth et al., 2021). Therefore, adaption and tailoring to context should be considered early and in terms of how we ensure that the intervention will fit the context of its intended setting, group, or population. The opportunity therefore lies in designing the best possible intervention at the start (feasibility Phase 1). Doing so will help later phases, by identifying early on the determinants of current behaviour and desired behaviour change which can help in the selection of the components of the implementation strategies that can target key determinants, therefore, minimise the risk of replicating these barriers when scaling the intervention across sites or scaling across healthcare systems. Implementation Science Frameworks such as the Consolidated Framework For Implementation Research (CFIR) are useful, because this framework considers how an intervention is designed will affect how well it can be implemented (Damschroder et al., 2009). On author reflection, our study highlights something missing within our case examples that included more thought over intervention design considerations using implementation science frameworks to guide intervention design optimisation, and therefore this too needs to be employed in feasibility studies (Chambers et al., 2013). In addition, the intervention characteristics of the CFIR (i.e., intervention source complexity, adaptability, relative advantage, trialability) will inherently complement the feasibility phase of intervention design (Landes et al., 2019) because, by the time you reach past this stage, it potentially is too difficult, or too late (fixed in effectiveness research) to change, adapt or optimise a working intervention. For feasibility, identifying enablers to achieve on-going optimal trial design is a worthwhile goal (Smith, Braithwaite, O'Brien, Smith, Tyrrell, et al., 2022). Rich information on barriers and facilitators to research implementation can be used to modify the trial before testing efficacy and effectiveness and this can also become an iterative process. Collecting such data at the outset of our research goals allows us to implement the principles of behaviour change into our scientific research pursuits. Therefore, we are armed with knowledge about contextual fit, and the barriers and facilitators at the early feasibility phase and can be proactive rather than reactive later down the line (as in efficacy and effectiveness studies) (Chambers et al., 2013).
Theme 4: Specify the Implementation Strategies Within the Feasibility Study
Implementation strategies are defined as “methods or techniques used to enhance the adoption, implementation, and sustainability of a clinical program or practice” (Curran et al., 2012; Proctor et al., 2013, p. Pp. 140). Despite the rapid rise of implementation science as a discipline (Sales et al., 2019), the quality of implementation trials has been criticised and the effects of implementation strategies on implementation have only been modest (Grimshaw et al., 2004; Lewis et al., 2018; Powell et al., 2015). The reasons for this have seldomly been reported and are poorly understood (McIntyre et al., 2020). Herein we present the view that designing implementation strategies can be optimised within feasibility studies in preparation for an RCT. The feasibility phase is a missed opportunity not to align implementation strategies with implementation outcomes (e.g., feasibility and acceptability) and work towards early optimisation of the intervention (Rudd et al., 2020). The implementation strategies in the MS context based on our document sources are the strategies (reminders, education etc.) used to support the uptake of the exercise intervention (Curran, 2020; Smith et al., 2022). To effectively engage in implementation science research, it is a pre-requisite to understand the role of behaviour change in developing an implementation strategy (Handley et al., 2016). Our document sources provide clear evidence that implementation strategies for studies that have yet to establish efficacy or effectiveness hold the key to early optimisation generating useful knowledge that can be used across the translational process for the utility and application of implementation strategies to support the intervention (McHugh et al., 2018). Theme 1 (theory) and Theme 4 (implementation strategy) are interlinked. This is because the use of theory such as Social Cognitive Theory (SCT), and Behaviour Change Techniques (BCT’s) used in the document sources structure understanding of barriers and can help to develop implementation strategies in this pre-efficacy phase, providing an emerging approach at the intersection of feasibility and implementation science. It is argued here that designing for implementation and testing effects on implementation strategies can be considered as an important additional feasibility aspect that should not be ignored, since this offers foundational knowledge that could help across each phase of the research translational process (Craig et al., 2008). Further work could specify the implementation strategy in more detail. For example, if the intervention is attempting to get people to engage in exercise behaviour, consideration of the implementation strategies would be to ask, what further education or instruction is needed for recipients of the intervention? What do recipients of the intervention need to know concerning the intervention (i.e., if telehealth, access to the equipment; if an aerobic/strength programme access to equipment)? How long or how often should they exercise (dose/fidelity), or how much support should be provided? What economic considerations influence the use of implementation strategies to deliver the intervention? Knowing this information will facilitate identifying what the barriers are to making this intervention happen. If Theme 4 (implementation strategy) is considered within feasibility studies that have yet to establish efficacy, one would need to consider our next theme on those intended to deliver the intervention long-term since by now, one would have gained prior knowledge of the barriers as well as facilitators for those delivering and receiving the intervention that could be passed onto those intended to deliver the intervention (e.g., identifying possible training needs of clinicians/research staff to deliver the program) for efficacy or effectiveness phases (see Theme 5). This also leads to better estimates of the costs involved for running a RCT. For example, when training needs are identified, these costs have to get covered by for example a research grant. These items can thus be added to the study budget.
Theme 5: Identify Those People Delivering the Intervention in the Research Trial/Efficacy Effectiveness/Hybrid Stages?
The case examples show that staff/primary therapists were identified in the MINC trial and coaches (physiotherapists, exercise physiologists student exercise physiologists) in BASE suggesting evidence over how, by who and for whom. However, often within research feasibility trials, key propositions are not identified, or identified for use within later Phase II or III or are identified and not being documented (e.g., in GEMS ‘the who’ was postgraduate and postdoctoral exercise scientists and physiotherapists who were delivering the intervention, yet this is not documented within the actual protocol or results papers) (Learmonth et al., 2017). Equally important is to consider what skills and qualifications are needed to deliver the intervention to recipients of the intervention? Not collecting this data is also a lost opportunity. Yet again, within research trials, this is seldom documented or part of this process. Typical of most interventions at the feasibility phase, intervention designers do not anticipate or provide clear specification of who the intended people are to deliver the intervention and sustain it over time in real-world settings. Still, literally, these people may not even exist within the system that the intervention is intended to be provided. If groups or individuals to deliver the intervention do not exist in the system that we intend it to go, how is a research study considered feasible at this phase?
It is clear from the above, as people adopt exercise behaviour for rehabilitation, we gain more information on the types of barriers and facilitators that follow. This is critical information because by specifying and operationalising how the implementation strategies should look like and what they should include (Theme 4), we can subsequently move towards who delivers it (Theme 5). For who ultimately delivers these implementation strategies in RCT or effectiveness studies, we also ensure for whom they will be delivered (Knox et al., 2018). By applying our themed findings from the current case studies (See Case Studies Table 1), implementation science clearly has a critical role in feasibility research because we could improve current feasibility research by helping to map out those individuals who could ultimately take on these roles (Chambers, 2012; Presseau et al., 2019; Wandersman et al., 2008) and this could further inform later phases (efficacy and effectiveness). Hence, we could optimise this aspect within feasibility studies before leading to efficacy and effectiveness where continued optimisation may ensue.
Our new model view, shown in Figure 2, builds the necessary scaffolding around the use of feasibility of a study from an implementation science lens and opens up and extends the idea of an iterative cyclical approach toward implementation science within feasibility studies to improve results later on (i.e., better choices over implementation strategy and therefore better results later on) (Davies et al., 2010). Proposing a cyclical model on where feasibility meets implementation science to improve translating and implementing evidence into practice.
Evidence indicates that researchers face a myriad of challenges translating the benefits of exercise in MS identified in clinical trials into increased physical activity and exercise participation. These challenges may stem from the methodological design. Our presented findings on theories, models and frameworks, combined with acceptability, feasibility, from the implementation science field at the feasibility phase can be used to improve effective translation in MS exercise interventions (Learmonth & Motl, 2018; Rapport et al., 2022). Our study is timely and provides a wider applicability by providing a roadmap to MS studies that are having to alter, adapt and optimise intervention designs amid on-going change such as a result of external factors as with the COVID-19 pandemic (Chambers, 2020; Sandroff et al., 2021; van der Groen et al., Unpublished).
Our findings represent a cyclical iterative approach (Hill & Knox, 2022; Knox et al., 2018), where we can learn about the possible implementation challenges at the feasibility phase and optimise the intervention throughout the translational process. We provide clarity for studies across the translational process by considering multiple case examples using different document sources highlighting where feasibility meets implementation science for studies that are yet to show strong efficacy or effectiveness. One limitation of our study is that guidelines on document analysis methodology is scant because document analysis is an underused qualitative methodology (Morgan, 2022). However, document analysis methodology and the use of standalone documents sourced (peer-reviewed published and unpublished documents) are very reliable data sources, and this was a far more cost-effective and time-efficient and unobtrusive process that could track change and development (Bathmanathan et al., 2018; Morgan, 2022). Document analysis can capture where feasibility meets implementation science in ways that other qualitative methods may not be able to. We highlight the use of the integration of implementation strategies and optimisation processes at the feasibility phase (and beyond), showing how our documents sources reveal this practice, although our case examples have yet to show strong efficacy or effectiveness. We also presented critical reflection to describe where feasibility meets implementation science amid on-going change. This further allowed for clarity related to the opportunities and challenges faced, including the foundations of implementation science in multiple areas of feasibility studies. The premise of this paper was that if the intervention has not yet shown strong efficacy or effectiveness, feasibility studies should be employed, and the earlier implementation science is introduced the better. The well-constructed implementation of behaviour change will improve real-world practice (Campbell et al., 2000; Friedman et al., 2015; Learmonth & Motl, 2018). Therefore, the development of solutions on how implementation science can complement feasibility studies is sorely needed within the translational process literature and how this can improve the quality of implementation strategies (how to effectively implement and sustain those interventions) in effectiveness research, potentially answering the question to why MS exercise research is currently not translating to real-world participation.
Conclusion
To maintain clarity in research translation within exercise and MS, we need to understand the intersection between feasibility and implementation science outlined here in terms of the need of theory, models, frameworks, acceptability, implementation strategies and evaluation. These crucial aspects highlighted in our document sources also clearly identified the importance of gaining prior knowledge of the barriers as well as facilitators for those delivering the intervention that could be passed onto those intended to deliver the intervention long-term in real-world practice across different settings and systems. Hence, our key message is that there is potential for an iterative process whereby feasibility studies help us learn about refining implementation strategies and, optimise and adapt aspects so that we can harness all of this prior knowledge to influence later phases with the continued importance to on-going development optimisation and adaption to diverse populations and systems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funding received from the Multiple Sclerosis Society of Western Australia (MSWA) with YCL funded through a Multiple Sclerosis Australia Fellowship.